
Case Report | DOI: https://doi.org/10.31579/2693-4787/027
*Corresponding Author: Lena Marinova, Complex Oncology Center; Department of Radiotherapy -Ruse, Bulgaria.
Citation: L Marinova, B Yordanova, N Evgeniev. (2021). Uterine carcinosarcoma аfter prolonged antiestrogenic therapy - pathohistological characteristics, immunohistichemical analysis, prognosis and complex treatment. Clinical Oncology Research and Reports. 2(2) Doi: 10.31579/2693-4787/027
Copyright: © 2021 Lena Marinova. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium provided the original author and source are credited.
Received: 11 August 2021 | Accepted: 23 August 2021 | Published: 02 September 2021
Keywords: uterine carcinosarcoma; pathohistological analysis; immunohistochemical analysis; surgery; simultaneous chemo-radiotherapy; complex treatment
Uterine carcinosarcoma (UCS) is a rare aggressive neoplasm.We present a clinical case with UCS, developed during along-term five years adjuvant tamoxifen treatment and ovarian suppression with LHRH agonist on the occasion of invasive ductal breast carcinoma. Crucial for obtaining diagnosis of this rare aggressive neoplasm is the strict pathohistological and immunohistochemical analysis, carried out by an experienced pathologist. Every patient with a history of breast carcinoma is a subject for periodic monitoring. Genital bleeding is required to perform a separated endometrial abrasion with a precise histological study. For UCS / III C2 FIGO stage without distant metastases is necessary to conduct a maximal surgical tumor reduction, involving ever total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic and para-aortic lymphadenectomy, peritoneal cytology, and omentectomy, followed by a combined simultaneous chemo-radiotherapy of tumor bed and pelvic lymph nodes, definitive radiotherapy of para-aortical lymph nodes, as well as adjuvant chemotherapy.
Malignant uterine neoplasms containing both carcinomatous and sarcomatous elements are designated in the World Health Organisation (WHO) classification of uterine neoplasms as carcinosarcomas [1]. Uterine carcinosarcomas (UCS) are characterized with a rare occurrence, accounting for only 2–5% of all uterine malignancies [2-5]. They are aggressive undifferentiated carcinomas which include both carcinomatous and sarcomatous elements, arising from a single malignant epithelial clone [6-9]. Carcinosarcomas are classified into two histological subtypes based on their sarcomatous component, namely homologous or heterologous [10,11]. Extremely important for the diagnostics of this rare aggressive neoplasm is the strict pathohistological and immunohistochemical analysis, carried out by an experienced pathologist. Due to rare diagnosis, there are no established standards for complex oncology treatment. We will present a rare UCS, developed on the basis of long-term antiestrogenic hormone treatment for invasive ductal breast carcinoma.
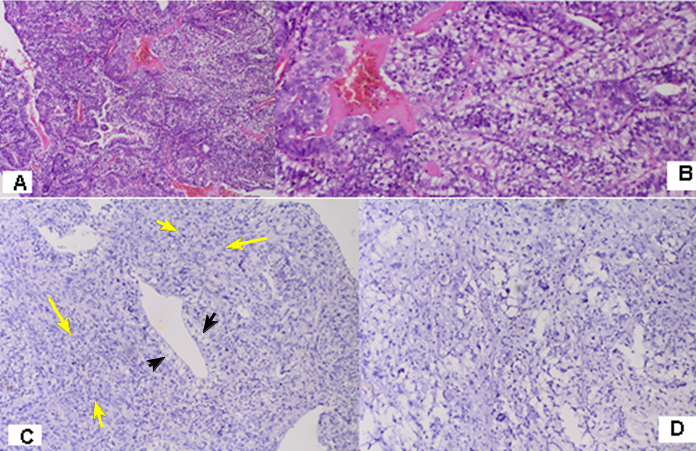
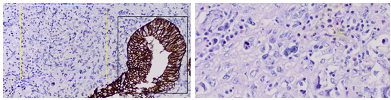
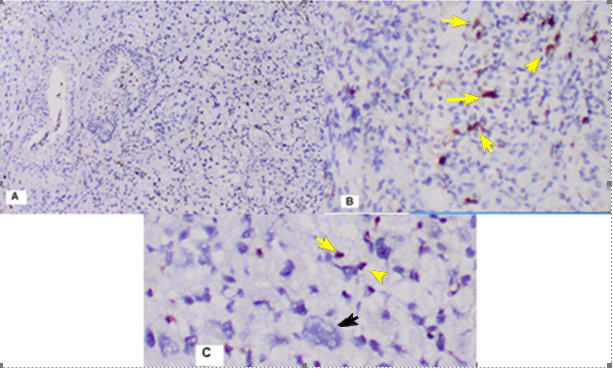
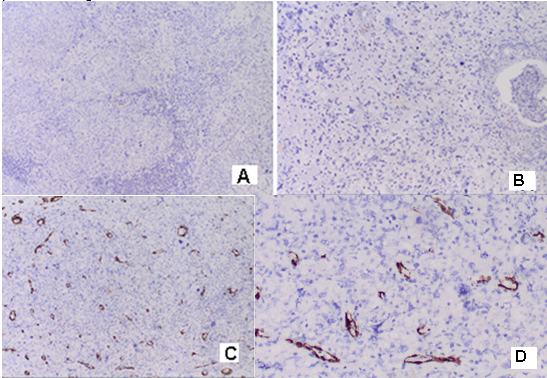
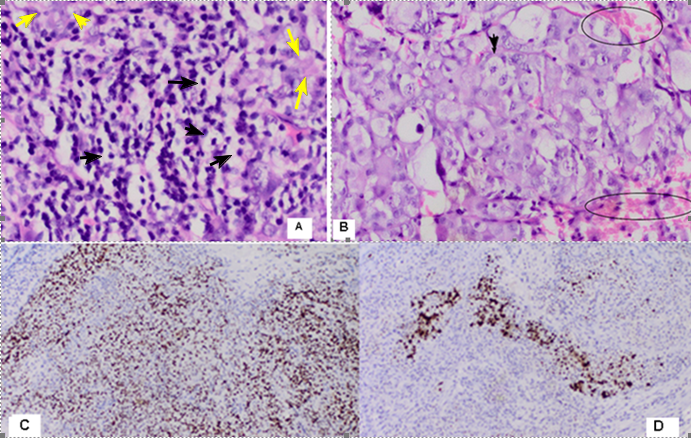
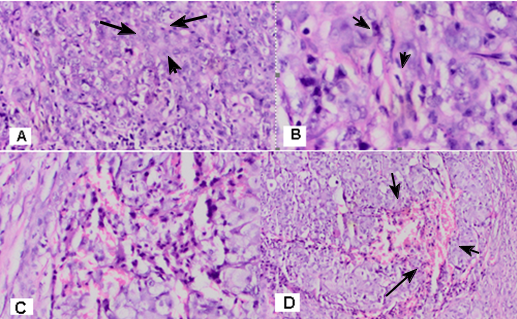
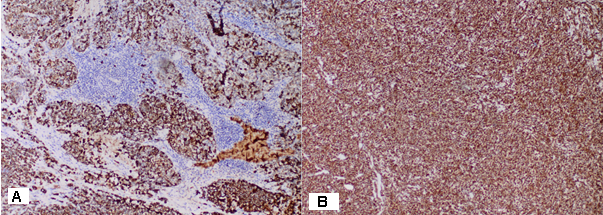
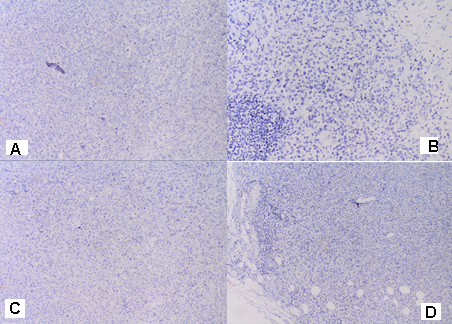
Clinical case - A 50-year-old woman diagnosed with breast cancer invasive ductal carcinoma of the right breast / pT2 N1 M0; G2; ER and PR-positive; HER2 –negative) seven years ago. A quadrectomy with axillary dissection has been performed in 2013 and followed with 6 courses adjuvant chemotherapy (Ch) with docetaxel and postoperative radiotherapy (RT) of the right breast and the regional lymph nodes up to total dose (TD) 50 Gy, an ovarian suppression with LHRH agonist and anti-estrogenic hormone therapy with tamoxifen have been added. Separated endometrial abrasion have been performed in July 2020 for genital bleeding. From pathohistological and immunohistochemical analysis an uterine carcinosarcoma (UCS) with cervical tumor infiltration was confirmed. Patohistological morphology and immunohistichemical analysis of the material from separated endometrial abrasion - Histological examination revealed classical malignant biphasic growth pattern with undifferentiated epithelial component, composed of clear cells with light, relatively wide cytoplasm and small- round nuclei, atypical cells with hyperchromatic nuclei. Cells form wide fields and adenoid structures. Tumor infiltration in smooth muscle and subepitelial endocervical area is reported. The epithelial component is surrounded by undifferentiated mesenchymal tissue, consisting of pleomorphic and bizarre tumor cells visualized variable cellularity with varied size, as well as giant cells usually bizarre with multilobulated nuclei, irregular mitosis, histiocyte-like cells with vacuolated nuclei with abundant clear cytoplasm (mesenchymal component) (Fig.1,Fig.2B). In the carcinoma component, a positive IHC reaction to Cytokerin is reported and the sarcomoid component shows negative expression. And the two cellular components are positive to Vimentin. Focal positive IHC expression to S-100 protein in single tumor cells with with atypical cell mitosis. Negative IHC expression to Myogenin, Desmin and SMA in tumor cells, but positive expression in the smooth muscular walls of the blood vessels. (Fig.2A-Fig.5). Based on the morphological and immunohistochemical (IHC) study, a malignant mixed Mullerian tumor of the uterus was found. The carcinoma component consists of clear cell carcinoma with hight grade endometroid adenocarcinoma. The sarcomatoid cells consist undifferentiated sarcoma with scars of lipogenic phenotype in pathogenesis, given the focal immunohistochemical expression of S-100 protein in single tumor cells. In August 2020 has been carried out Robot-assisted total hysterectomy with two-sided adnexectomy without lymph nodes pelvic dissection. Pathohistological analysis reports endometrium with carcinosarcoma infiltration, meometrium with an invasion of up to 50% of the uterine wall with abundant lymphovascular invasion; uterine cervix and endocervix with tumor emboli and neoplastic invasion; Fallopian tubes and ovaries with tumor emboli and metastases. Immunohistochemical analysis reports positive expression of tumor cells to CKAE 1/3 and negative to GATA 3, Mammaglobin and GCDFP.
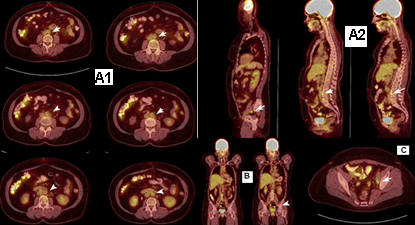
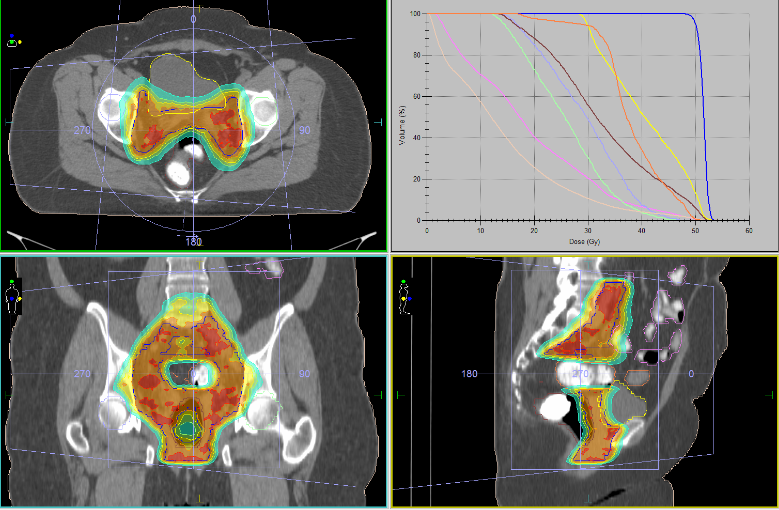
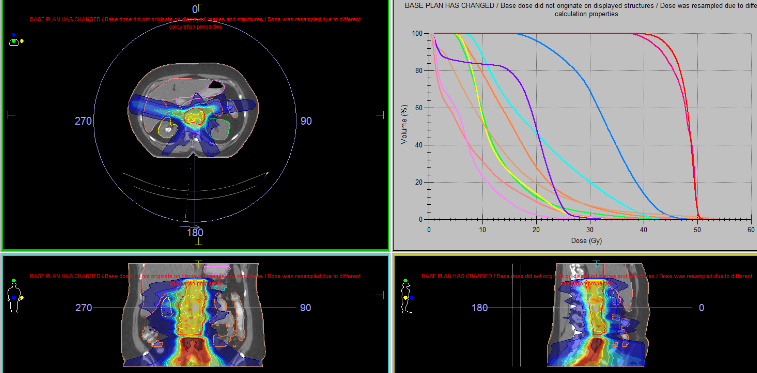
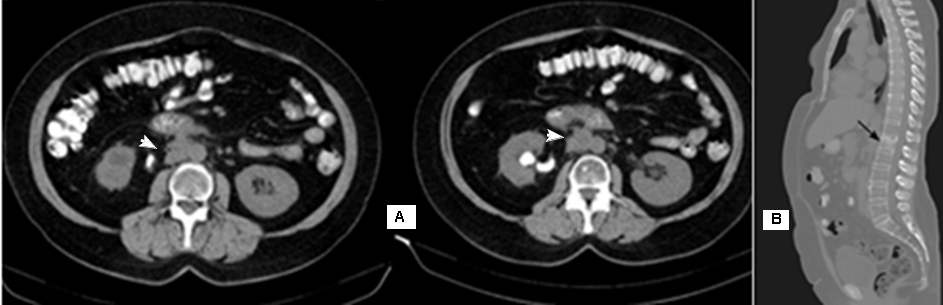
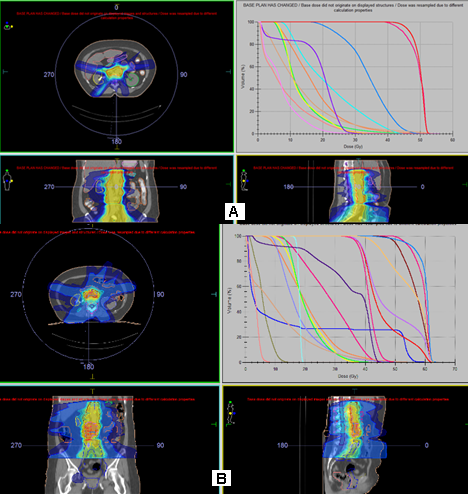
PET/CT have been performed 3 months after surgery in Oct 2020. Metabolically active pelvic and para-aortic lymph nodes at L2-L3 level, have been suspected for metastatic (Fig.6). Thus, it was confirmed locally advanced uterine carcinosarcoma (pT3bcN2M0), but postoperative pelvic and para-aortic lymph nodes dissection was not carried out. After surgery, the patient conducted combined with Ch (cisplatin) intensity modulated radiation therapy (IMRT) in the tumor bed and bilaterally pelvic lymph nodes up to total dose (TD) 50 Gy (Fig.7), followed by definitive RT of the para-aortic lymph nodes up to 52 Gy with daily dose (DD) 1.8 Gy ( Fig.8). Control CT and PET/CT from May 2021 reports disease progression with metabolic active bone marrow engagement zones in the vertebra C1 and L3, a pathological fracture of L1 and a metabolic active area on the right para-aortic lymph nodes at level L2-L3 (Fig.9). After a biopsy of a pathologically increased inguinal lymphatic node done on 10 Jun 2021, immunohistochemical analysis proved metastasis of uterine carcinosarcoma (Fig.10-Fig.14). Due to pain syndrome, we conducted palliative re-irradiation in the area of metastatic vertebrae and metastatic para-aortic lymph nodes at L2-L3 level in June 2021 (Fig.15)
In humans, UCSs are very aggressive tumors and comprise ~5% of uterine malignancies [12, 13]. Carcinosarcoma /malignant mixed Mullerian tumor (MMMT) of the endometrium accounts for only 1%−2% of all gynecological malignancies [14]. Carcinosarcomas are biphasic malignant tumors composed of 2 distinct neoplastic cell populations: epithelial (or carcinomatous) cells, and mesenchymal (or sarcomatous) cells [15].
The risk factors to develop the UCS include obesity, nulliparity, exogenous estrogen, tamoxifen, and exposure to pelvic radiation, while progestin-containing contraceptives are thought to have protective effects [7, 16]. We present a rare clinical case with UCS, developed on the basis of long-term antiestrogenic hormone treatment with tamoxifen and ovarian suppression with LHRH agonist on the occasion of invasive ductal breast carcinoma.
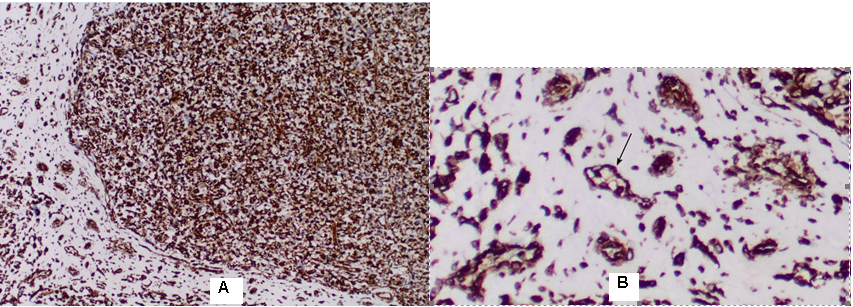
A neoplastic population may undergo mutations that lead to transformation from an epithelial to a mesenchymal phenotype (epithelial–mesenchymal transition) [12]. The tumor relapse can be explained by the mesenchymal transdifferentiated subpopulations of cancer cell nests that are induced by the fibroblastic stroma and are readily radio-resistant and chemo-resistant [17]. Epithelial to mesenchymal transition (EMT) is involved in tumor progression with metastatic expansion, and the generation of tumor cells with stem cell properties that play a major role in resistance to anticancer treatment [18-20]. EMT is a crucial step in metastasis that enables polarized immotile epithelial cells to gain fibroblast-like mesenchymal abilities such as enhanced motility [21]. In Fig. 3, we present the positive IHC expression in both cell populations carcinomatous and sarcomatous with infiltration in myometrium. Vimentin staining confirms mesenchymal origin of some tumors, but it is normally positivated in endometrial stromal cells, endometrial glandular structures and in lymphocytes, neutrophils, macrophages and platelets [22]. Normal proliferative-phase and secretory-phase endometrial stromal cells showed the following immunopositivity: vimentin 10 of 10, muscle-specific actin (MSA) 10 of 10, alpha-smooth muscle actin (alpha SMA) 10 of 10, desmin nine of 10, cytokeratin (AE1/AE3 and CAM 5.2) zero of 10, epithelial membrane antigen (EMA) zero of 10, and S-100 protein zero of 10 [23]. In recent years, Vimentin has been recognized as a marker for epithelial-mesenchymal transition [24].
MRI and fluorodeoxyglucose (FDG) PET-CT can help detect lymph node involvement prior to surgery [25]. In the presented clinical case, PET-CT is carried out after the operation without lymphatic dissection of pelvic lymph nodes. The imaging study shows a local advanced tumor with pelvic and paraaortic lymph nodes infiltration, which is typical of carcinosarcomas (Fig.6). Despite the combined chemo-radiotherapy of pelvic and paraaortic lymph nodes (Fig.7, Fig.8), a progression of UCS is detected with an inguinal lymph node and bone marrow desimination / distant metastasis M1 after six months (Fig.9). This progression of the disease impedes the re-irradiation of the metastatic lymph nodes and palliative exposure of metastatic vertebrae in strict observance of tolerant doses in neighboring critical organs / thin bowels, kidneys, spinal cord (Fig.15).
The overall prognosis of UCS is poor, even with the best of care, due to its aggressive behavior [7, 16]. It is likely that a sarcomatous component within an endometrial cancer is a histological marker of increased aggressiveness [26]. The risk of recurrence is higher with larger tumors, higher cancer stage at initial presentation, the existence of lymphovascular involvement, and deeper myometrial invasion [27]. UCS with the epithelial elements, high grade carcinoma and serous and clear cell components were associated with a higher frequency of metastases, deep myometrial invasion, lymphatic or vascular space invasion, and cervical involvement, all parameters indicative of an aggressive behaviour [11, 28]. In our clinical case, we take into account all the above-mentioned adverse prognostic factors as a mixed carcinoma cell component composed of clear cell carcinoma and high-grade endometrial carcinoma, advanced UCS (pT3bcN2M0), lymphovascular tumor invasion, pleorphic sarcomatous component with phenotype of lipublastoma and metastases in the paraaortic lymph nodes.All these factors show an extremely malignant tumor requiring aggressive complex treatment.
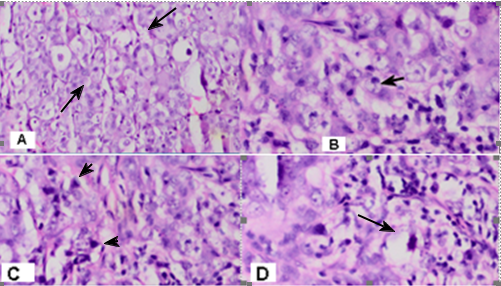
The basic definition of UCS is the following: 1/ Biphasic, malignant tumor with high grade epithelial and sarcomatous components.; 2/ Sarcomatous component is derived from the carcinomatous component as a result of metaplasia / transdifferentiation epithelial to mesenchymal transition [29]. Malignant mixed mesodermal tumors, also called carcinosarcomas, are diagnosed mainly in postmenopausal women and are composed of mixed malignant epithelial and mesenchymal components, usually high grade [30]. This proves that the basic meaning for diagnosis is a precise pathohistological feature of combination of the two tumor components-carcinoma, (more frequently high grade carcinoma- high grade endometrial adenocarcinoma, clear cell or serous carcinoma) and a homologous or heterologous sarcomatoid component (Fig.1,Fig.2A,Fig13). Histological examination in our clinical case revealed classical malignant biphasic growth pattern with carcinoma cells in glandular structures undifferentiated epithelial component, mixed by undifferentiated mesenchymal tissue (sarcomatoid component), consisting of monstruous and multinucleated tumor cells with hyperchromatic nuclei and scant cytoplasm, myxoid areas, tumor necrosis and haemorrhage with type of pleomorphic sarcoma (Fig.1, Fig.2B, Fig 10 A/B). Cells are visualized variable cellularity with varied size, as well as giant cells usually bizarre, irregular mitosis, histiocyte-like cells with vacuolated nuclei, atypical cells with hyperchromatic nuclei, irregular fascicles, cells with abundant clear cytoplasm, psammoma bodies and hyalinized stroma, associated with solid pattern (Fig.11, Fig.12). The carcinoma cells component consists of clear cell carcinoma with high grade endometrioid endometrial carcinoma. Endometrial clear cell carcinomas (CCC) constitute fewer than 5% of all carcinomas of the endometrium [31]. Cells have clear cytoplasm, hyalinized stroma associated with solid pattern, numerous grade 3 nuclei and thin fibrous septae [32].These pathologist characteristics are well visible in Fig.1B/C, Fig.2A. Solid architecture and polygonal cells with moderate to abundant clear or eosinophilic cytoplasm are characterized in clear cell carcinoma [33]. The definition of undifferentiated/unclassified sarcoma is pleomorphic sarcoma composed of fibroblasts, myofibroblasts and histiocyte-like cells [34]. In the presented clinical case, the sarcomatoid component is made up of рleomorphic and bizarre tumor cells with foamy cytoplasm and marked atypia, in background of collagenous and mixoid stroma, which is typical of the undifferentiated sarcoma cells (Fig.10 A/B, Fig.11, Fig.12). Fig.11 and Fig.12presents pronounced cellular polymorphism, lipoblasts and zones of hemorrhage.
Histopathology and immunohistochemistry revealed a mixed, anti-cytokeratin AE1/AE3-positive epithelial, and vimentin-positive mesenchymal neoplasm consistent with a homologous carcinosarcoma, also called malignant mixed Müllerian tumor, with areas of double-labeling [35]. Immunohistochemically, UCSs typically express epithelial (cytokeratins and epithelial membrane antigen) and stromal lineage markers (vimentin, CD10, CD34) in relation to their histologic appearances [36]. Areas of double-labeling with cytokeratins and vimentin, and immunohistochemical staining for p16, p53, and PAX8, may be helpful in establishing a diagnosis of UCS [37].For precision diagnosis of the carcinoma and sarcoma component, IHC is required. We received positive diffuse IHC reaction to Cytokeratin AE1/AE3 in the carcinoma component in which clear cell adenocarcinoma stands out and negative reaction to Cytokeratin AE1/AE3 in the sarcomatoid component, which is mixed by the adenocarcinoma cells component (Fig.2/A,Fig.13/A).Immunohistochemically clear cell carcinoma has negative expression to estrogen and progesterone receptors [31], we take into account a positive reaction to these receptors due to high-grade cells of endometroid endometrial carcinoma (Fig.10C/D). Undifferentiated/unclassified sarcoma is high grade sarcoma with no distinctive microscopic, immunohistochemical or molecular features fitting any specific line of differentiation [34, 38]. Large round, spindle or bizarre cells with marked nuclear anaplasia and large prominent nucleoli are Cytokeratin AE1/AE3 negative, which proves the presence of high-grade sarcoma cells (Fig.2A/B, Fig.13/A). In the heterologous subtype USC, the mesenchymal element includes foci of striated muscle, cartilage, bone (sometimes covered by plump osteoblasts), and/or adipose tissue (i.e., tissue types not normally present in the uterus). These foci also often display malignant features [39]. In the presented clinical case, the sarcomatoid component displays positive expression not only to Vimentin, but also focal expression to S-100 protein in single tumor cells, which shows lipoblastic sarcoma histogenesis (Fig.3A/B, Fig.4). The definition of pleomorphic liposarcoma is widespread high grade, pleomorphic tumor cells with some lipoblasts but no evidence of well differentiated liposarcoma. Pleomorphic lypoblastoma cells show positive expression to Vimentin and S-100 Protein [40], which is visible in Fig.3A/B and Fig.4. In the pleomorphic areas the expression of smooth muscle markers (desmin 10 of 28, muscle-specific actin 13 of 28, and α-smooth muscle actin 14 of 28) was significantly reduced [36]. In Figure 5, we report negative IHC expression to Myogenin and Desmin, as well as negative expression to SMA in tumor cells, but positive expression in the smooth muscular walls of the blood vessels.The liposarcom cells are negative to Desmine [41]. In the clinical case, due to a history of breast carcinoma 7 years ago, for differential diagnosis between lymph metastasis of uterine carcinosarcoma or breast carcinoma, we conducted immunohistichemic analysis with the specific breast carcinoma immune histochemical markers HER2, Mamaglobin and GCDFP (Fig.14 A/B,D). A negative expression is reported, indicating that it is a metastase of a uterine carcinosarcoma. A negative IHC reaction to Melan A excludes the diagnosis malignant melanoma (Fig.14 C).
Uterine carcinosarcomas should be regarded as metaplastic carcinomas and adjuvant treatment should probably be similar to that directed against aggressive high grade endometrial carcinomas, rather than being sarcoma based [26]. The principal treatment in early and locally-advanced UCS is surgery; because of its aggressiveness [42]. Total hysterectomy and bilateral salpingo-oophorectomy along with surgical staging are the first line in patients without distant metastasis [43]. Staging surgery consisted of total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic and para-aortic lymphadenectomy, peritoneal cytology, and omentectomy [44]. Lymphadenectomy as part of the surgical procedure has shown to prolong survival even for early-stage disease. A combined chemo-radiotherapeutic approach has shown a survival benefit [45]. Surgery and adjuvant RT seem beneficial for excellent LRC rate [46].
There is enough evidence that the most UCSs are monoclonal and that the carcinomatous element is the driving force. Probably the adjuvant chemotherapy should be more similar to that given for a high stage, high grade endometrioid adenocarcinoma or an aggressive histological subtype of endometrial adenocarcinoma, such as serous or clear cell adenocarcinoma [26].
Previous GOG phase III trials have shown a better response to single agent treatment using cisplatin rather than doxorubicin [47,48]. Chemotherapy alone or associated with RT seems to improve disease free survival (DFS) and overall survival (OS) in stage III and IV UCS [42].In the future, the emergence of combination of chemotherapeutic agents with molecular-targeted agents may show promising results [45]. The transcription profile induced by EMT acquires radio-resistance in tumor cells that share the properties of stem cells [49]. Furthermore, research directed toward elucidating the role of vimentin in various signaling pathways would reveal new approaches for the development of therapeutic agents [24].
The endometrial carcinosarcomas are rare aggressive neoplasms. The strict pathohistological and immunohistochemical study is crucial for obtaining diagnosis and determine the need for aggressively complex treatment. Patients with a history of breast carcinoma were subject to periodic monitoring. In case of genital bleeding a separated abrasion with a precise histological study is required. In patients without distant metastases is necessary to conduct a maximal surgical tumor reduction, combined simultaneous chemo-radiotherapy of tumor bed and pelvic lymph nodes. Definitive radiotherapy of para-aortic lymph nodes, as well as chemotherapy are also recommended OS to be improved.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
