
Research Article | DOI: https://doi.org/10.31579/CCOR-2021/003
Obstetrics and Gynaecology, Diana Princess of Wales Hospital/ North Lincolnshire/ Grimsby · Grimsby, GBR.
*Corresponding Author: Deniz AL-Hirmizy, Obstetrics and Gynaecology, Diana Princess of Wales Hospital/ North Lincolnshire/ Grimsby · Grimsby, GBR.
Citation: Deniz AL-Hirmizy, Wood N. , Nugent D. , West R. and Duffy S. (2021) The Effect of Pre-Operative Oral Carbohydrate Loading On Inflammatory Markers in Patients, With Advanced Stage Ovarian Cancer Undergoing Surgery: Randomised Control Trial. Clinical Cancer and Oncology Research 1(1) DOI:10.31579/CCOR-2021/003
Copyright: © 2021, Deniz AL-Hirmizy, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 May 2021 | Accepted: 12 May 2021 | Published: 29 May 2021
Keywords: oral carbohydrate; inflammatory markers; ovarian cancer; randomised trial
Objective: Historically, patients have fasted before elective surgery to ensure an empty stomach to avoid aspiration. However, fasting-induced biological changes may adversely affect the speed of recovery after surgery. In our randomised control trial, we tested the effect of oral carbohydrate loading on the inflammatory markers in patients undergoing major surgery for advanced stage ovarian cancer.
Methods: A double-blinded, single-centre randomised trial was designed to recruit 110 patients with advanced stage epithelial ovarian cancer undergoing either primary surgery, or neoadjuvant chemotherapy prior to debulking surgery (IDS) (reference number: 08/H1306/108). Following informed consent, the patients were randomised into two groups. Group 1 received the carbohydrate drink and group 2 received flavoured water. The volume of fluid in both groups was 800ml the night before the surgery and 400ml two hours before the induction of anaesthesia. We examined the white cell, neutrophil and lymphocyte counts as well as lymphocyte subsets - using a flowcytometry approach.
Results: Between March 2009 and December 2011, 85 patients were approached, 80 patients were randomised and 75 completed the study. A decision was made to close the trial early, as a change in routine clinical practice meant that patients were admitted on the day of surgery rather than a day before. Analysis of the data revealed that oral carbohydrate loading can positively modulate the white cell counts in patients undergoing primary surgery rather than IDS.
Conclusion: In this single-centre study, that failed to recruit the planned number of patients, we found evidence to support that oral carbohydrate intake pre-operatively has some positive influence in enhancing white cell counts in patients with advanced stage ovarian cancer having interval debulking surgery.
Ovarian cancer is the most lethal form of all gynaecological malignancies and the incidence is rising (Redman et al, 2011). This disease mainly affects the older age group of population, who already at a high risk of co-morbidity and a compromised nutritional state. Aggressive treatment modalities, in terms of chemotherapy and extensive major surgery, are the treatment of choice. This warrants optimisation of the general health condition before the treatment of the malignancy - especially prior to surgery.
It has been found that by the avoidance of fasting and dehydration pre-surgery, the post-operative well-being and the clinical outcomes improves significantly (Nygren et al., 2007).
Therefore, Enhanced Recovery Programme (ERP) with the element of pre-operative oral carbohydrate loading may contribute to reduce the stress response caused by surgery, which could adversely affect the well-being of the patient peri-operatively. Thus, this prospective trial aimed to measure the effect of pre-operative oral carbohydrate loading (in patients undergoing surgery for advanced stage ovarian cancer) on the immune system as a marker of patient's recovery post-operatively.
ERP have shown improved results in terms of reduced hospital stay and enhanced surgical recovery ( Kagedan et al., 2015; Nelson, G et al., 2016; Steenhagen, 2016). Since 2006, the use of ERP developed in the field of colorectal surgery (Wind et al., 2006; Kehlet, Henrik, 2008) and became well established. Following this, moves have been made to introduce the ERP into other surgical fields including gynaecology and gynaecological oncology (de Groot et al., 2014).
The immune system consists of a complex network of cells, interacting with each other to regulate our innate and adaptive immunity (Palm and Medzhitov, 2009). Innate immunity is provided by the phagocytes, antigen-presenting cells as well as the members of the T lymphocytes subsets - namely the T cytotoxic and the Natural Killer (NK) cells (Sun and Lanier, 2009; Notes, 2011). Various subtypes of T helper (Th) cells have distinct functions in immunity. The Th1, Th9 and Th17 cells are primarily involved in the launch of pro-inflammatory responses through the production of cytokines. In contrast, the regulatory T lymphocytes are responsible for the suppression of immune responses
through the release of immunosuppressive cytokine interleukin (IL)-10 and transforming growth factors (Spickett, 2006).
The adaptive immunity is the other arm of the immune system, whose T memory cells file records of the nature of the intruding particles or molecules for future immediate immune responses.
Other member of the immune family, namely B lymphocytes, secrete specific antibodies to neutralise and assist in the elimination of the “repeat offenders” by other effectors' immune cells, such as macrophages and granulocytes.
Little is known about the effect of fasting on the components of the immune system. However, it has been reported that 36 hours of fasting is capable of inducing changes in the lymphocyte population with prominent decline in T helper (Th), T cytotoxic (Tc) and B lymphocyte numbers (Meier et al., 2007). Hence, we have examined the effect of administration of oral carbohydrate loading, prior to surgery, on the post–operative immune responses.
Patient population
Ethical approval for the study was granted by the Leeds East Regional Ethics Committee, in October 2008 (REC reference number:08/H1306/108). Potential participants were identified from the weekly Leeds Gynaecological Cancer Centre Specialist Multi-Disciplinary Team meetings (MDT). The study inclusion criteria included patients with presumed stage III/IV epithelial ovarian cancer scheduled for major pelvic surgery, who were willing and able to give written informed consent. Both chemotherapy naïve and post-chemotherapy patients were approached. Exclusion criteria included: 1) diabetes mellitus (type I or type II); 2) any pre-morbid disorder of gastric emptying; 3) morbid obesity (BMI of >50); and/or 4) citrus allergies. Patients were admitted the day before surgery and on admission approached by the researcher, who provided both verbal and written information about the study.
Randomisation
On admission and following written consent, participants were randomised into two groups: routine care (placebo/flavoured water) or pre-operative oral carbohydrate loading (intervention/CHO) - by using sequentially numbered opaque, sealed envelopes containing cards marked “f. water” (flavoured water) or “pre-Op” (oral carbohydrate/CHO). Random number allocation was used to generate 110 sealed opaque envelopes, with allocation to either placebo or intervention (55 cards in each way). These cards were kept with the store of the product of pre-Op ™ and flavoured water, on the gynaecological oncology ward. The clinical fellow (Dal-H) was responsible for drawing sequential envelopes the evening prior to the surgery. Then, the clinical fellow would hand the sealed envelope to one of the nursing staff who was not directly involved in the study - to open it and to decant the assigned drink (pre-Op ™ or f. water).
Intervention
Following randomisation, the appropriate substance (flavoured water or pre-operative oral carbohydrate loading) was decanted into two sterile containers for evening and morning administration by the nursing staff. These were labelled with the patient’s name and kept refrigerated on the ward until administration at the prescribed time. By performing this method, we aimed to ensure “blinding” of the surgical team. 800 ml of the evening drink commenced at 20.00 hours, whilst 400 ml of the morning one was given at 6.00 am for morning surgery and 11.00 am for afternoon surgery.
Data Collection
In order to compare pre and post-operative immunological parameters, blood samples were taken from the participants on the morning of the surgery (D0) and 48 hours post-operatively (D2).
One particular area of interest is the alteration, in the proportion of lymphocyte subsets, in the two patient groups. Lymphocyte subsets can be identified by the expression of specific functional proteins on their cell surface and such proteins are termed the ‘Cluster of Differentiation’ (CD) molecules. All T lymphocytes express CD3 within which, the T helpers co-express CD4 while the CD8 expression is specific for the T cytotoxic subsets. The B lymphocytes are marked by their specific CD19 molecules. The detection of the expression pattern was carried out by the flow cytometry, following the labelling (binding) of the CD molecules of interest by specific antibodies.
1. Labelling of CD molecules
The white blood cells - containing a layer (buffy coat) - which was obtained by the centrifugation of an EDTA-anti coagulated whole blood sample - at 800g for 5 minutes at room temperature. The buffy coat was collected from between the plasma and red blood cells layer using a Pasteur pipette. Contaminated red blood cells were lysed using a hypotonic shock method, based on the higher
Susceptibility of red blood cells to hypotonicity. After 5 minutes in the hypotonic lysis, the remaining white blood cells were collected by centrifugation and subsequently, washed twice in PBS and once in FACS buffer. The washed cells were dispensed into three tubes, which were subject to various treatments (No treatment control [No Rx], isotype control [Iso] and antibodies labelled [Ab]). All antibodies were purchased from BD Biosciences, Oxford, UK. The No Rx control provided the cells for background setting, while the isotype controls served for the detection of non-specific binding. This treatment was performed at room temperature for 30 minutes. The cells were then washed two times in PBS, fixed in Cytofix® and kept at 4Cᵒ in dark until analysis (within 24 hours). Using the LSRII (BD Biosciences).
The antibodies used in the experiments are tagged with fluorochrome labels emitting fluorescence at specific energy levels, which can be detected by the flow cytometer as its demonstrated in table 1.

2. Flow cytometry settings
The operating procedures for the analysis of CD expression patterns (by flow cytometry) involved various focusing (termed gating) steps. Firstly, various white blood cells were identified by their specific properties in the scattering and transmission of a beam of laser - which the cells were sent through. The lymphocyte population was then gated, according to their relatively smaller sizes and low granularity which determine the side and forward scattering of the laser (Figure 1).
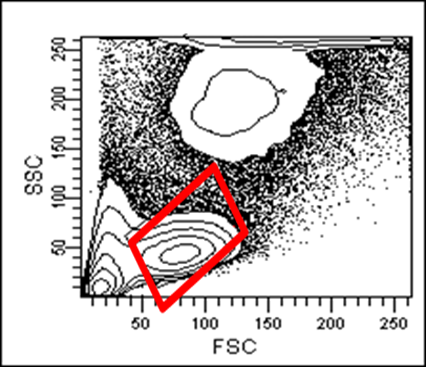
FSC= forward scatter SSC= side scatter
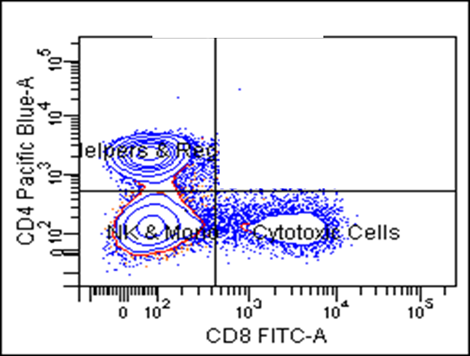
Within the lymphocyte gate, cells were then analysed for their levels of CD [removed]Figure 2).
The levels of fluorescence are directly proportional to the levels of CD molecules being expressed by the cells. The No Rx and Iso controls were used for the setting of the forward, side scatter channels and baseline
fluorescence levels (usually between 102 to 0.5 x 103). Cells appearing below the baselines were regarded as being negative for the parameter being studied. In figure 2, the lower left quadrant contains the cells with no CD3 or CD19 expressions. CD3 (T lymphocytes) appear in the left upper quadrant. The lower right quadrant contains the cells expressing no CD4 but high CD19 levels, thus they are B lymphocytes.
A further gating was then set to include the CD3 positive cells only. This CD3 positive population was then further analysed for their CD4 and CD8 expressions (Figure 3).
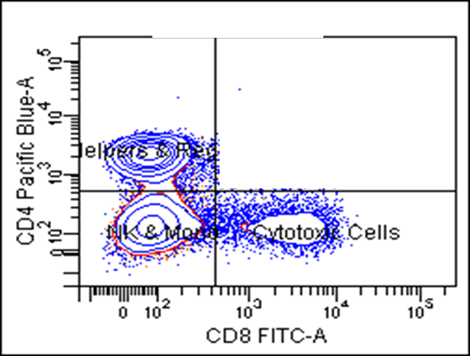
In figure 3, the lower left quadrant has the CD3 positive but no CD4 expression pattern. There is a possibility that these are the Natural Killer (NK) cells. However, NK cells can only be accurately identified by their expression of other NK-specific markers such as CD18 and Perforins. The T helper lymphocytes (CD4 positive) and the T cytotoxic (CD8) cells are shown in the upper left and the lower right quadrants respectively. A flow cytometer has the capability of analysing a large number of cells in a short period of time. In order to achieve statistical confidence on each sample analysis, the number of cells to be examined (event) was set to either 10,000 or 20,000 - depending on the amount of cells available.
The LSRII flow cytometer was calibrated by the LIMM FACS facilities staff every morning, using calibrator beads with standardised fluorescent intensities for each detection channels.
We have looked at White Blood Cells (WBC), Neutrophil and Lymphocyte counts in addition to the Neutrophil/Lymphocyte Ratio (NLR) and Lymphocyte subsets (T helper, T cytotoxic, B-lymphocyte and T regulatory). The blood samples for the parameters above were collected on the Day of surgery, just before the operation (D0) and on Day two post-operatively (D2). These blood results were obtained from St. James's hospital, University of Leeds/ NHS laboratory.
100% of the data for the WBC counts were analysed (75/75 pairs). Whilst for the neutrophil counts 72/75 pairs were analysed because three patients (one from the CHO group and two from the placebo group) had their blood samples haemolysed. The remaining 72 pairs of blood samples accounted for 96% of the total. For the Lymphocyte counts, one patient's blood sample was damaged with the remaining samples available to analyse and this represented 98.6% of the total (74/75 pairs).
1. WBC (normal reference value is = 4-11 X 10⁹/L).
There were outliers from the normal range of WBC counts for both study groups in pre (day 0) and the post-operative period (day 2). Most of the patients with low WBC count (<4>
Those outliers who entered the trial with high WBC counts (> 11 x 10⁹/L) were clinically fit for surgery and showed no signs or symptoms of infection.
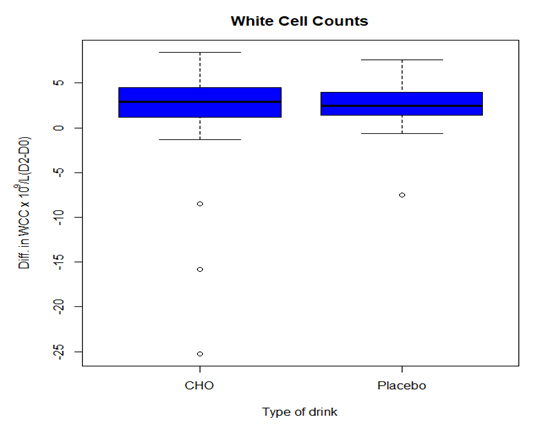
Since then, we collected data on WBC counts for day 0 (pre-operative) and day two post-surgery, we calculated the mean of differences between the two days (Day 2-Day 0) for both study groups [CHO group (n=38)(mean= 1.69) and placebo group (n=37)(mean= 2.58)]. A student's t test was performed on the two sets of data and revealed no significant statistical difference between the study groups (Table 2).
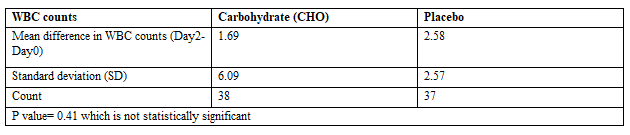
In addition, we have run an analysis on the WBC counts for both study groups - following the exclusion of all the WBC values outside the normal range (4-11 x 10⁹/L). We obtained the same results of no statistical significance between the two study groups.
However, additional analysis of the WBCs for day 0 pre-operatively and day 2 post-operatively were based on the type of surgery for the subgroups of IDS and PDS. They had revealed the following: there was a significant difference of WBCs in the IDS subgroup (between CHO and placebo) for D0 (p=0.040) in favour of the CHO group. This finding was not the same for D2 (p=0.170). Conversely, no significant differences were found in the PDS subgroup (in between the CHO and placebo) for D0 (P=0.440) or D2 (P=0.630) respectively.
2. Neutrophil counts (Normal range (1.5-8.0) x 10⁹/)
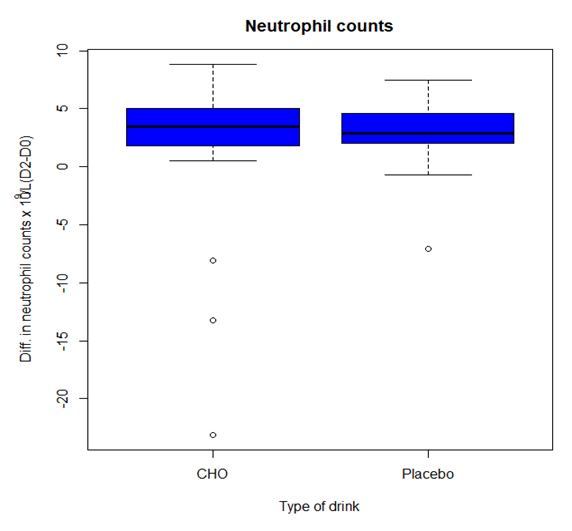
Three patients from both study groups (DH14 from the CHO group and DH11 & DH15 from the placebo group) were excluded from the analysis as the blood samples were haemolysed. Therefore, the total number of analysed samples were 72 pairs, 37 in the CHO group and 35 in the placebo group respectively. We calculated the mean of the differences between pre (Day 0) and post-operative (Day 2) of the study groups (Day 2-Day 0). The mean value for the CHO group was 2.03 and for the placebo group, it was 3.22 - with a calculated p value of 0.48. Therefore, no statistical
Significance was found between the two study groups when the significance of the p value was set to be p< 0>

3 . Lymphocyte counts Normal reference value for the lymphocyte counts is (0.8-3) x 10⁹/L
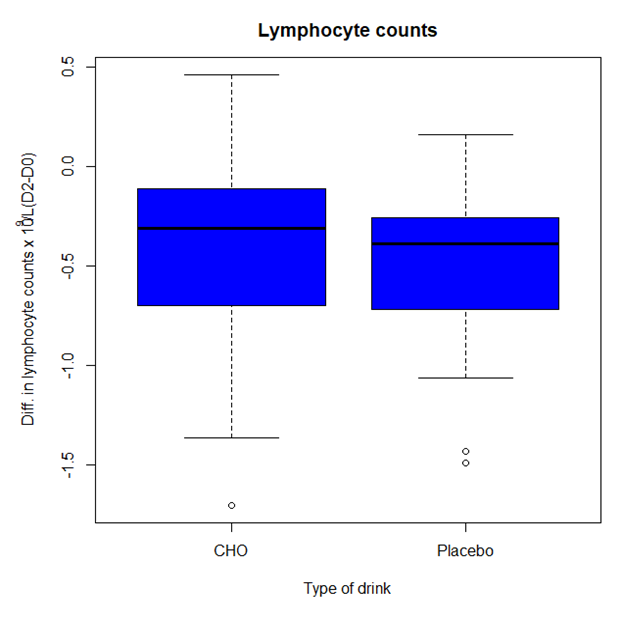
One patient from the intervention/CHO group (DH14) had to be excluded from the analysis of the absolute number of lymphocyte counts as the blood sample was haemolysed. Therefore, the total analysed number of lymphocyte counts for the CHO was 37 and for the placebo group was 37. We looked at the mean value of difference of lymphocyte counts between the pre (Day 0) and post-operative (Day 2) for both study groups. The mean value for the CHO group was -0.41 and for the placebo group was -0.48 respectively. A Student's t test was performed on two sets of data for CHO (Day 2-Day 0) versus placebo (D2-D0) with a p value of 0.48 found. This concluded that there was no statistical significant difference between the study groups (Table 4).

4. Neutrophil/Lymphocyte ratio (NLR)
This parameter has been used as a marker for subclinical inflammation, therefore we have included it in our analysis. The same method of analysis was conducted on this parameter as above. We compared the mean difference of NLR between Day 2 and Day 0 for each study group; CHO (n=37) with mean value of 5.17 and placebo (n= 35) with mean value of 5.11. A calculated Student's t test with a p value of 0.96 revealed that no statistical significance was identified between the study groups (Table 5).

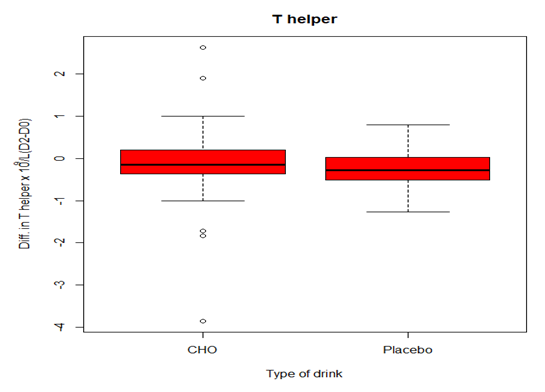
5. Lymphocyte subsets
The lymphocyte subsets (T helper, T cytotoxic, T requlatory and B lymphocyte) data were obtained by performing flowcytometry. We conducted this analysis in the Wellcome Trust Brenner Building/Research institute in St James's University Hospital in Leeds.
Forty two patients (21 from each group) from the total (n=75) patients, who completed the trial, were selected randomly for lymphocyte subset analysis. This was due to limited resources. A preliminary statistical
analysis on the flowcytometry data was required for the purpose of experimental design. This was carried out on the first twenty eight patients (n=28) from both study groups. Following this initial analysis, we noticed that adding another lymphocyte subset (T regulatory) to reflect on the function, rather than only the count of the immune system, was an important step to be undertaken. Therefore, the total number of T regulatory cells was even lower than the rest of lymphocyte subsets.
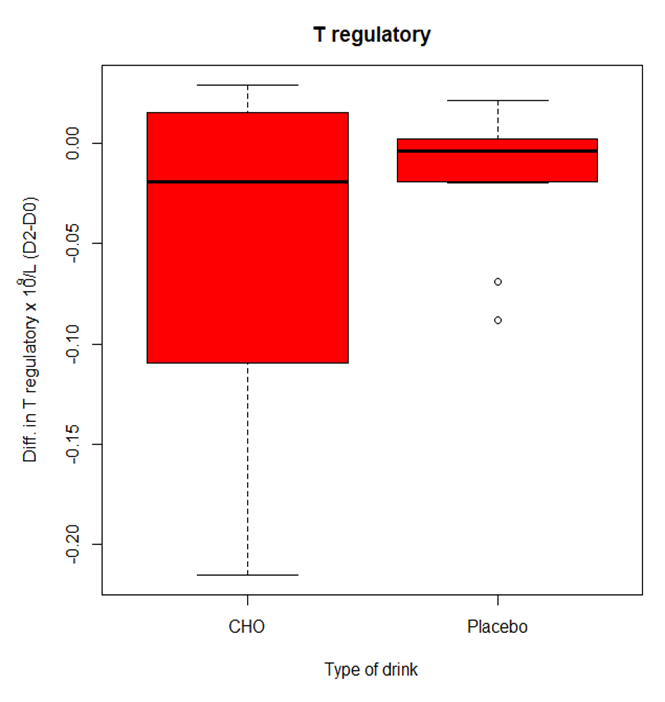
A total number of nineteen patients could be recruited for the analysis of the T regulatory lymphocyte cells (n=19) (CHO=8 and placebo = 11).
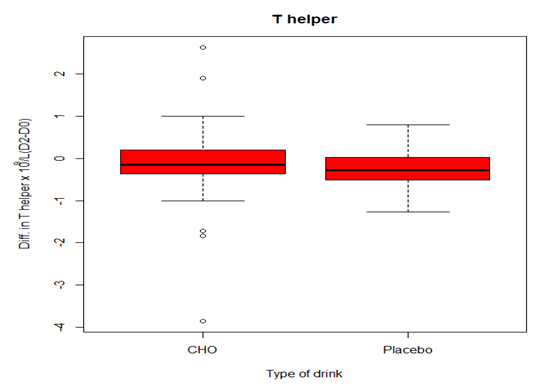
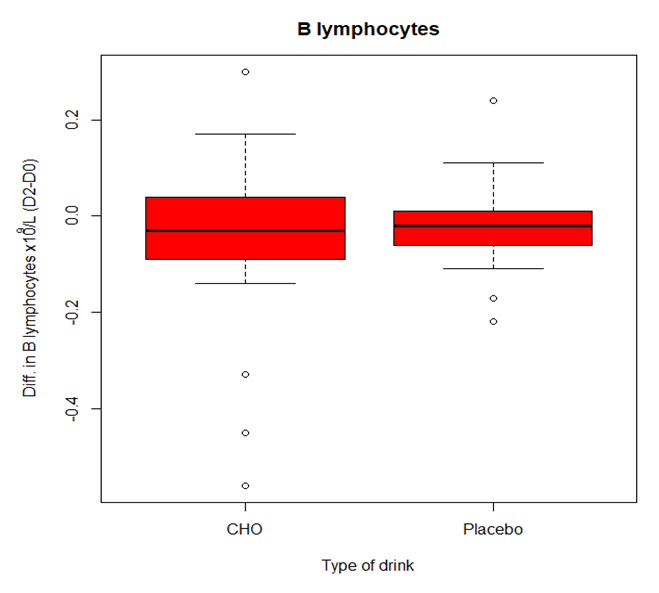
Table 6 shows that no statistical significant differences were found in the mean differences of Day 0 to Day 2 subsets between patients receiving the CHO loading or the placebo drink - with respect to T helper lymphocytes (p=0.83), T- cytotoxic lymphocytes (p=0.72), T- regulatory lymphocytes (p=0.19) or B lymphocytes (p=0.64).
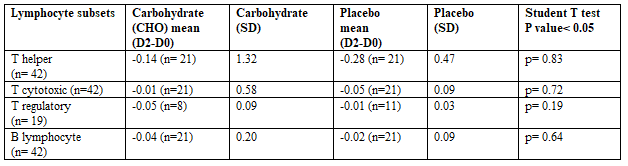
SD= Standard Deviation
The analysis of our immunological data revealed that there were no significant differences between the two study groups (CHO, placebo) with respect to White Cell Counts (WCC), lymphocyte counts, neutrophil counts and the neutrophil/lymphocyte ratio. The baseline bloods for the above markers were taken on D0 prior to surgery, then on 48 hours after the surgery (D2). 75 pairs of blood samples for the WCC, 72 pairs for the neutrophil counts (three sample pairs were excluded due to haemolysis) and 74 pairs for lymphocyte counts as well as for the neutrophil/ lymphocyte cells ratio (one pair of the sample were excluded due to haemolysis). The mean value of the difference between (D2-D0) was obtained and compared between both study groups.
Further analysis of WCC had shown that four (4) patients from both study groups (3 patients from the CHO group and 1 patient from the placebo group) had elevated the pre-operative total of the WCC which returned to the normal range - 48 hours after surgery (an observation which could be explained by the general impact of surgery and immunosuppression). Clearly those patients were well enough to continue having their surgery, therefore they were included in the analysis; as well as all the patients with low WCC (please see an explanation on the WCC in the results section). However, when we analysed the data of the total WCC, excluding the patients with high WCC, we still found that there was no significant differences in the WCC mean score - between the two study groups.
Since chemotherapy compromises the overall immune function of the body and since more than half of our study population had chemotherapy prior to having surgery (which can synergise the immunosuppression process), we have justified an ad-hoc analysis of the WCC in the subgroups, based on the type of surgery, whether patients received IDS or PDS as part of their management plan. However, this time we analysed the WCC data on D0 and D2 for both study groups. The findings stated that there was a significant difference of the WCC in the IDS subgroup - between the CHO and the placebo for D0 (p=0.04) in favour of CHO - but this finding was not the case for D2 (p=0.17) respectively. On the other hand, no significant difference was seen in the PDS subgroup between the CHO and the placebo for D0 (P=0.44) or D2 (p=0.63).
The possible explanation is that the pre-operative oral CHO drink potentially boosts the already compromised immune activity of the IDS population, prior to having surgery. However, there was no obvious effect on D2, which could be potentially explained by an inability to counteract the profound
Immunosuppression as a result of major surgery. Also, to a lesser extent, it could be due to a variable approach to the nutritional support post-operatively (non-uniform post-operative operating team care package).
In cancer surgery, the lymphocyte subsets - especially the T-cells of the immune system - would be the first impacted at the time of surgery and immediately afterward. An intact immune system - with the full complement of the T cytotoxic and T helper (subsets of T cells) - has an important role in fighting cancer and its metastasis (Shakhar and Ben-Eliyahu, 2003; Snyder and Greenberg, 2010).
Humoral immunity, mainly represented by B lymphocytes, has a crucial role in the eradication of bacterial pathogens and fighting infection. B cell proliferation and differentiation are affected by a number of cytokines - as well as the B cells themselves that produce a variety of cytokines including IL-10 (Lund, S.A. et al., 2009; Lund, F.E. and Randall, 2010).
Twenty one (21) participants from each study group were included in the analysis for lymphocyte subsets, specifically T helper, T cytotoxic and B lymphocytes. This sub-sample of 42 patients in total, were only analysed as a result of the limited time and laboratory resources. It was found that there were no significant variations between the study groups, in regards to the lymphocyte subsets. T regulatory cell population (another subtype of lymphocyte cells) was added half way through the recruitment process - following a preliminary analysis of T cells, in an attempt to gain more information on the immune function rather than the cell count only. This subpopulation was analysed in the same way as above and we found that there was no significant difference between the study populations.
The interpretation of the immunological variables has limitations, including: small sample sizes and even smaller sizes with the lymphocyte sub-population; the different timing of blood samples (circadian rhythm); IDS and its association of chemotherapy's effect in the groups; and the variable degree of severity of surgery. Despite this, we found evidence to support that oral carbohydrate intake pre-operatively has some positive influence in enhancing white cell counts in patients with advanced stage ovarian cancer having interval debulking surgery.
In future studies, testing blood samples for inflammatory markers for longer than 48 hours (which may be up to 7 days) probably is required, in the context of using the full package of the ERAS programme, to improve our understanding of the immunological effects.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
