AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2578-8949/004
*Corresponding Author: Landon Owen, Department of Dermatology, France.
Citation: Jonathan Noah, Benjamin Dylan, Landon Owen, An Infection of Acrodermatitis Chronica Atrophicans Herxheimer by Borrelia Affzelii J .Dermatology and Dermatitis. Doi: 10.31579/2578-8949/004
Copyright: © 2017 Lénaïg Halos. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 March 2017 | Accepted: 26 March 2017 | Published: 30 March 2017
Keywords: acrodermatitis chronic atrophicans herxheimer; borreliosis; cutaneous manifestations; treatment
Acrodermatitis Chronica Atrophicans Herxheimer (ACA) is a tick-born disease due to infection by Borrelia afzelii, the major vector organism is Ixodes rhicinus. We report on a 48-year-old male patient who developed extensive livid-erythematous fibrosclerotic symmetric plaques associated with hyperpigmented widely distributed lesions within the tension lines, and acrocyanosis. The diagnosis of ACA has been confirmed by histopathologic examination of a skin biopsy and laboratory investigations with positive IgG and IgM immunoblots. The patient was treated by intravenous ceftriaxone resulting in partial remission of cutaneous and extracutaneous symptoms.
Acrodermatitis Chronica Atrophicans Herxheimer (ACA) is a tick-born disease that has initially been described 1902 by Herxheimer. The disease is a late manifestation of infection in most cases by Borrelia afzelii, although B. garinii and Bb sensu strictu have been isolated in a few cases. In Germany the major vector organism is Ixodes rhicinus. The disease starts with an edematous early stage with livid erythema. Here the number of differential diagnoses is large and covers such different disorders like chronic venous insufficiency with stasis dermatitis, myxedema, dermatoliposclerosis, and scleroderma [1, 2].
In about 6% of patients a pseudoscleroderma can develop due to increased collagen synthesis. These patients are characterized by high levels of IgG antibodies against Borrelia afzelii [Hofmann 2005]. In the late, atrophic stage, there is a marked epidermal, dermal, and subcutaneous adipose tissue atrophy with pronounced wrinkling (cigarette paper-like) with venous show. Extracutaneous symptoms include arthralgia, allodynia, peripheral polyneuropathy. The latter may lead to neurogenic ulcers [3].
Diagnosis of ACA is confirmed by medical history, clinical examination, histopathology, and laboratory investigations. Sensitivity and specificity of enzyme immuno assay and immune blot are 95% and 80-95% for ACA [4]. Polymerase chain reaction (PCR) of skin biopsies was positive in up to 88% on fresh-frozen tissue but only in 44-52% using paraffin-embedded tissue [5].
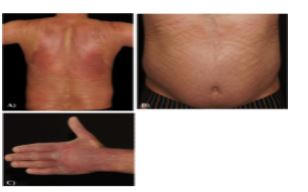
A 48-year-old male patient was referred to our hospital because of large livid-erythematous fibrosclerotic plaques on his trunk and extremities which developed within half a year. He suffered from arterial hypertension and had a penicillin allergy. He had no memory of any tick bite.
On examination we observed symmetric large lividerythematous fibrosclerotic plaques on his upper back. Erythematous to brownish lesions along the tension lines of skin were found on the lower back, abdominal, on the shoulders and proximal extremities. On this hands, a livid erythema was noted. During inspiration the lower thoracic aperture had a decreased elongation. On the hands there was an incomplete fist circuit notable. No other clinical symptoms were noted.
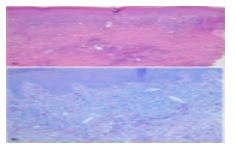
We performed a skin biopsy. Histologic evaluation disclosed dermal changes including broadened and homogenized collagen bundles, perivascular and periadnexal lymphocytic infiltrate with some mast cells and plasma cells intermingled. PCR for Borrelia remained negative.
Laboratory investigations
Leukocytes 12.4 (normal range: 3.8-11.0 Gpt/l); neutrophils 9.4 (1.8-7.6 Gpt/l); C-reactive protein 17.6 (< 5 mg/dl); total IgE 269 (0-100kU/l); rheumatoid factor 38 (< 14 IU/ml); Borrelia IgG-antibodies [Enzyme immune assay] >200 (<16 RE/ml), IgM-antibodies 19.2 (<16 RE/ml), IgG-immunoblot: positive; IgM-immunoblot positive; serum albumin 47.6 (60,3-71,4 %), Ý-globulin 30.0 (8.7-16.0 %). Antinuclear antibodies (ANA) and antibodies against extractable nuclear antigens (ENA): negative.
Ultrasound - neck, axillaries, groins, abdomen - unremarkable. Thoracic X-ray and body plethysmography - unremarkable. Electrocardiography: indifferent type, heart beat frequency 79/ min.
Based on clinical examination, histopathology and serologic investigations the diagnosis of ACA, edematous stage, was confirmed.
Because of the penicillin allergy we treated the patient with intravenous ceftriaxone 2g once daily for 10 days. We combined this with topical steroids, bath-PUVA (Psoralen Plus UVA-irradiation), and complex physio- and ergotherapy. The latter consisted of manual lymph drainage, respiratory therapy, relaxation, and motoric-functional treatment of both hands.
We achieved a partial response with improved motoric ability of the hands. The skin became more softened, erythema vanished, and fibrosis improved.
ACA is a tick-borne disease with progressive course. In the adult European population 1-2% of Borreliosis develop ACA [2], among children ACA was observed in about 1% [6]. The clinical presentation may vary. Extracutaneous manifestations are common among our patients [7]. Cutaneous manifestations cover a broad spectrum. Unusual symptoms include chronic venous insufficiency [8], vasculitis racemosa [9], morphea- and lichensclerosus- like lesions [10], anetoderma [11], juxta-articular nodules [12], small spinous papules [13], foot ulcers [3], and alopecia [14]. A very rare manifestation is facial involvement [15, 16].
Our patient was quite unusual related to cutaneous manifestations. Hyperpigmented lesions along the tension lines of skin and extensive livid-erythematous fibrosclerotic plaques are ambiguous. Only the livid erythema of the hands was a classical presentation. Serologic investigations and histopathology of a skin biopsy, however, confirmed ACA.
Early antibiosis is important to prevent the progress of ACA to an atrophic stage. Intravenous treatment is possible with ceftriaxone, cefotaxime, or penicillin G [17]. We used ceftriaxone since the patient had a penicillin allergy.
ACA remains a diagnostic challenge, this has been illustrated by our patient.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.
















































