
research article | DOI: https://doi.org/10.31579/2637-8914/091
1 Nutrition Department, Al-Sabah Hospital, Ministry of Health, Kuwait.
2 Nutrition Department, Al-Adan Hospital, Ministry of Health, Kuwait.
3 Public Authority of Food and Nutrition, Ministry of Health, Kuwait.
4 Clinical Dietitian, Kuwait Cancer Control Center, Kuwait.
5 Academic Consultant, Greater Richmond Area, Richmond, Virginia, USA.
*Corresponding Author: Farouk El-Sabban, Nutrition and Physiology Consultant, Greater Richmond Area, Richmond, Virginia, USA.
Citation: Fay Al-Dousari, Shahad Al-Otaibi, Dalal Ali, Farhia A. Mohammad, and Farouk El-Sabban. (2022). Status of Nutrition and Health of the Elderly in Kuwait–A Pilot Study. Nutrition and Food Processing. 5(3); DOI:10.31579/2637-8914/091
Copyright: © 2022, Farouk El-Sabban. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 March 2022 | Accepted: 26 March 2022 | Published: 01 May 2022
Keywords: Age; body mass index; chronic diseases; exercise; lifestyle; nutrition
With advances in medicine and medical care, the life span of the elderly population is becoming longer and represents a considerable percentage of society. Therefore, nutrition, lifestyle, and general health of the elderly gained more attention in recent years. However, there have not been published reports on the nutrition and health of the elderly in Kuwait. Thus, this cross-sectional study aims to assess the nutrition and health status of a sample of the elderly in Kuwait. A simple questionnaire was designed and distributed among 149 Kuwaiti and non-Kuwaiti elderly of both genders at various locations. Obtained data were analyzed using the software Statistical Package for the Social Sciences (SPSS- V.19). Findings of this study showed that the range for age of participants was 60-85 years, 96% lived with family and consumed homemade meals, about 70% ate three meals/day, and 70% were overweight (41%) and obese (29%). Diabetes and hypertension were most prevalent among participants, and only 40% followed a dietary program for their health problems. Therefore, the overall nutritional status of the elderly in Kuwait seems adequate. We conclude that interest in the nutrition of the elderly should take individuality into account. In addition, the elderly who are diseased and socially disadvantaged should be given more care, whether from a general health or nutritional perspective. Additionally, we recommend that further large-scale studies ought to be carried out that would reveal various aspects of care for the elderly and help in drawing appropriate strategies in this regard.
The elderly is an umbrella term that involves people who have reached an advanced age, including those in the age category of 55 to above 85 years old. Depending upon the geographical location in the world, reference to the elderly varies accordingly – such as aged and senior citizens. However, it has been generally adopted that the elderly are those humans who are 65 years or older [1]. Therefore, it is customary to report scientific data in 3 categories: the young-old (65-74), the old (75-84) and those 85 and above years as the oldest-old [2].
Advances in medicine and medical care have led to a dramatic increase in life expectancy and the elderly population in society. For example, the projected elderly segment for 2025 in Italy is 25% and 36% in Japan for 2050 [1]. Thus, the elderly population will account for a considerable percentage in societies across the globe. The aging process is a biological reality that is dynamic and mainly beyond human control. However, it is also subject to the constructions by which each society makes sense of old age [3]. The distinguishing marks associated with old age involve both physical and mental aspects that influence the health status of individuals [4]. Generally, there is a reduction in the functions of many organs and systems with aging. Such physical conditions may include bones (osteoarthritis and osteoporosis) and joints, dental problems (loss of teeth), digestive system problems (decreased saliva production, difficulty in swallowing, reduced number and efficiency of taste buds, loss of appetite, and reduced function of digestion and absorption). Most likely, the elderly would suffer from chronic diseases such as hypertension, heart problems, and diabetes. Coupled with bone disease and diminished eyesight, it increases the possibility of falls in the elderly [5]. Additional problems that complicate life for the elderly may include reduced functions of the lungs and the immune system. Chronic pain (rheumatological or malignancy) afflicts older adults as a feature of old age [6]. A variety of problems can involve the skin, vocal cords, and sleeping – among many others. The mental state of the elderly makes them cautious and have antipathy toward risk-taking, may have feelings of incompetence and worthlessness. Because of loneliness and other social and economic factors, the elderly may suffer from depression – which, if severe, may lead to committing suicide. According to the World Health Organization of the United Nations, mental disorders afflict about 15% of people aged 60 and above years old [7]. A survey taken in 15 countries reported that mental disorders of adults interfered with their daily activities more than physical problems [8].
It is realized that the nutrition of the elderly is complex, and the main factors involved are physiological, psychological, pathological, and socioeconomic [1]. Therefore, nutrient requirements for the elderly vary, and the individuality in providing nutritional services ought to be considered. Unfortunately, there have not been any published studies related to the combined nutrition and health of the elderly in Kuwait, thus, this work was carried out. The objective of this pilot study was to assess the nutrition and health status of the Kuwaiti and non-Kuwaiti elderly in Kuwait.
Sample and study tools: This study is a cross-sectional survey of Kuwaiti and non-Kuwaiti elderly. It involved 149 participants of both genders whose age was 60 and above years old. A questionnaire was devised in Arabic and was translated to English – with any discrepancies resolved. The survey questions included aspects of nutrition related to the elderly and their lifestyle. The first section of the questionnaire had personal information. The second section was on the health status of the elderly, the third section was to collect social data, the fourth section involved a 24-hr recall of diet, and the last part was on the medications used by participants. A member or more of the first three authors distributed the questionnaire and answered and clarified any questions from participants. The Arabic version of the questionnaire was used for Arabic-speaking participants and the English version for non-Arabic speakers.
Data analysis
The collected responses of the administered questionnaire were analyzed utilizing a mathematical software Statistical Package for Social Sciences (SPSS- V.19). Student’s t-test and chi-square analysis were used to detect significant differences among parameters of interest. A “P” value of <0>
Demographic data of the study population are shown in Table 1. The sample of the elderly was balanced regarding gender and nationality. Data on the body mass index (BMI) were based on calculations of the weight and height of each participant. The weight of females averaged 75.2+11.4 kg, and their height was 161.2+6.4 cm, and those for males were 77.3+16.7 and 169.0+21.8, respectively. Categorization of BMI showed that 40.9% were overweight and 29.5% were obese – while only 28.9% had normal weight. The overall values for BMI for Kuwaitis and non-Kuwaitis were not significantly different. Only 26.2% of the sample smoked, and the rest were non-smokers. Smoking was not significantly different regarding nationality; however, the difference between genders was significant (P<0>
Item | N | % | |
Gender | Male | 70 | 47.0 |
Female | 79 | 53.0 | |
Nationality | Kuwaiti | 79 | 53.0 |
Other Nationalities | 70 | 47.0 | |
Age | 60-65 | 73 | 49.0 |
66-75 | 51 | 34.2 | |
76-85 | 25 | 16.8 | |
BMI | <18> | 1 | 0.7 |
18.5 – 24.9 | 43 | 28.9 | |
25 – 29.9 | 61 | 40.9 | |
>30 | 44 | 29.5 | |
Do you smoke? | Yes | 39 | 26.2 |
No | 110 | 73.8 | |
Table 1: Demographic, body mass index (BMI), and smoking habit data of the study population (N=149)
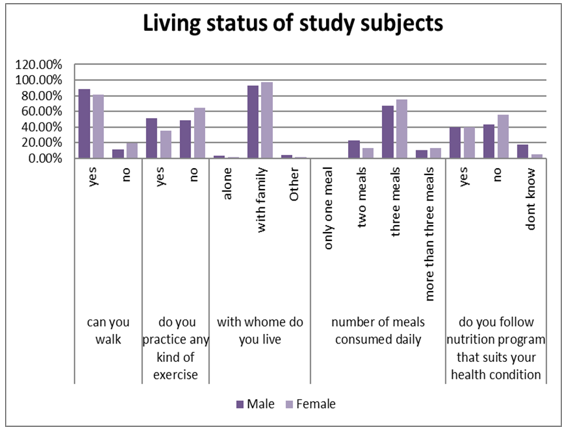
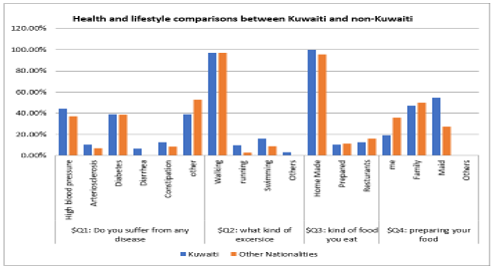
Data on the living status of the study population are presented in Figure 2. Most participants of both genders (96%) lived with their families, 80% were able to walk, and about 40% practiced some exercise. In addition, nearly 70% ate three meals/day, and 40% followed a nutrition program for their health conditions. Data on health and lifestyle of Kuwaiti and non-Kuwaiti study participants are presented in Figure 3. Regarding
health, hypertension, and diabetes figured prominently (about 30% for each). Other heath condition included problems with the digestive system function. Percentages of walking as a form of exercise for Kuwaitis and non-Kuwaitis were equal (about 95%). Almost all of the participants (about 96%) ate home-made food and prepared meals by family members and maids.

This cross-sectional study aimed to assess the overall status in a sample of 149 elderly in Kuwait. We explored the living quality and the health and nutrition status of the study population, such as weight, height, BMI, diagnosed diseases, dietary consumption, and exercise. This sample included Kuwaiti and Non-Kuwaiti elderly from various locations of Kuwait. The proportions of female to male subjects were balanced, as well as with the nationality. The study population in the age group from 60-65 constituted the highest percentage (49%), followed by the age group from 66-75 (34.2%). Reported life expectancy in Kuwait were 73.7 years for males and 76 years for females, with higher mortality rate among males than in females (9). This accounts for the smaller percentage of the elderly in the 75-85 category in this study.
Data on the overall nutritional status showed that 40.9% of the participants were identified as overweight, followed by (29.5%) identified as obese - indicating a high prevalence of overweight and obesity among the older adult population in Kuwait. These results are consistent with a study that reported the prevalence of overweight and obesity among the elderly in Kuwait (10). This study demonstrated a significant difference in mean values of BMI of the male and female participants, 31.2±6.9 for women and 28.1±4.6 for men. Similar results were reported in another study, which showed that overweight and obesity were prevalent among older adults from different geographical regions of Saudi Arabia (11). Both studies indicate that gulf countries have a high incidence of overweight and obesity epidemic among their elderly population. Such a rise in numbers can be due to several factors, including urbanization, increased income, physical inactivity, and unhealthy diet practices (12). Therefore, further studies on the gender difference in obesity parameters among the elderly in Kuwait are suggested. Specially designed programs for healthy nutrition and for physical activity ought to be devised, for better health and well-being of the elderly in these countries.
The percentage of underweight among participants of our study was low (0.7%), which is believed to be more common among hospitalized older patients in Kuwait. A study in Lebanon showed that the malnutrition rate was 12.6% (14 out of 111) among a sample of an elderly (13). This study indicated that underweight participants were malnourished and 48.7% (N=54) were at risk of malnutrition. These findings may indicate that our study participants were adequately nourished and consumed various items from all food groups, lowering the prevalence of multiple forms of malnutrition. In addition, it supports the fact that the older adults in Kuwait and other Arabian Gulf countries live and get proper care in a family setting, whether nutritionally or morally. Almost all of our study’s elderly population (96%) lived with the family, which helped in providing a comfortable living conditions and care towards their health and nutrition status – thus, is considered advantageous when compared to other adults residing in other Middle Eastern countries.
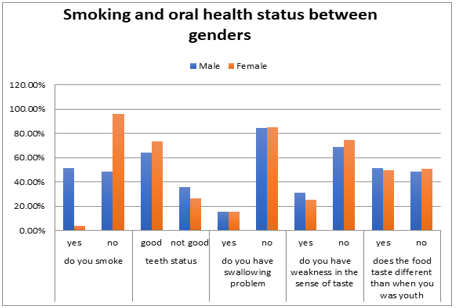
Oral health care is considered essential, especially for the older adult population. Many research studies emphasized the adverse effects of cigarette smoking on the oral health, as it is linked to an increased risk of dental problems, gum disease, mouth cancer, and more. However, most participants in our study had good oral health. They neither smoked cigarettes nor had problems with swallowing, did not experience changes in tasting of food compared to when they were younger. Perhaps, the high proportion of participants who generally had good oral health were more educated, practiced good oral hygiene and habits. It is undeniable that oral health is significant in improving the older people's quality of life, health, and nutrition status. Although, these results differ from a previous study, which indicated that the dental status in the older adult population is alarmingly poor in the 20th century, emphasizing the need for more oral health education programs targeting the elderly in Kuwait (14). However, it seems that knowledge about oral health has improved over the past 15 years, which helped in reducing the incidence of dental and oral diseases and subsequentially improved the oral health of the elderly in Kuwait.
As people age, they are more likely to experience different diseases and health conditions. In this study, diseases common among the Kuwaiti and non-Kuwaiti participants were digestive system conditions, diabetes, and high blood pressure. The finding is relatively consistent with the WHO (Kuwait profile report) about non-communicable diseases (NCD) among the adults in Kuwait. According to the report, the common diseases were cardiovascular diseases, cancer, and diabetes for a population aged between 30 and 70 years (9). This outcome explains why the most used medications were for hypertension and diabetes treatments among the study population. In addition, the prevalence of overweight and obesity could be contributed as a risk factor for the diseases, which the older adults in the study reported.
Good nutrition has been shown to improve the quality of life in older adults. Even though only (40%) of participants followed a nutrition program for their health condition, 70% ate three meals a day. This meal frequency method, eating three meals a day, might lead to most of them not reporting any signs of undernutrition. In addition, 96% of older adults ate homemade food and prepared meals by family members and maids. However, their meals consisted mainly of milk and dairy products (probably full-fat products) for breakfast, whereas meats, starch (probably refined), vegetables for lunch and starches, vegetables, milk, and milk products for dinner. For snacks, the majority favored tea and coffee (probably sweetened) over the other items. Mainly, the distribution of participants was relatively equal for both genders in terms of meals, showcasing that starch is prominently consumed in almost all types of meals. This outcome could explain the high prevalence of overweight, obesity, and nutrition-related diseases, such as diabetes and hypertension, among Kuwait's older adults. Unfortunately, data are insufficient concerning the nutrition and health status of the elderly in Kuwait. Thus, there is ample room for further research areas related to the nutrition of the elderly. The Kuwait Institute for Scientific Research (KISR) issued recommendations that emphasized the importance of action plans for promoting healthy eating among the Kuwaiti population, based on its first comprehensive national nutrition survey (15). Meanwhile, this does not downgrade the need for immediate interventions to reduce the incidence of diet-related diseases. A study done in India that involved a sample of 3871 elderly reported that the nutrition status of this population was poor in terms of quality and quantity (16). In general, the most prominent finding to emerge from this study is that effective nutrition interventions are needed to improve the health and nutrition status of the aging population. In addition, the high prevalence of nutrition-related diseases among the elderly in Kuwait highlights the importance of immediate intervention from stakeholders, such as the Public Authority for Food and Nutrition and the Food and Nutrition Administration before the emergence of serious health and nutritional consequences affecting the older adults in Kuwait.
It is commonly known that nutritional requirements change throughout the stages of life. Assessment of nutritional status is essential for preventing chronic diseases and for well-being. Studying the causes of changing dietary needs and food preferences would be valuable to nutritionists in providing individualized care. Concerning the elderly, nutritional requirements are related to the aging processes and become complicated by other influencing factors. Health promotion for the elderly ought to involve an active lifestyle. According to our findings, the nutrition of the elderly seems to be adequate; unfortunately, most were overweight and obese. The most prevalent chronic diseases among the elderly were hypertension and diabetes. The elderly of this study enjoyed being among their families and consuming home-based meals. Most of
them walked as a form of exercise, a commendable lifestyle aspect. While our research work is of a small scale and the sample involved may not represent the situation for the elderly in Kuwait; however, it sheds light on the importance of paying attention to the care of this segment in society.
This study is the first of its kind in Kuwait and provided general data about the health and nutrition status of the Kuwaiti and non-Kuwaiti elderly. We realize that the used devised questionnaire could have been more comprehensive and included questions regarding the level of education, income, and other living conditions. Also, this study was primarily limited by the data collecting method – as anthropometric information, health conditions, medications taken, and recalling of dietary patterns were self-reported by participants. While deciding on participants was random, the small sample of the elderly included in the study may not be a perfect representation of all elderly in Kuwait. In fact, participants were interviewed at outdoor locations, which could make our sample to be leaning towards the more on the active side persons. Additionally, almost half of the participants were in the “not-too-old” category, which may have accounted for the positive side of our results. We realize that the number of subjects of this study was not considered large; however, such is deemed satisfactory with experienced time constraints. Meanwhile, even with the expressed limitations of this study, it sheds the light on the importance of care and well-being of the elderly population. Accordingly, there needs to be larger-scale studies in the future that explore several perspectives and the many interchanging and influencing factors that involve the health and nutrition status of the elderly in the country.
This work was carried out as a capstone project when the first three authors were senior students in nutrition at the Department of Food Science and Nutrition, College of Life Sciences, Kuwait University, Kuwait. Farhia Ahmad Mohammad organized the components of the manuscript, searched for relevant recent studies, and helped in editing the different drafts of this manuscript. Farouk El-Sabban supervised the capstone project, coordinated all efforts, and edited the final version of this manuscript. All authors approved this manuscript for publication.
All authors declare no conflict of interest in conducting this study or publishing its results.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
