
Research Article | DOI: https://doi.org/10.31579/2692-9562/128
1 Master's student of the Postgraduate Course in Health Sciences at PUC-Campinas. Head and Neck Surgery at PUC-Campinas Hospital, Brazil.
2 Advisor Professor of the Graduate Course in Health Sciences at PUC-Campinas. Head and Neck Surgery at PUC-Campinas Hospital, Brazil.
3 Head and Neck Surgery at São Leopoldo Mandic, Brazil.
4 Head and Neck Surgery at PUC-Campinas Hospital, Brazil.
5 Head and Neck Surgery at PUC-Campinas Hospital, Brazil.
*Corresponding Author: Thalita Ruba Carpanezi Barbosa, Master's student of the Postgraduate Course in Health Sciences at PUC-Campinas. Head and Neck Surgery at PUC-Campinas Hospital, Brazil.
Citation: Carpanezi Barbosa TR, José Luis B De Aquino, De Sales Chagas JF, Brandi Filho LA, Rizzantti Pereira DA, (2024), Voice Rehabilitation with Tracheoesophageal Prosthesis in Patients Submitted to Total Laryngectomy: Qualitative and Quantitative Evaluation of Global Quality of Life, Journal of Clinical Otorhinolaryngology, 6(5); DOI:10.31579/2692-9562/128
Copyright: © 2024, Thalita Ruba Carpanezi Barbosa. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 02 July 2024 | Accepted: 24 September 2024 | Published: 07 October 2024
Keywords: laryngeal neoplasms; artificial larynx; rehabilitation; voice prosthesis; quality of life
Introduction: Laryngeal cancer is a prevalent disease and represents 25% of all head and neck malignancies. One of the treatments is total laryngectomy, which is a surgery with an important impact on the quality of life of patients. Within the different forms of vocal rehabilitation, the voice prosthesis stands out.
Aim: To evaluate vocal rehabilitation and global quality of life in patients submitted to total laryngectomy for laryngeal squamous cell carcinoma, with placement of a tracheoesophageal prosthesis.
Materials and Methods: Two questionnaires were applied to total laryngectomized patients from January 2002 to July 2022. Questionnaire 1 was the voice quality of life protocol. Patients with a score greater than 50 were classified in the group of rehabilitated patients, and those with a score less than or equal to 50, in the group of non-rehabilitated patients. Questionnaire 2 is the University of Washington Quality of Life Questionnaire. Patients in the rehabilitated and non-rehabilitated groups were compared with their relevant scores as defined by validated questionnaires.
Results: Thirteen patients were interviewed. In questionnaire 1; an average score of 71.54, ranging from 20 to 100, was observed with a standard deviation of 26.47. In questionnaire 2, an average score of 79.78, ranging from 55.5 to 94.5 was observed.
Conclusion: Rehabilitation of total laryngectomized patients with voice prosthesis proved to be a reproducible method with few complications. There was an improvement in quality of life after treatment, with good to excellent quality of life in most patients.
World annual head and neck malignancies affect about 888,000 individuals, causing more than 453,000 deaths [1]. According to the Brazilian National Cancer Institute (INCA), laryngeal cancer represents 2% of all malignant tumors of the body and 25% of head and neck malignancies [2]. In Brazil, the estimated number of new annual cases of laryngeal cancer for the three-year period 2023-2025, is 6,570 in men and 1,220 in women [3].
Laryngeal tumors mainly affect male patients, between 50 and 70 years of age, most of them smokers and alcoholics [2]. The most prevalent histological cancer type includes squamous cell carcinoma, confirmed in more than 90% of cases [4].
Depending on the oncological staging, the treatment may be clinical, using associated or exclusive radiotherapy, or surgery in more advanced cases [5]. Surgical removal of the larynx can offer a curative approach for patients with advanced larynx and hypopharynx cancer without distant metastases [6]. The surgical techniques used are total laryngeal resection with definitive terminal tracheostomy or tumor exeresis with safety margin and reconstruction of a functional neolarynx [4]. According to the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology, total laryngectomy remains the standard treatment for T3 and T2-T4a laryngeal squamous cell carcinoma of the hypopharynx [7]. Due to the negative impact on the quality of life (QoL) of patients submitted to total laryngectomy, such as loss of voice, difficulty in communication and permanent presence of the tracheostomy, more conservative treatments have been proposed, with partial preservation of the organ: conservative surgeries [8], radiotherapy followed by surgery, exclusive radiotherapy and exclusive chemoradiotherapy [6]. Speech rehabilitation in patients submitted to total laryngectomy has been a continuous concern over the years. Currently, for the rehabilitation of totally laryngectomized patients, three forms are available: the esophageal voice, the electronic larynx and the Voice Prostheses (VP) [9]. VP is the most recently developed method for vocal rehabilitation of totally laryngectomized patients, and the prosthesis can be placed surgically or endoscopically [10]. Phonation through VP has the advantage of being functionally achieved through a few sessions of guidance and vocal refinement with the help of a speech therapist; it is a great option for patients who cannot develop an esophageal voice [6]. Moreover, compared with the electronic larynx and the esophageal voice, the VP stands out, as the patients develop an acceptable voice, with success rates around 90% [11]. VP represents the gold standard for voice restoration after total laryngectomy, improving patients’ QoL after surgery [12]. The first report on tracheoesophageal fistula with placement of a valve VP was released by Singer and Blom in 1978 [13]. The VP is a small tube made of antiallergic silicone material, which is inserted into a hole surgically made in the common wall that separates the trachea and the esophagus, creating a fistula at the level of the tracheostomy [14]. As the patient occludes the tracheostomy, air from the lungs is forced through a one-way valve of the VP, causing the pharyngoesophageal segment to vibrate. The vibration penetrates the oral cavity and the buccal articulation creates speech. The small valve VP allows the flow of air from the trachea to the esophagus and prevents the passage of liquids and food from the esophagus to the trachea [15].
Total laryngectomy is a mutilating surgery [16], and its anatomical and physiological changes can lead the patient to frequent chronic pain, socio-emotional changes and psychological disorders; these drawbacks have an important influence on the QoL of both the patients and their family [17]; the impact is mainly due to the hampering of communication caused by the total loss of the vocal cords [18]. At the Head and Neck Surgery Service of the Hospital PUC-Campinas, the evolution of cases of total laryngectomized patients using VP was monitored. There are cases of groups of people who underwent vocal rehabilitation and other groups without rehabilitation leading each patient to an individualized and unique QoL. From this observation, this work emerged requiring further investigation of these patients. This study was aimed at analyzing and quantifying the QoL of total laryngectomized patients who are using a VP, in connection with their vocal rehabilitation.
This study aims to evaluate the vocal rehabilitation and global QoL of patients submitted to total laryngectomy for laryngeal squamous cell carcinoma, and with VP placement.
This is a descriptive observational study, based on the medical records of patients who underwent total laryngectomy and VP placement, at the Head and Neck Surgery Service of Hospital PUC-Campinas; the survey sample included all patients monitored during the period January 2002 to July 2022 in this service and who met the following stipulated criteria [19], which totaled 13 patients.
Inclusion criteria
1. Patients with insertion of VP after total laryngectomy for larynx squamous cell carcinoma.
2. Free of disease at the time of the interview.
3. Agreeing with the investigation by signing an informed consent form.
4. Minimum 6 months postoperative time with the use of VP.
5. Having been submitted to adjuvant radiotherapy.
6. Having been submitted to bilateral neck dissection.
Exclusion criteria
This study was approved by the Human Ethics Committee of PUC-Campinas, on May 4, 2022 under number CAAE: 50729121.7.0000.5481. The patients were followed up by a team of speech therapists and physicians from the Head and Neck Surgery Service at Hospital PUC-Campinas. General aspects such as gender, age, comorbidities, date of surgery, preoperative staging, adjuvant treatment, period of cancer treatment and rehabilitation were examined in the medical records (19). Patients who met the inclusion criteria were interviewed face-to-face, after a previously scheduled routine appointment for periodic outpatient VP replacement. All patients used the same VP brand and model: Provox Vega by Atos.
In the interview, the patient was informed about the survey he would be a participant. All questions were clarified, and the patient was asked to sign an informed consent form. Subsequently, two questionnaires were applied.
Questionnaire 1 is the Voice-related Quality of Life. (V-RQOL) protocol (Appendix 1) in its version validated for Brazilian Portuguese by Gasparini and Behlau (19). This questionnaire constitutes a self-assessment of personal satisfaction regarding the vocal rehabilitation method used, and helped classify patients into either the group of rehabilitated patients (G1) or the group of non-rehabilitated patients (G2). In line with the literature patients evaluated themselves answering several questions regarding vocal rehabilitation. The questionnaire uses a 5-cm analogue-visual scale where 1 (one) means “very satisfied” and 5 means “very dissatisfied”. The V-RQOL lists potential voice-related problems, consisting of ten questions to be answered taking into account the severity of any problem and the frequency in which it occurred in the last two weeks before the interview. The value of the total V-RQOL score was calculated using the formula: Total = 100 – [(raw score – 10) / 40] x 100, with the raw score being the sum of the responses to the questions. The maximum score is 100 (best vocal quality), and the minimum score is zero (worst vocal quality). In this investigation, patients with a score greater than 50 were considered rehabilitated, and patients with a score lower than or equal to 50 were considered not rehabilitated; patients were then classified into groups G1 and G2 respectively.
Questionnaire 2 that was used to assess specific QoL in the postoperative period of head and neck surgery is the University of Washington in Seattle Questionnaire (UW- QOL) (Appendix 2), developed by Ernest A. Weymuller Jr (20). After several revisions, the questionnaire includes the following domains: pain, appearance, activity, recreation, swallowing, chewing, speech and shoulder function; the patient selects the best alternative related to what he felt in the last week before the interview. The current version (version 4), developed in 2001 (20) and used in this work, includes 12 questions related to specific functions of the head and neck, in addition to themes related to mood and anxiety, with each question having 3 to 5 answer categories with scores ranging from 0 (worst) to 100 (best). It also presents an open-ended question at the end of the questionnaire, asking the patient to describe problems that may not have been mentioned in the questions. Vartanian et al. (21), of the Department of Head and Neck Surgery and Otorhinolaryngology of Hospital do Câncer A. C. Camargo, validated the Portuguese version adapted to the national culture. The results of the survey were analyzed qualitatively and quantitatively. Quantitative analysis was carried out individually for each domain through a score, whose value ranges from 0 (worst QoL) to 100 (best QoL) and through the global average of these domains (sum of scores divided by 12), with the same numeric variation. The qualitative assessment was carried out by analyzing the open question, assessed individually. This questionnaire was used for its simplicity, being accessible to the patient (22). The questionnaires were completed by the patients themselves. When the patient found it difficult to fill the questionnaire out, he/she was assisted by a single interviewer. The two groups of patients, rehabilitated (G1) and non-rehabilitated (G2), were statistically analyzed in relation to QoL, as well as gender, age, medical history, cancer stage, time of cancer treatment and rehabilitation.
3.1 Statistical analysis
Exploratory data analysis was performed by calculating summary measures (mean, standard deviation, median, minimum, maximum, frequency and percentage). Comparison between groups was performed using the Mann-Whitney or Fisher's exact test. The level and significance adopted was 5%. The computer program used was the version 4.2.0. 2022 (©) of the R Foundation for Statistical Computing.
13 patients whose medical records had been evaluated were interviewed; they included 10 men and 3 women, with a mean age of 66.07 years, the youngest being 57 years old and the oldest 77 years old. All patients had a history of smoking and alcohol consumption, with smoking cessation in 100% of patients and alcohol use cessation in 84.6%. Regarding the total laryngectomy postoperative period, one patient had undergone the surgery less than three years before, four patients had undergone surgery 3-10 years before, five patients 10-15 years, one patient 15-20 years and two patients had undergone surgery more than 20 years before the survey. Regarding the time of VP use, one patient had less than three years of use, five patients had 3-10 years of use, four patients had 10-15 years, two patients had 15-20 years and one patient had more than 20 years of VP use.
4.1 Voice Quality Questionnaire
According to Table 1,
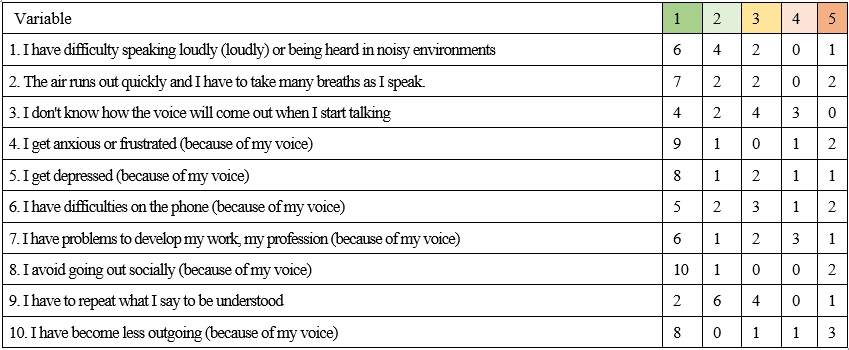
Table 1: Results of the Voice Quality of Life protocol.
Note: 1) It never happens and it's not a problem; 2) It happens infrequently and it is rarely a problem; 3) It happens sometimes and it is a moderate problem; 4) It happens a lot and it is almost always a problem; 5) It happens all the time and it really is a serious problem.
Source: Prepared by the authors (2023).
an average score of 71.54 was obtained, ranging from 20 to 100, median 85. The standard deviation was 26.47, with a coefficient of variation 37. According to the criteria defined in this study, ten patients were considered rehabilitated (G1) and three patients were considered not rehabilitated (G2).
4.2 University of Washington Quality of Life Questionnaire (19)
A mean total score of 79.78 was obtained, ranging from 55.5 to 94.5, median 80.5. The standard deviation was 11.68, and the coefficient of variation was 14.6, and p = 0.128; the comparison between G1 and G2 was not significant.
In the Pain domain (UW-QOL1), 84.6% of the patients answered that they had no pain; 7.7% answered that they had mild pain not requiring medication and 7.7% answered that they suffered severe pain, not controlled by medication.
In the Appearance domain (UW-QOL2), 69.2% answered that the change was minimal and 15.4% answered that appearance bothered them, but that they remained active. Regarding Activity (UW-QOL3), 76.9% of patients responded that they were as active as they had always been and 7.7% answered that they didn't leave the house because they did not have the strength.
Regarding Recreation (UW-QOL4), 30.7% of patients answered that they had no limitations for recreation at home or outside the home; 46.1% answered that there are few things that they cannot do, but that they still leave the house to have fun. In the Swallowing domain (UW-QOL5), 61.5% of patients answered that they could swallow normally; 38.5% answered that they could not swallow some solid foods. In the Chewing domain (UW-QOL6), 69.2% of patients answered that they could chew normally; 30.8% answered that they could eat light solid foods, but could not chew some foods. About Speech (UW-QOL7), 92.3% of patients answered that they had difficulty uttering some words, but that they could be understood even on the phone; and 7.7% answered that only their family and friends could understand them. Regarding the Shoulder function (UW-QOL8), 61.5% responded that their shoulder was stiff, but this did not affect their activity or strength and 15.5% responded that pain and weakness in their shoulder made them change jobs.
In the Taste domain (UW-QOL9), 76.9% of patients responded that they tasted food normally. In the Saliva domain (UW-QOL10), 84.6% of patients answered that their saliva had a normal consistency and 15.4% answered that they produced very little saliva. As to Mood (UW-QOL11), 46.1% of patients responded that their mood was excellent and was not affected by the cancer and 46.1% responded that their mood was generally good and was only occasionally affected by the cancer. Regarding Anxiety (UW-QOL12), 30.7% of patients answered that they were not anxious because of the cancer and 46.1% answered that they were a little anxious because of the cancer. Considering the domains, the patients scored those most important (UW-QOL13) as shown in Table 2.
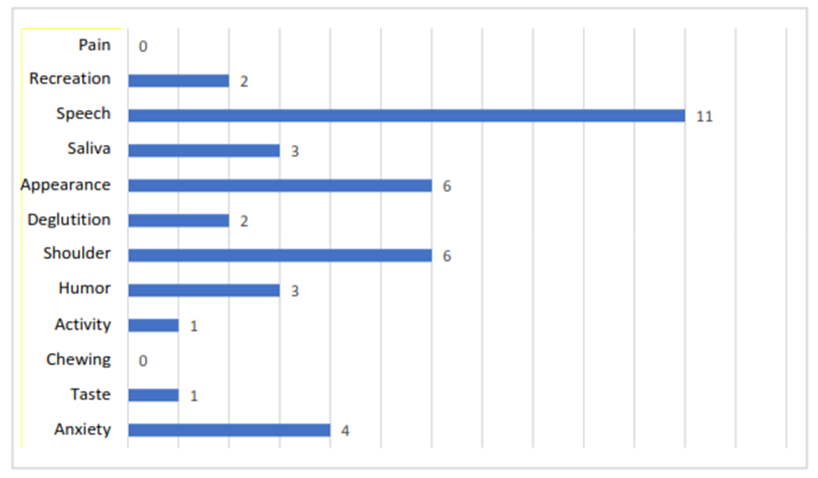
Source: Prepared by the authors (2023).
Table 2: UW-QOL13 - What issues have affected you most, during the past seven days? Mark (X) up to three alternatives.
Comparing with the month before the patient developed cancer, three patients rated their health-related QoL as much better, three rated it slightly better, six rated it more or less the same, and one rated it slightly worse (UW-QOL14). Overall, five patients said their health-related QoL over the last 7 days had been excellent, five said it had been good, two said it had been average, and one said it had been poor (UW-QOL15). Considering everything in life that contributes to personal well-being, two patients rated their overall QOL over the past seven days as excellent, eight rated it as good, two rated it average, and one rated it poor (UW-QOL16). In the open-ended question, six patients indicated loss of smell, one patient indicated increased salivation and six patients chose not to answer the question. The patients interviewed did not complain about the number of questions asked in the questionnaires.
4.3 Statistical analysis results
Data from 13 patients were reviewed; 10 of them (77%) were considered rehabilitated, according to the V-RQOL (score greater than 50).
Table 3 presents the quantitative analysis and descriptive measures of age, postoperative time, time of VP use, in addition to QoL questions, not showing significance in all variables by Mann-Whitney test
| Variable | Total (N=13) | Not Rehabilitated (N=3) | Rehabilitated (N=10) | p-value | |||
| Mean (SD) | Mean [Min;Max] | Mean (SD) | Mean [Min;Max] | Mean (SD) | Mean [Min;Max] | ||
| Age | 65.6 (5.49) | 66.0 [56.0;77.0] | 62.7 (4.62) | 60.0 [60.0;68.0] | 66.5 (5.62) | 66.0 [56.0;77.0] | 0.307 |
| Postoperative time | 12.2 (6.53) | 11.0 [3.0;24.0] | 13.0 (6.0) | 13.0 [7.0;19.0] | 12.0 (6.98) | 11.0 [3.00;24.0] | 0.670 |
| Time of prosthesis use | 9.88 (5.70) | 10.0 [0.50;21.0] | 12.0 (5.57) | 13.0 [6.00;17.0] | 9.25 (5.87) | 9.50 [0.50;21.0] | 0.351 |
| UW-QOL1 | 90.4 (28.0) | 100 [0.0;100] | 66.7 (57.7) | 100 [0.0;100] | 97.5 (7.91) | 100 [75.0;100] | 0.282 |
| UW-QOL2 | 75.0 (14.4) | 75.0 [50.0;100] | 66.7 (14.4) | 75.0 [50.0;75.0] | 77.5 (14.2) | 75.0 [50.0;100] | 0.254 |
| UW-QOL3 | 88.5 (24.2) | 100.0 [25.0;100] | 83.3 (28.9) | 100.0 [50.0;100] | 90.0 (24.2) | 100.0[25.0;100] | 0.648 |
| UW-QOL4 | 76.9 (19.0) | 75.0 [50.0;100] | 75.0 (25.0) | 75.0 [50.0;100] | 77.5 (18.4) | 75.0 [50.0;100] | 0.856 |
| UW-QOL5 | 87.3 (16.7) | 100.0 [67.0;100] | 78.0 (19.1) | 67.0 [67.0;100] | 90.1 (15.9) | 100.0 [67.0;100] | 0.271 |
| UW-QOL6 | 84.6 (24.0) | 100.0 [50.0;100] | 83.3 (28.9) | 100.0 [50.0;100] | 85.0 (24.2) | 100.0 [50.0;100] | 0.916 |
| UW-QOL7 | 64.4 (9.43) | 67.0 [33.0;67.0] | 55.7 (19.6) | 67.0 [33.0;67.0] | 67.0 (0.00) | 67.0 [67.0;67.0] | NC |
| UW-QOL8 | 69.4 (21.4) | 67.0 [33.0;100] | 78.0 (19.1) | 67.0 [67.0;100] | 66.8 (22.3) | 67.0 [33.0;100] | 0.437 |
| UW-QOL9 | 84.6 (32.3) | 100 [0.0;100] | 77.7 (38.7) | 100 [33.0;100] | 86.7 (32.2) | 100.0 [0.0;100] | 0.648 |
| UW-QOL10 | 89.7 (25.2) | 100.0 [33.0;100] | 100.0 (0.0) | 100.0 [100;100] | 86.6 (28.2) | 100.0 [33.0;100] | NC |
| UW-QOL11 | 82.7 (21.4) | 75.0 [25.0;100] | 75.0 (0.0) | 75.0 [75.0;75.0] | 85.0 (24.2) | 100.0 [25.0;100] | NC |
| UW-QOL12 | 64.2 (34.6) | 67.0 [0.0;100] | 33.3 (33.5) | 33.0 [0.00;67.0] | 73.5 (30.6) | 67.0 [0.00;100] | 0.071 |
| UW-QOL Total | 79.8 (11.7) | 80.5 [55.5;94.5] | 72.7 (7.76) | 75.8 [63.9;78.5] | 81.9 (12.1) | 85.5 [55.5;94.5] | 0.128 |
Note: SD: Standard Deviation; Min: Minimum; Max: Maximum; UW-QOL: University of Washington QoL Questionnaire. NC: not calculated, because there was no variation in one of the groups.
Source: Prepared by the authors (2023).
Table 3: Quantitative analysis and descriptive measures by group; p-value of comparison between groups.
Table 4 shows the qualitative analysis and comparison between groups in relation to the categorical variables. For this table, it was not possible to perform a statistical test, as there is at least one category with a low frequency of observations; therefore, in this case, data must be interpreted descriptively.
| Variable | Total (N=13) | Not Rehabilitated (N=3) | Rehabilitated (N=10) |
| Gender | |||
| Female | 3 (23.1%) | 2 (66.7%) | 1 (10.0%) |
| Male | 10 (76.9%) | 1 (33.3%) | 9 (90.0%) |
| T staging | |||
| T2 | 1 (7.69%) | 0 (0.0%) | 1 (10.0%) |
| T3 | 7 (53.8%) | 3 (100.0%) | 4 (40.0%) |
| T4a | 5 (38.5%) | 0 (0.0%) | 5 (50.0%) |
| N staging | |||
| N0 | 5 (38.5%) | 1 (33.3%) | 4 (40.0%) |
| N1 | 2 (15.4%) | 2 (66.7%) | 0 (0.0%) |
| N2b | 1 (7.69%) | 0 (0.0%) | 1 (10.0%) |
| N2c | 3 (23.1%) | 0 (0.0%) | 3 (30.0%) |
| N3b | 2 (15.4%) | 0 (0.0%) | 2 (20.0%) |
| Cancer staging | |||
| II | 1 (7.69%) | 0 (0.0%) | 1 (10.0%) |
| III | 6 (46.2%) | 3 (100.0%) | 3 (30.0%) |
| IV a | 4 (30.8%) | 0 (0.0%) | 4 (40.0%) |
| IV b | 2 (15.4%) | 0 (0.0%) | 2 (20.0%) |
| UW-QOL14 | |||
| Much better | 3 (23.1%) | 1 (33.3%) | 2 (20.0%) |
| A little better | 3 (23.1%) | 1 (33.3%) | 2 (20.0%) |
| More or less the same | 6 (46.2%) | 1 (33.3%) | 5 (50.0%) |
| A little worse | 1 (7.69%) | 0 (0.0%) | 1 (10.0%) |
| UW-QOL15 | |||
| Excellent | 5 (38.5%) | 0 (0.0%) | 5 (50.0%) |
| Good | 5 (38.5%) | 1 (33.3%) | 4 (40.0%) |
| Average | 2 (15.4%) | 1 (33.3%) | 1 (10.0%) |
| Bad | 1 (7.69%) | 1 (33.3%) | 0 (0.0%) |
| UW-QOL16 | |||
| Excellent | 2 (15.4%) | 0 (0.0%) | 2 (20.0%) |
| Good | 8 (61.5%) | 2 (66.7%) | 6 (60.0%) |
| Average | 2 (15.4%) | 0 (0.0%) | 2 (20.0%) |
| Bad | 1 (7.69%) | 1 (33.3%) | 0 (0.0%) |
| Open UW-QOL | |||
| Increased saliva | 1 (14.3%) | 0 (0.0%) | 1 (20.0%) |
| Loss of smell | 6 (85.7%) | 2 (100.0%) | 4 (80.0%) |
Note: Data presented in frequency (percentage); UW-QOL: University of Washington QoL Questionnaire. Source: Prepared by the authors (2023).
Table 4: Qualitative analysis and frequency and percentage distribution of categorical variables analyzed in the study.
Cancer patients have to make difficult decisions regarding treatment, with the possibility of exchanging their QoL for life span. Several factors are involved in patients' decision regarding cancer treatment, and the personal costs they are willing to pay to prolong their life. [23]. Patients with better health generally value life time, and conversely, those with worse physical status prefer QoL [24]. In laryngeal cancer, the main impact after total laryngectomy is the loss of voice, and vocal rehabilitation is essential for QoL recovery. Since the introduction of VP by Singer and Blom in 1980, there has been a significant improvement in the success of restoring vocal
communication after total laryngectomy (25). The sample evaluated in this study was mostly composed of patients who had been in the postoperative period of total laryngectomy for more than ten years (61%) and in use of VP also for more than ten years (53%). For this study, the V-RQOL and UW-QOL questionnaires were chosen, as they proved to be more specific considering the sequelae inherent to total laryngectomy and its injuries, as described in the literature [26]. The two questionnaires include a total of 22 questions, and their association helps obtaining important information about the impact of the disease and treatments on the life of individuals, and may constitute auxiliary tools for the planning and for the most appropriate conduct for each case [27]. The patients interviewed did not complain about the number of questions in the questionnaires applied. This made the association of the two questionnaires on QoL an executable tool in this study. The first questionnaire applied was the V-RQOL, which analyses the QoL of total laryngectomized patients related to voice, which specifically points out how much the difficulty in using the voice is a problem in the patient's daily life [28].
The RQOL indicated a good voice quality, with an average score of 71.54, demonstrating that the VP has good adaptability and promotes satisfactory vocal rehabilitation. Out of the sample assessed, ten patients (76.9%) were considered rehabilitated (G1) and three patients (23.1%) were considered not rehabilitated (G2). Almeida [29] also applied the QVV in 20 total laryngectomized patients using VP and with a postoperative period of 2 to 11 years; they found a mean score of 83 which is higher than the mean score found in this study.
Daily VP hygiene is required with the use of a cleaning brush and topical nystatin to prevent fungal colonization and VP leakage. VP lifetime is also significantly associated with gastroesophageal reflux [30]. In this study, all patients received guidance on VP hygiene during their routine appointments.
One of the causes of vocal rehabilitation failure in patients with VP is spasm of the pharyngoesophageal segment. It is triggered by the entry of air into the esophagus, which prevents the progression of airflow to the pharynx, preventing vibration of the pharyngeal mucosa and phonation, thus being an obstacle to vocal rehabilitation in patients using VP [31]. This spasm can be treated through dilation of the pharyngoesophageal segment, with myotomy of the middle and inferior pharyngeal constrictors, or by neurectomy of the pharyngeal plexus, or by chemical denervation of the pharyngoesophageal segment with botulinum toxin [31]. No patient in this study underwent myotomy, neurectomy or chemical denervation of the pharyngoesophageal segment. It is also necessary to consider that not all laryngectomy patients using VP benefit from the same level of rehabilitation. Problems with the VP, such as reduced lifespan due to biofilm growth, periprosthetic leaks, swallowing or bronchoaspiration of the VP, in addition to problems associated with the fistula, such as tracheoesophageal granulomas, infections, stenosis and even clogging of the tracheoesophageal fistula, may result in poor voice performance and force the patient to undergo a greater number of medical-surgical procedures, many times aggressive, with potential secondary discomfort [32]. All of the patients in this study have experienced the growth of biofilm on the VP and periprosthetic leaks as the VP approaches its routine replacement date, but none of the patients had experienced complications with the fistula at the time of the interview.
The second questionnaire applied to analyze the QoL of head and neck cancer patients treated with total laryngectomy was the UW-QOL. This questionnaire shows how much the sequelae of cancer treatment in the head and neck region specifically affect the QoL of patients [27]. The UW-QOL questionnaire showed an average score of 79.78, with the following domains yielding the highest scores: pain, activity, taste and saliva. The domains with the lowest scores were: speech, anxiety and appearance. The longer the postoperative period, the higher the QoL. According to the literature, patients operated more than two years before the date of the interview achieved better QoL scores, with statistical significance for the speech domain, with p=0.006 [33]. This is in line with our study, since 12 patients were more than two years postoperative. The better perception of QoL detected after long-term laryngectomy may indicate that patients have adapted to their new condition over time, modifying their habits, social and family relationships. It may also be related to the possibility of better speech rehabilitation methods and postoperative adaptability [34].
Out of the sample assessed 76.9% of patients reported being as active after the surgery as they had always been, demonstrating that this domain had no impact on their QoL. Work is an important issue in the postoperative period of total laryngectomy. Work makes people build social bonds and their identity, and after total laryngectomy with consequent loss of voice, patients tend to retire early [35]. The lack of work generates different feelings for the individual, such as the feeling of worthlessness, sadness, devaluation and low self-esteem. These feelings may be accompanied by the loss of references and social contacts and purchasing power, and reinserting these individuals into the job market is a major factor in improving the QoL of the vocal rehabilitated individuals [36]. Out of the patients interviewed, 92.3% complained having difficulty uttering a few words, but that they could be understood even on the phone, demonstrating the great positive impact of communication on the QoL of total laryngectomy patients and its influence on their social life. It was found that the interviewees' taste was not impaired in 76.9% of the cases, demonstrating that this factor contributed positively to the patients’ QoL. Taste alteration in 23.1% of patients may be related to postoperative radiotherapy, as well as loss of smell, which acts in a complementary way to the taste in food [37]. Total laryngectomized patients, due to the fact that breathing occurs through the terminal tracheostomy, end up not pushing air into the nasal cavity, which impairs the sense of smell [38].
Out of the sample assessed, 53.9% of patients experienced some type of change in mood due to cancer, demonstrating that this factor harmed their QoL, and 69.3% considered anxiety a factor that was harmful to their QoL. Female participants had lower scores in the mood and anxiety domains, with a greater chance of developing depression after treatment. These data are confirmed in the literature, indicating that women suffer greater negative impacts on their QoL than men [33].
Early identification of depression, worries and anxiety in patients with head and neck cancer is of great importance, particularly because depression is underdiagnosed in cancer patients (39). We should emphasize the importance of incorporating QoL assessment into the daily practice and the approach of a multidisciplinary team that takes into account each patient’s personality, personal needs and relational conditions, in order to determine and apply the appropriate speech rehabilitation method to achieve a better QoL [40].
In the open-ended question, 6 patients indicated the loss of smell. One hypothesis of olfactory impairment after total laryngectomy is the interruption of normal nasopulmonary airflow due to a permanent disconnection between the upper and lower airways, with the terminal tracheostomy. The alteration in the air flow reduces the stimuli in the olfactory bulb, causing apoptosis and atrophy [41].
This study demonstrated that the UW-QOL questionnaire is an important assessment tool and its incorporation into clinical practice is of great relevance, as it can help improve and measure the effectiveness of treatments and their sequelae [33].
The need to develop public policies was also noted, both for the prevention of laryngeal cancer, and for helping patients who have already undergone total laryngectomy to restore their voices and be reintegrated into the social environment [27].
The main limitation of this study is the small number of patients assessed, which may have resulted in the lack of sample power. However, we ought to consider that, after applying our strict inclusion and exclusion criteria, such as extended follow-up, the total number of the sample’s selected patients was drastically reduced.
Another limitation due to the cross-sectional design used in our investigation is that the patients included in the study may not be representative of the total population of patients who underwent treatment in this service, but only of those who survived, taking into account the morbidity and mortality of the cancer disease, since total laryngectomy is a surgery indicated for patients with advanced neoplasia who can undergo resection.
To minimize information and selection biases, the data collection procedure was aided by a single investigator. A limitation of this study may be related to the recall bias, since the patients included were submitted to the surgical procedure at different times before the start of the study. Another limitation could be related to cognitive bias, as most patients were over 65 years of age.
Despite the methodological limitations inherent to the design of this study, the results can be used in the planning and evaluation of future actions geared to patients undergoing treatment for head and neck cancer.
It can be critically considered that the vocal prosthesis presents good results in the vocal rehabilitation of patients, which in clinical practice in this country can be well indicated for patients who were unable to achieve rehabilitation with esophageal voice, since the phonatory prosthesis, despite periodic changes, still presents a lower cost and good adaptability when compared to the electronic larynx.
The rehabilitation of total laryngectomized patients with tracheoesophageal VP proved to be a reproducible method with few complications for the patient. There was a significant improvement in QoL after treatment, with most patients considering their QoL good to excellent at the time of the interview.
Appendix 1 − Voice-related Quality of Life. (V-RQOL) protocol
We are trying to learn more about how a voice problem can interfere with your daily activities. Please answer all questions based upon what your voice has been like over the past 2 weeks. There are no “right” or “wrong” answers. Considering both how severe the problem is when you get it, and how frequently it happens, please rate each item below on how “bad” it is (that is, the amount of each problem you have).
Rating Scale: [-----1-----2-----3-----4-----5-----]
1= None, not a problem
2= A small amount
3= A moderate (medium) problem
4= A lot
5= Problem is “as bad as it can be”
How much of a problem is this because of my voice?
1. I have trouble speaking loudly or being heard in noisy situations
[-----1-----2-----3-----4-----5-----]
2. I run out of air and need to take frequent breaths when talking
[-----1-----2-----3-----4-----5-----]
3. I sometimes do not know what will come out when I begin speaking
[-----1-----2-----3-----4-----5-----]
4. I am sometime anxious or frustrated (because of my voice)
[-----1-----2-----3-----4-----5-----]
5. I sometimes get depressed (because of my voice)
[-----1-----2-----3-----4-----5-----]
6. I have trouble using the telephone (because of my voice)
[-----1-----2-----3-----4-----5-----]
7. I have trouble doing my job or practicing my profession (because of my voice)
[-----1-----2-----3-----4-----5-----]
8. I avoid going out socially (because of my voice)
[-----1-----2-----3-----4-----5-----]
9. I have to repeat myself to be understood
[-----1-----2-----3-----4-----5-----]
10. I have become less outgoing (because of my voice)
[-----1-----2-----3-----4-----5-----]
Appendix 2 − University of Washington in Seattle Questionnaire (UW- QOL)
This questionnaire asks about your health and quality of life over the past seven days. Please answer all of the questions by checking one box for each question.
1. PAIN. (Tick one box: þ )
(100) I have no pain.
(75) There is mild pain not needing medication.
(50) I have moderate pain - requires regular medication (e.g. paracetamol).
(25) I have severe pain controlled only by prescription medicine (e.g. morphine).
(0) I have severe pain, not controlled by medication.
2. APPEARANCE. (Tick one box: þ )
(100) There is no change in my appearance.
(75) The change in my appearance is minor.
(50) My appearance bothers me but I remain active.
(25) I feel significantly disfigured and limit my activities due to my appearance.
(0) I cannot be with people due to my appearance.
3. ACTIVITY. (Tick one box: þ )
(100) I am as active as I have ever been.
(75) There are times when I can't keep up my old pace, but not often.
(50) I am often tired and have slowed down my activities although I still get out.
(25) I don't go out because I don't have the strength.
(0) I am usually in bed or chair and don't leave home.
4. RECREATION. (Tick one box: þ )
(100) There are no limitations to recreation at home or away from home.
(75) There are a few things I can't do but I still get out and enjoy life.
(50) There are many times when I wish I could get out more, but I'm not up to it.
(25) There are severe limitations to what I can do, mostly I stay at home and
watch TV
(0) I can't do anything enjoyable.
5. SWALLOWING. (Tick one box: þ )
(100) I can swallow as well as ever.
(70) I cannot swallow certain solid foods.
(30) I can only swallow liquid food.
(0) I cannot swallow because it "goes down the wrong way" and chokes me.
6. CHEWING. (Tick one box: þ )
(100) I can chew as well as ever.
(50) I can eat soft solids but cannot chew some foods.
(0) I cannot even chew soft solids.
7. SPEECH. (Tick one box: þ )
(100) My speech is the same as always.
(70) I have difficulty saying some words but I can be understood over the phone.
(30) Only my family and friends can understand me.
(0) I cannot be understood.
8. SHOULDER. (Tick one box: þ )
(100) I have no problem with my shoulder.
(70) My shoulder is stiff but it has not affected my activity or strength.
(30) Pain or weakness in my shoulder has caused me to change my
work / hobbies.
(0) I cannot work or do my hobbies due to problems with my shoulder.
9. TASTE. (Tick one box: þ )
(100)I can taste food normally.
(70) I can taste most foods normally.
(30) I can taste some foods.
(0) I cannot taste any foods.
10. SALIVA. (Tick one box: þ )
(100) My saliva is of normal consistency.
(70) I have less saliva than normal, but it is enough.
(30) I have too little saliva.
(0) I have no saliva.
11. MOOD. (Tick one box: þ )
(100) My mood is excellent and unaffected by my cancer.
(75) My mood is generally good and only occasionally affected by my cancer.
(50) I am neither in a good mood nor depressed about my cancer.
(25) I am somewhat depressed about my cancer.
(0)I am extremely depressed about my cancer.
12. ANXIETY. (Tick one box: þ )
(100) I am not anxious about my cancer.
(70) I am a little anxious about my cancer.
(30) I am anxious about my cancer.
(0) I am very anxious about my cancer.
Which issues have been the most important to you during the past 7 days?
Tick þ up to 3 boxes.
Pain Swallowing Taste
Appearance Chewing Saliva
Activity Speech Mood
Recreation Shoulder Anxiety
GENERAL QUESTIONS
Compared to the month before you developed cancer, how would you rate your health-related quality of life? (Tick one box: þ )
(100) Much better
(75) Somewhat better
(50) About the same
(25) Somewhat worse
(0) Much worse
In general, would you say your health-related quality of life during the past 7 days has been: (Tick one box: þ )
(100) Outstanding
(80) Very good
(60) Good
(40) Fair
(20) Poor
(0) Very poor
Overall quality of life includes not only physical and mental health, but also many other factors, such as family, friends, spirituality, or personal leisure activities that are important to your enjoyment of life. Considering everything in your life that contributes to your personal well-being, rate your overall quality of life during the past 7 days. (Tick one box: þ )
(100) Outstanding
(80) Very good
(60) Good
(40)Fair
(20) Poor
(0) Very poor
Please describe any other issues (medical or nonmedical) that are important to your quality of life and have not been adequately addressed by our questions (you may attach additional sheets if needed).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
