
Case Report | DOI: https://doi.org/10.31579/2693-4787/019
1 Additional Professor, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
2 Senior Resident, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
2 Senior Resident, Department of Pathology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
4 Professor & Head, Department of Pathology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
*Corresponding Author: Satyajeet Rath, Senior Resident, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
Citation: Rahat Hadi, Satyajeet Rath, Azfar Neyaz, Nuzhat Husain (2020) Sebaceous carcinoma of the male breast. J. Clinical Oncology Research and Reports. 2(4); DOI: 10.31579/2693-4787/019
Copyright: © 2020, Satyajeet Rath, This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original
work is properly cited.
Received: 21 September 2020 | Accepted: 07 November 2020 | Published: 15 November 2020
Keywords: sebaceous carcinoma; male breast carcinoma; immunohistochemistry; mastectomy
Sebaceous carcinoma of the male breast is an exceedingly rare occurrence. Literature is inadequate about the prognosis and treatment of such malignancies. We report histo-pathological and immuno-histochemical (IHC) findings in a case of sebaceous carcinoma of breast of a 60-year-old male. An initial biopsy suggested sebaceous carcinoma. Total mastectomy was performed, followed by local radiotherapy and adjuvant chemotherapy. The receptor status was triple negative. Pan cytokeratin and epithelial membrane antigen were positive, whereas S-100 was focally positive and HMB-45 and Melan A were negative. IHC is central to diagnosis and differentiation of these rare kind of tumours from the common invasive ductal carcinomas. The exact line of treatment following excision of the tumour is unclear. Local radiotherapy is generally indicated, whereas the role of adjuvant chemotherapy is uncertain. Wider reporting of such cases will help in widening the horizon of prognosis and management of these tumours.
Sebaceous carcinoma of the breast (SCB) is a rare presentation. Generally, sebaceous carcinomas are reported most commonly in the eyelid. Till date, around 20 cases have been reported in published English literature. Almost all of these cases are reported in females, with one being a male. The case was reported infiltrating ductal carcinoma showing lipid-rich sebaceous like component [1]. We describe a case of male SCB who presented to us after surgery and was treated with chemotherapy and radiotherapy. A thorough review of literature of all the cases, including the histological, immunochemical, clinical, follow up and outcome data is presented.
The patient is a 60-year old male who presented with complaints of progressively increasing fungating growth in the right breast since 9 months. Excision biopsy was done outside. A biopsy done outside was suggestive of poorly differentiated malignant tumour with clear cell changes, possibly sebaceous cell carcinoma. The tumour showed sheets and groups of tumour with marked nuclear pleomorphism, high nucleo-cytoplasmic ratio, hyperchromatism and increased mitotic activity with clear cell changes, lymphocytic infiltrate in the stroma and active areas of necrosis and inflammation. A review of the histopathology slides confirmed the diagnosis of sebaceous cell carcinoma of the breast (SCB). The Immunohistochemistry (IHC) was CK-7, BerEP4 and EMA positive and, Mammoglobin, GCDFP, CEA, ER, PR and Her2neu negative.
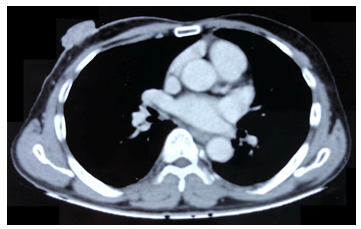
Routine haemogram, kidney and liver function tests and electrolytes were within normal limits. CECT Scan of the thorax was suggestive of right breast soft tissue lesion with heterogenous post contrast enhancement measuring approximately 4 X 3 X 2 cms (Figure 1). Interface of the lesion with underlying chest wall was well-defined. Right axilla showed multiple lymph nodes with mild post contrast enhancement, no necrosis and loss of fatty hilum, with the largest one measuring approximately 11 X 9 mms. Chest X-Ray and CT Abdomen were normal.
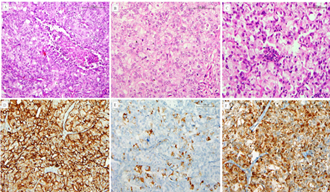
A wide local excision with right axillary dissection was performed. The post op HPE showed the tumour with macroscopic extension into epidermis with skin ulceration. The pT size was 4.5 X 3.3 X 1.4 cm, central and unifocal. The subepithelial zone showed tumour disposed in sheets and nests. The tumour cells were moderately pleomorphic, having vescicular nuclei, distinct nucleoli, moderate amounts of eosinophilic cytoplasm and focal cytoplasmic clearing. Fair number of mitoses were seen. Surrounding stroma showed lymphoplasmocytic infiltrate. All the margins were clear with no lymph node metastasis. All the hormone receptors were negative. Among other markers, Pan CK and EMA were positive. S-100 was focally positive. HMB-45, CEA, GCDFP and Melan A were negative (Figure 2).
SCB is a rare metaplastic breast malignancy. It is characterized by a nested or lobular growth pattern of tumor cells mixed with cells having sebaceous differentiation [2]. It is defined as a breast malignancy with sebaceous differentiation in at least 50% of the cells and not originating from cutaneous adnexal sebaceous glands of the skin of the breast [3, 4]. The term sebaceous carcinoma was first used by Tavassoli, who described it as a distinct subtype of breast carcinoma [4]. Data on the genetic features of these tumours is not available. The histological and IHC features in these cancers conform with those arising in more common anatomic locations like skin and adnexa [6, 7].
A thorough literature review found only 20 described cases of SCB, of which only one case was a male SCB. Three cases were described by von Bogaert et al. [17] and Carlucci et al. [18] each. Svadjler et al. [15] published a case series of 4 cases in 2016. Rest of the cases were reported as as case reports of a single patient [1, 8-14, 16]. The detailed IHC report was available for only 13 cases. The available details of these cases are described in the table below (Table 1). The patients ranged from 45-85 years, except one, who was 25 years old. Eight cases were right sided breast cancers.
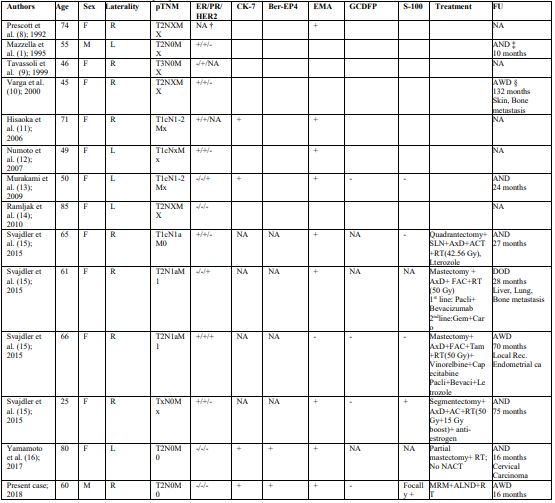
Table 1
†NA – Not available
‡AND – Alive with no disease
§AWD – Alive with disease
¶DOD - Died of disease
The receptor positivity status of the cases is variable ranging from triple positive to triple negative cancers. The complete panel of IHC markers is not available for all cases. 7 patients showed Estrogen receptor positivity, while three cases showed HER2 positivity. The ER and HER2 status was available for 12 and 10 cases, respectively. Eight cases were epithelial membrane antigen positive and three cases showed cytokeratin positivity. Five out of nine patients with known nodal status shoed nodal positivity pointing towards aggressive nodal spread of the disease. Four out of the six cases with known M status had metastatic disease.
There is very little literature on prognosis and behaviour of the malignancy. Hence, the query regarding the best possible management option remains largely unanswered. Like in intraductal carcinomas, most of these cases were also treated with combination of surgery, chemotherapy and radiotherapy. Three of the 5 patients for whom treatment details are available, had mastectomies, while two others had lumpectomies. All these patients had axillary lymph node dissections. Radiotherapy was given ranging from 42.5 – 50 Gy. One of these patients also received boost of 15 Gy. Anti-estrogen therapy was started depending upon the estrogen receptor positivity status. The chemotherapy consisted of anthracyclines plus cyclophosphamides along with a taxane or 5-flurouracil.
The follow-up data was available for 7 of these patients. The survival of the cases ranged from 10-132 months. The differential diagnosis to be considered in this case includes lipid-rich carcinoma, carcinoma with apocrine differentiation, adenoid cystic carcinoma and liposarcoma [5].
In conclusion, we described a case of SCB. The prognosis of these type of cancers is variable. The summary of all the cases reported suggests non-uniformity in management protocols for this particular subtype of mammary carcinoma. More reports on this topic on diagnosis, treatment and prognosis arse needed to further refine the management.
The authors disclose no conflict of interest or no source of funding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
