
Research Article | DOI: https://doi.org/10.31579/2578-8965/154
Department of Obstetrics and Gynecology, Faculty of Medicine - Ain-Shams University, Cairo, Egypt.
*Corresponding Author: Osama S. Badawi, Department of Obstetrics and Gynecology, Faculty of Medicine - Ain-Shams University, Cairo, Egypt.
Citation: Mohamed A. Al-Senity, Osama S. Badawi, Karim Wahba, Tamer El Refaei, Mohamed Essmat (2021), The Effect of Laparoscopic Ovarian Cystectomy for Endometrioma on Ovarian Reserve in Patients with Infertility (a Prospective Cohort Study). J. Obstetrics Gynecology and Reproductive Sciences, 5(9) DOI: 10.31579/2578-8965/154
Copyright: © 2021 Osama S. Badawi, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 September 2021 | Accepted: 13 October 2021 | Published: 25 October 2021
Keywords: laparoscopic ovarian cystectomy; endometrioma; ovarian reserve; infertility
Background: Endometriosis, the presence of endometrial tissue outside the lining of the uterine cavity, is one of the most common pelvic diseases in women. It is generally acknowledged that an estimated 6–10% of all women during their reproductive years are affected by this condition.
Objective: to evaluate the effect of laparoscopic ovarian cystectomy for endometrioma on ovarian reserve in patients with infertility.
Design: This study was conducted on 34 women with infertility undergoing laparoscopic ovarian cystectomy for endometrioma at Ain Shams University Maternity Hospital in the period between August 2017 and August 2019,4 patients were excluded by postoperative histopathological exclusion of endometrioma. Ultrasound and biochemical markers of ovarian reserve were measured preoperatively and 1 month postoperatively.
Results: There was a highly significant difference between pre and post intervention AMH, FSH, Estrogen, AFC and ovarian volume.
Conclusion: However, Laparoscopy is extremely useful in the diagnosis and treatment of endometriomas. We concluded that laparoscopic ovarian cystectomy of endometrioma led to significant decrease of AMH levels, AFC and ovarian volumes. It also led to significant increase of FSH and estrogen levels which indicates the possible deleterious effect of laparoscopic ovarian cystectomy for endometrioma on ovarian reserve and subsequently on fertility and live birth rates
Our understanding of endometriosis is incomplete, and controversy continues regarding management of endometriosis. Surgery has a fundamental role to play in the treatment of endometriomas (Hart RJ et al., 2018). The damage to ovarian reserve inflicted by surgery represents a major concern in the balance between reproductive benefits and risks. The absence of a clear plane of cleavage between the cyst and ovarian stroma could result in unintentional removal of the ovarian cortex and loss of follicles with potential reduction in follicular reserve. Injury may be inflicted to ovarian stroma during hemostasis by electrosurgical coagulation (Li CZ et al., 2009).
A true ovarian reserve is the number of primordial follicles present in the ovaries. Ultrasound and endocrine measures have been widely accepted as markers of ovarian reserve. (Tsolakidis D et al., 2010) The endocrine markers such as follicle-stimulating hormone (FSH), E2, inhibin B and anti-Müllerian hormone (AMH) provide information on ovarian reserve of both ovaries as a combined unit, therefore using them as markers of ovarian reserve is still questionable, especially because most cysts are unilateral and that the intact contralateral ovary can adequately compensate for the affected one in terms of function (Ercan CM et al., 2013). Ultrasound assessment of the total number of antral follicles, ovarian volume and ovarian stromal vascularity are important determinants of ovarian reserve as affected ovary’s reserve can be assessed independent of compensation by unaffected normal ovary (Scheffer GJ et al., 2002). Inadvertent removal of normal ovarian tissue can be studied by histopathology of excised cyst wall (Hashisuga T et al., 2002)
Laparoscopic cystectomy is the gold standard surgical technique of clinical care for women with endometriosis and pelvic pain or infertility. For years, a debate has been under way as to the most appropriate technique for surgical treatment of endometriomas, comparing the most commonly used techniques (Muzii et al., 2002) cystectomy, fenestration and bipolar coagulation, or fenestration and laser vaporization of the cyst wall or two or three step techniques (Tsolakidis et al., 2010). These techniques are usually evaluated in terms of their effect on symptomatic relief, the ovarian reserve, pregnancy rate and the risk of recurrence (Muzii et al., 2005). There are significant concerns about the potential deleterious effects on ovarian reserve. Endometrioma surgery carries the risks of 2.4% postsurgical ovarian failure and 30.4% disease recurrence (Busacca et al., 2006). A successful operation means not only removal of ovarian pathology, but also maintenance of ovarian function and subsequent pregnancy.
This studied aimed to evaluate the effect of laparoscopic ovarian cystectomy using stripping technique for endometrioma on ovarian reserve in patients with infertility.
Patients and Methods
Type of the study
prospective cohort study
study setting
Ain Shams University Maternity Hospital
Study period
From August 2017 to August 2019
Study population
The study included 30 women with infertility undergoing laparoscopic ovarian cystectomy for endometrioma.
Inclusion criteria
The study included patients with ages from 18-39 years, BMI 18-29 Kg/m2, regular menstrual cycle every 21-35 days at the time of the operation, complaint of infertility of any duration, ovarian endometrioma, diagnosed by transvaginal ultrasonography (ACOG practice bulletin no. 114, 2010) as adnexal mass with ground glass echogenicity of the cyst fluid (low-level, homogeneous internal echoes consistent with old blood), one to four locules and no papillations with detectable blood flow (Dunselman et al ,2014), persistent cysts for more than two menstrual cycles and measuring more than 3 cm (ACOG practice bulletin no. 114, 2010), histopathological diagnosis of excised ovarian tissue confirmed postoperatively to be an endometriotic cyst and written and signed informed consent by the patient to participate in the study.
Exclusion criteria
The following patients were excluded from the study: Age more than 39 years, BMI more than 29 Kg/m2, polycystic ovary syndrome, diagnosed – according to the revised 2003 consensus on diagnostic criteria of polycystic ovary syndrome by the Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group (Chang et al., 2004), Evidence of any other endocrine disorder such as diabetes mellitus, thyroid dysfunction, hyper-prolactinemia, congenital adrenal hyperplasia, Cushing’s syndrome or adrenal insufficiency, Evidence of premature ovarian failure, i.e. persistently elevated or serially rising FSH levels (Beck-Peccoz et al., 2006), previous history of adnexal surgery, Having any suspicious findings of malignant ovarian disease, Histopathological diagnosis of excised ovarian tissue confirmed postoperatively to be a non-endometriotic cyst, Any hormonal treatment or oral contraceptive pills during the last three months before enrollment, Intraoperative conversion to exploratory laparotomy, Any contraindication to laparoscopy, Any chronic medical disorder, e.g. hypertension, autoimmune disorders, … etc, Mental condition rendering the patients unable to understand the nature, scope and possible consequences of the study.
All subjects were subjected to the following:
Pre-Enrollment Assessment
Proper history taking, examination and investigations to: ensure the diagnosis of endometrioma, exclude other causes of hormonal imbalance. Menstrual history: to exclude oligo- or anovualtion. Past history: any history of previous adnexal or pelvic surgery, OCP or hormonal treatment. Clinical examination, including: Assessment of hirsutism via modified Ferriman-Gallwey score Assessment of alopecia and acne. Assessment for any signs of endocrine disease. Assessment of abdominal and pelvic scars of previous operations for planning of laparoscopy. Transvaginal ultrasonography: by the same experienced gynecological sonographer using a Voluson E6 Expert ultrasound machine (General Electric®, Fairfield, CT, USA) for U/S criteria of endometrioma (see before) and exclusion any uterine or pelvic pathologies.
Assessment of Preoperative Ovarian Reserve
Preoperatively on day 2 of menses, AMH, FSH, luteinizing hormone (LH) and E2 levels were measured.
Preoperatively on day 2 of menses, ovarian and endometrioma volumes, antral follicle counts (AFCs) and stromal blood flow (peak systolic flow) were assessed.
Laparoscopic Ovarian Cystectomy Using the Stripping Technique
All the ovarian cystectomies were performed by the same team of surgeons using the stripping technique as described by Ramachandran et al 2013.
Participants underwent the operation under general anesthesia. Using a Verres needle passed through a 1cm umbilical incision, pneumoperitoneum was induced by CO2 insufflation to maintain an intra-abdominal pressure of 12 mmHg. Umbilical 10mm trocar and telescope were introduced to guide the insertion of 2-3 additional 5mm trocars through supra-inguinal incisions.
After exploration of pelvic cavity and visualization of ovarian cysts, endometriosis was staged according to revised American Society of Reproductive Medicine classification (Canis et al 1996).
After mobilization and grasping of the ovary with forceps, an incision was made on the antimesenteric surface, away from the ovarian hilus. After identifying the correct plane of cleavage between the cyst wall and the ovarian tissue, traction was applied; strong, but nontraumatic with two grasping forceps, so that, the inner lining of the cyst is stripped from the normal ovarian tissue.
No ovarian tissues were resected in order to identify the plane. The bed of the cyst carefully was inspected to detect possible bleeding zones that may require coagulation with bipolar forceps avoiding excessive diathermy. No sutures were used for ovarian reconstruction.
Postoperative Assessment of The Ovarian Reserve
Histopathological evaluation of excised cyst wall. The endometrioma wall was evaluated histologically. The slides were reviewed by the same pathologist, who is blind to the clinical variables of the patient. Routine hematoxylin and eosin staining were used on the sections for histopathologic examination. For the diagnosis of endometriosis, the criteria of the technical bulletin on endometriosis of the American College of Obstetricians and Gynecologists were followed (ACOG practice bulletin no. 114, 2010).
All patients were followed-up postoperatively on day 2 of the next menses for their second evaluation. Ovarian reserve was rechecked by measuring ovarian volume, AFC, stromal blood flow by ultrasound and AMH, FSH, LH and E2 levels.
Statistical analysis
Statistical analysis was performed using Microsoft Excel® 2007 and statistical package for social sciences (SPSS® version 15.0). Data were prescribed as range, mean and standard deviation (for parametric variables), range, median and interquartile range (for non-parametric variables), and number and percentage (for categorical variables). Difference between variables of two groups was analyzed using student’s t-test (for non- parametric variables) and Chi-squared test (for categorical variables). Difference between variables of more than two groups was analyzed using oneway ANOVA test (for parametric variables), Kuskal Wallis test (for non-parametric variables) and Chi-squared test (for categorical variables). Correlation between two variables was estimated using Pearson’s correlation coefficient (for parametric variables) and Spearman’s rank correlation coefficient (for non-parametric variables). Significance level was set at 0.05.
Ethics and legal data
Before the beginning of the study and in accordance with the local regulation followed, the protocol was declared for the Ethical and Research approval by the Council of the OB/GYN Department, Ain Shams University. Furthermore, the approval of the study protocol was granted by Ethics Research Committee, Faculty of Medicine, Ain Shams University. Before being admitted to the clinical study, informed consent was taken from all patients after explaining the nature and scope of the clinical study.
Results
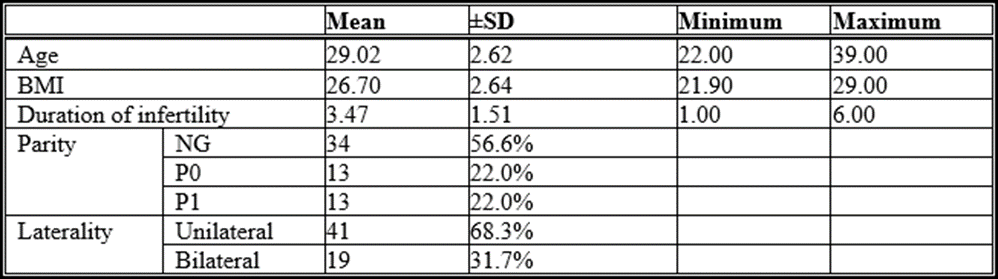
Table 1: Demographic characteristics.
The above table shows that the mean age among study cases was 29.02± 2.6, and the mean BMI was equal to 26.7± 2.64. The duration of infertility was 3.4± 1.5 years. More than half of cases were nulligravida (56.6%). Unilateral case represented 68.3% of cases
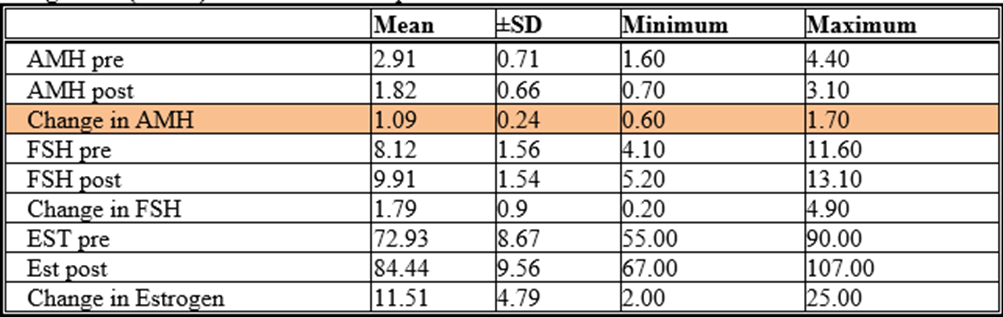
Table 2: Description of hormonal profile before, after and the change after intervention among cases group

Table 3: Description of AFC before, after and the change after intervention among cases group
*Inter quartile range

Table 4: Description of ovarian volume before, after and the change after intervention among cases group
Note >> ov vol pre op was including endo cyst
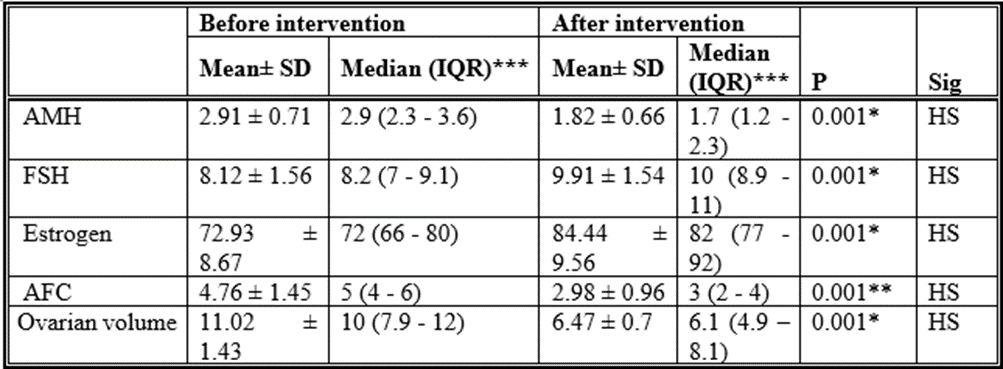
Table 5: Comparison between before and after intervention hormonal profile, AFC and ovarian volume There was a highly significant difference between pre and post intervention AMH, FSH, Estrogen, AFC and ovarian volume.

Table 6: Comparison between cases according to affected side as regard AMH before and after intervention and change after intervention
*Student t test
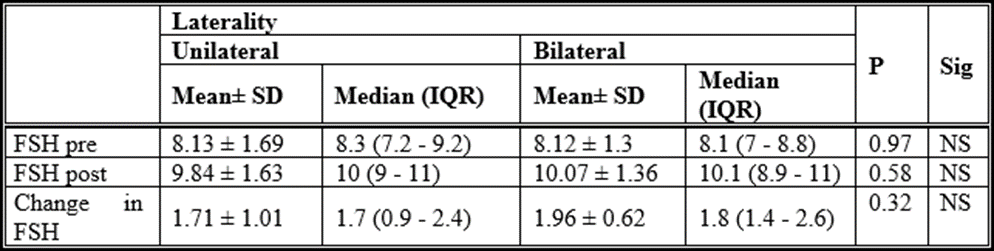
Table 7: Comparison between cases according to affected side as regard FSH before and after intervention and change after intervention
*Student t test
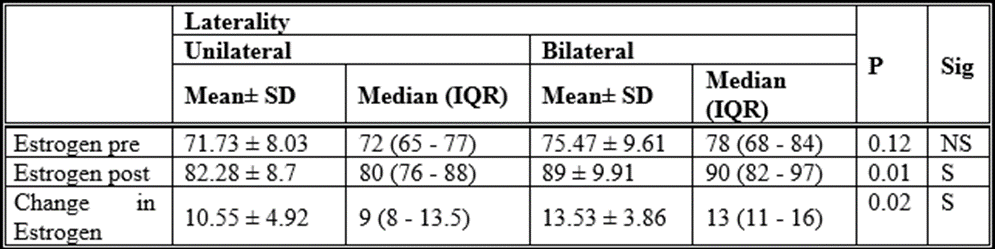
Table 8: Comparison between cases according to affected side as regard Estrogen before and after intervention and change after intervention
*Student
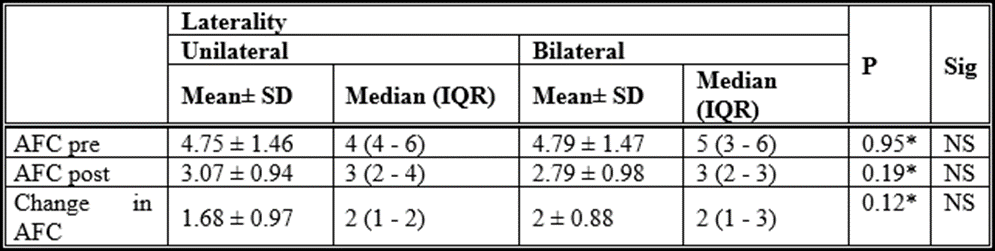
Table 9: Comparison between cases according to affected side as regard AFC before and after intervention and change after intervention
*Mann Whitney test
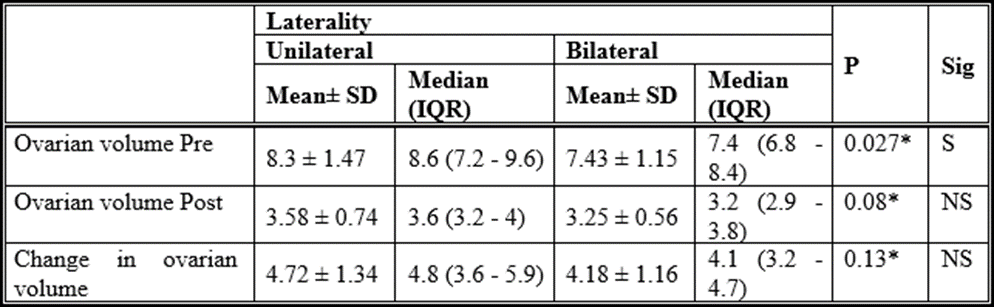
Table 10: Comparison between cases according to affected side as regard Ovarian volume before and after intervention and change after intervention
*Student t test
Statistical analysis of this study results showed that there were highly significant differences between AMH levels (2.91 ± 0.71 vs. 1.82 ± 0.66); (P= 0.001) before and after intervention. There was no significant difference between cases according to affected side as regard AMH before and after intervention and change after intervention (1.12 ± 0.23 vs. 1.05 ±) (P= 0.31).
Abd El-Aal et al (2018) study evaluated the effects of laparoscopic cystectomy on ovarian reserve in patients with endometriomas. This prospective study was conducted on 44 cases suffering from ovarian endometriomas and subjected to laparoscopic cystectomy. The patients in the study were selected from the Outpatient Clinic in Sayed Galal University Hospital and EL-Gala Maternity Teaching Hospital. This study was conducted between April 2017and March 2018. Serum anti-mullerian hormone (AMH), FSH and E2, as well as the antral follicle count (AFC) were measured preoperatively and 3 months postoperatively. They agreed with results of current study and stated that the serum levels of AMH decreased significantly (P<.001) postoperatively (0.1-4.8 vs. 0.1-3.6).
Amooee et al (2015) study investigated serum level of anti-mullerian hormone (AMH) as an indicator of ovarian reserve before and after surgical cystectomy. 60 patients with dermoid cyst, serous cystadenoma, and mucinous cystadenoma were recruited. Measurement of serum AMH was performed prior to surgery, and at one and 3 months after laparoscopic cystectomy. Serum AMH levels were compared before and after the surgery and between various types of ovarian cyst. They were in line with current study results and stated that serum AMH level declined significantly after the surgery which recovered to 65% of its baseline value three months later. AMH levels in studied population before the operation showed a mean value of 3.77 ng/mL (95% CI: 1.58-5.96 ng/mL) which declined to 1.87 ng/mL (95% CI: 0.67-3.07 ng/mL) 1 month after the operation. This decline was significant with the p:<0>
Chen et al (2014) study evaluated the impact of the presence of endometrioma and laparoscopic cystectomy on ovarian reserve as assessed by serum anti-Müllerian hormone (AMH) level. In addition, factors related to the decline in ovarian reserve were analyzed. 40 women were prospectively included with endometriomas as the study group (group A), 36 women with tubal factor infertilities as control group 1 (group B) and 22 women with the other benign ovarian cysts as control group 2 (group C). The women with ovarian cysts underwent laparoscopic cystectomy. Serum AMH levels were determined preoperatively and at 1 month after surgery. They agreed with us and stated that the endometrioma group had lower AMH levels (1.53 ± 1.37 ng/ml) compared with the other benign ovarian cyst group (2.20 ± 1.23 ng/ml) and the tubal factor infertility group (2.82 ± 1.74 ng/ml). The rate of serum AMH decline 1 month after surgery in the endometrioma group (0.62 ± 0.35) was larger than the decline in the other benign ovarian cyst group (0.32 ± 0.30). The preoperative AMH level showed a significant correlation with patient age (group A, r = −0.32; group B, r = −0.54; group C, r = −0.71); there was a statistically significant correlation between the rate of serum AMH decline and endometrioma diameter as well as with the preoperative serum AMH level. In addition, the rate of serum AMH decline was larger for bilateral endometriomas than for unilateral endometriomas, but there was no similar correlation in the other benign ovarian cyst group. The rate of AMH decline after surgery in the subgroup of >7 cm was significantly higher than in the subgroup of ≤7 cm.
Tanprasertkul et al (2014) study evaluated the impact of laparoscopic ovarian cystectomy for endometrioma on ovarian reserve, measured by serum antimullerian hormone (AMH), compared to nonovarian pelvic surgery. A prospective study was conducted. In this study, 90 women were enrolled. There were thirty-nine and 38women in laparoscopic ovarian cystectomy (LOC) and laparoscopic nonovarian pelvic surgery (NOS), respectively. Women who underwent laparoscopic ovarian cystectomy (LOC) and laparoscopic nonovarian pelvic surgery (NOS) were recruited and followed up through 6 months. Clinical baseline data and AMH were evaluated. After surgery, AMH of both groups decreased since the first week, at 1 month and at 3 months. However, as compared to the LOC group at 6 months after operation, the mean AMH of the NOS group had regained its value with a highly significant difference. They also agreed with us and stated that the distribution of serum AMH levels was inversely correlated to the patients’ age. After age of 40, the rate of declination was accelerated.
Alborzi et al (2014) study evaluated the effects of laparoscopic cystectomy on ovarian reserve in patients with endometriomas. In this prospective study, 193 patients with endometriomas, referred to private and university hospitals of Shiraz University of Medical Sciences, who underwent laparoscopic ovarian cystectomy. The patients were divided into four groups according to age (8 or >38 years of age), size of the cyst (>3 cm, Hwu et al (2011) study evaluated the impact of endometrioma and laparoscopic cystectomy on ovarian reserve as measured by serum AMH levels. A total of 1,642 patients were recruited in this retrospective analysis. Control group (group 1) included 1,323 infertility patients without endometrioma. Endometrioma group (group 2) included 141 patients with ovarian endometrioma. Previous cystectomy group (group 3) included 147 patients who underwent unilateral or bilateral laparoscopic cystectomy due to ovarian endometrioma more than 6 months before enrollment. Current cystectomy group (group 4) included 31 patients who underwent cystectomy during study period. Serum antimüllerian hormone (AMH) levels were measured upon enrollment with all patients. For patients in group 4; AMH levels were measured before and 3 months after cystectomy. They corresponded with the results of current study and stated that mean AMH level of patients in control group was significantly higher than that of endometrioma group or previous cystectomy group in each age subgroup, while the mean serum AMH level of the endometrioma group was also significantly higher than that of the previous cystectomy group in each age subgroup. The mean AMH level was significantly lower in patients with previous bilateral cystectomy compared to that of patients with unilateral cystectomy. The mean serum AMH level was also significantly lower in patients with bilateral endometrioma compared to that of patients with unilateral endometrioma. In group 4, mean AMH level significantly decreased from 3.95 +/- 0.42 preoperation to 2.01 +/- 0.21 ng/ml at 3-month postoperation. There were highly significant differences between FSH levels (8.12 ± 1.56 vs. 9.91 ± 1.54); (P= 0.001). There was no significant difference between cases according to affected side as regard change after intervention (1.71 ± 1.01 vs. 1.96 ± 0.62) (P= 0.32). Abd El-Aal et al (2018) study agreed with results of current study and stated that the serum levels of FSH increased significantly (P<.001) postoperatively (0.1-4.2 vs. 1.8-5.2). Bhat et al (2014) study evaluated the ovarian reserve in sub fertile women after laparoscopic endometriotic cystectomy. A Prospective study was conducted on a total of 85 patients. Laparoscopic cystectomy was performed by stripping technique for endometriotic cysts. Endometriosis was staged according to revised American Society of Reproductive Medicine classification (rASRM). Ovarian reserve assessed by comparing FSH and LH levels, measurement of residual ovarian volume, antral follicle counts and stromal blood flow on second day of menses pre and postoperatively. Cyst wall was evaluated histologically to note the presence of normal ovarian tissue in resected tissue. They disagreed with current study and stated that there was no significant difference between pre and postoperative values of FSH levels. Mean day 2 FSH levels pre and postoperatively were (7.24 ± 1.21 mIU/ml and 7.23 ± 1.51 mIU/ml) (P= 0.29). It is due to different methodology and sample size. Alborzi et al (2014) study agreed with current study and stated that the serum levels of FSH increased significantly 3 months (P =.039) after the operation. There were highly significant differences between Estrogen levels (72.93 ± 8.67 vs. 84.44 ± 9.56); (P= 0.001). There was a significant difference between cases according to affected side as regard Estrogen before and after intervention and change after intervention (10.55 ± 4.92 vs. 13.53 ±) (P= 0.02). Abd El-Aal et al (2018) study disagreed with results of current study and stated that the serum levels of Estrogen decreased significantly (P<.001) postoperatively (8-60 vs. 3-52). Alborzi et al (2014) study disagreed with current study and stated that the serum level of E2 remained unchanged (P =.318). There were highly significant differences between AFCs (4.76 ± 1.45 vs. 2.98 ± 0.96); (P= 0.001). There was no significant difference between cases according to affected side as regard change after intervention (1.68 ± 0.97 vs. 2 ± 0.88) (P= 0.12). Abd El-Aal et al (2018) study agreed with results of current study and stated that the AFCs decreased significantly (P<.001) postoperatively (5-16 vs. 2-9). Bhat et al (2014) study agreed with us and stated that there was significant difference between pre and postoperative AFCs (3.3 ± 1.9, 4.1 ± 1.5) (P=0.001). Alborzi et al (2014) study agreed with current study and stated that the AFC increased significantly 3 months after the operation (P<.001).
This study adds to the current knowledge on the deleterious effect of laparoscopic cystectomy on the ovarian reserve and possibly on fertility potential and live birth rate, careful counseling of the patients regarding the risks and benefits and the alternative treatment options is very important in these patients, highly trained surgical team is also very important to avoid removal of healthy ovarian tissue or damage of surrounding ovarian stroma using excessive electrocoagulation.
Availability and data material:
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests:
The authors report there are no competing interests to declare
Funding:
This study received no financial support.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
