
Research Article | DOI: https://doi.org/10.31579/2637-8914/223
1Helen Keller International, Nutrition Department, Yaoundé, Cameroon.
2ICT University, Department public health, Yaoundé, Cameroon.
3Family Health International 360, Bafoussam, Cameroon.
*Corresponding Author: André Izacar Gaël Bita, 1Helen Keller International, Nutrition Department, Yaoundé, Cameroon.
Citation: Gaël Bita AI, Agbor N. Agbornkwai, Alex O. Ndjebayi, Jules G. Assiene, (2024), Routine community-based vitamin A supplementation compared to the Mass campaign among 6-59-months old’s children in two health districts, Far North Cameroon, J. Nutrition and Food Processing, 7(10); DOI:10.31579/2637-8914/223
Copyright: © 2024, Fahim A. Shaltout. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 July 2024 | Accepted: 26 July 2024 | Published: 12 August 2024
Keywords: vitamin a; vitamin a supplementation; mass campaign; nutrition; community based; micronutrients
Introduction: Vitamin A supplementation (VAS) is one of the most cost-effective interventions with the greatest impact in reducing child mortality. Mass campaigns are costly, donor-driven, and heavily dependent on funding for mass immunization campaigns. We analyzed routine community-based VAS (rVAS) coverage using the pilot approach of strengthening community participation versus the mass campaign strategy during the “Mother and Child Health and Nutrition Action Week” (MCHNAW).
Methods: This was a descriptive study among from children under five prospectively followed up in a VAS program in Kaele and Guidiguis health districts. We performed a descriptive analysis of data from routine VAS program after capacity building of Community Health Workers (CHW) and compared them with data from the MCHNAW in the period October 2019 and May 2020. Data were collected in the health facilities from the registers to ODK Kobocollect and analyzed by Microsoft Excel 2010.
Results: rVAS showed 95.29% (92.49% Kaele; 98.49% Guidiguis) coverage for children aged 6-11 months (first dose). And 98.29% (97.71% Kaele & 98.77% Guidiguis) coverage for children aged 12-59 months (2nd dose). In comparison, VAS coverage in the mass campaign was lower with 68.46% (61.80% Kaele 72.42% Guidiguis) for 6-11 months and 62.57% (61.27% Kaele & 63.28% Guidiguis) for 12-59 months. These coverages are also lower, compared to the national target coverage (80%). rVAS showed high coverage (>92%) compared to Mass campaign and national target among 6–59-months age children in both health district in the far North Cameroon. However, this study has not analyzed the cost of both strategies of VAS.
Conclusion: Reinforce the routine community-based VAS showed the best coverage to reach children under-five compared to the mass campaign VAS. However, there is need more cost-effectiveness studies to confirm whether strengthening community-based VAS could be a better practice versus mass campaign.
In Cameroon, the infant and child mortality rate remain high at 80 deaths per 1,000 live births. In the Far North region (102 per 1,000) this rate is higher than the national average. This region is also one of the areas (along with the North and Adamaoua) in which the prevalence of micronutrient deficiencies is generally very high, such as vitamin A deficiency, which affects more than 35% of children [1].
Vitamin A supplementation (VAS) is one of the most cost-effective interventions to reduce infant and child mortality [2]. This scientific evidence shows that VAS for children reduces all cause infant mortality by 23% and, if implemented at 6 months of age, could reduce infant mortality by 2.3% (children 6-11 months old). In an environment where exclusive breastfeeding is not widely practiced, with a rate of 40% [1], many children arrive at 6 months with a high risk of vitamin A deficiency.
VAS from 6 months of age should reduce the risk of deficiency and improve survival. In the current model, the point of contact at 6 months (PC6M) to receive vitamin A has not been sufficiently developed and as a result most children do not receive their first dose of vitamin A until 9 months when they come for measles vaccination.
The integration of VAS into polio campaigns has been documented as a good practice in Angola, Chad, Côte d'Ivoire, Tanzania, and Togo [3]. Mass campaigns are costly, donor-driven, and heavily dependent on funding for mass vaccination campaigns. In the far north of Cameroon, the International Humanitarian Organization, Helen Keller International (HKI) has been working with the Ministry of Health (MoH) since 2017 to strengthen community participation in VAS in two health districts of Kaele and Guidiguis. The Community Health Workers (CHW) were recruited from each health area and received training to deliver a package of nutrition activities, including routine VAS in rural areas.
This study compares routine community-based VAS (rVAS) coverage through the pilot approach of strengthening community engagement versus the mass campaign strategy of the Mother and Child Health and Nutrition Action Week, a mass campaign (MCHNAW) among children aged to 6-59 months old in two health districts of Guidiguis and Kaele in Far north Cameroon in year 2020.
2.1. Study design
This was a descriptive study among from children under five prospectively followed up in a VAS program in Kaele and Guidiguis healths districts. We performed a descriptive analysis of data from routine VAS program after capacity building of Community Health Workers (CHW) and compared them with data from the MCHNAW campaign in the period October 2019 and May 2020.
2.2. Sampling
Sampling was exhaustive, all children who were enrolled in the VAS program in the health facilities in the target districts (Kaele and Guidiguis) and, whose data were available and complete in the Vitamin A registers were enrolled in this study.
2.3. Population and study sites
The health districts of Kaele and Guidiguis are locate in the Far North of Cameroon, in the Mayo Kani division, with 29 health areas in 2020. In the same period, the number of children aged 6-11 months living in the two health districts was estimated at 4,314 for Kaele and 7,238 Guidiguis health districts. The target vitamin A coverage was 80% for each district [4]. According to DHIS 2 (2020) data, both health districts had VAS coverage less than 70% for 6-11 months and less than 50% for 12-59 months in the first quarter of 2019. VAS coverage for the health districts were 57.4% (Guidiguis) and 47% (Kaele) for 6-11 months; 21.1% (Guidiguis) and 12.6% (Kaele) for 12-59 months [5].
2.4. Type of interventions
2.4.1. Routine community-based VAS:
This was a pilot VAS project implemented in the health districts of Guidiguis and Kaele in the Far North by Helen Keller International, targeting children aged 6 to 59 months. HKI Intl and MoH trained the Community Health Workers (CHWs) on the importance of Vit A and Essential Nutrition Actions (ENAs). A cohort of children aged 0-59 months was follow-up after a comprehensive census of children in the communities. CHWs conducted home visits (HVs) to sensitize communities, follow up and remind them of appointments, look for dropouts and supplement them with Vitamin A at home if necessary. Vitamin A was only given at home when the child and its mother were unable to reach the health facility. The children who had received the VAS during the mass campaign of December 2020 were excluded in the target. Data were collected by smartphones via the ODK app and analyzed on Excel over the period of October 2019-2020.
2.4.2. The mass Campaign of VAS during MCHNAW:
In December 2020, the MoH with the support of partners, organized the mass campaign of VAS during the MCHNAW, coupled with the National Immunization Days (JNVs). A few days before the start of the VAS, the MoH trained social mobilizers informed and sensitized the population in communities about the campaign. Essential messages were also broadcast in the media and door-to-door. CHWs administered free deworming to children aged 12-59 months, Vitamin A to children aged 6-59 months, and polio vaccine to children aged 0-59 months. The data collected in the tally sheets and summaries were analyzed in Excel by regional team of MoH in Far north.
2.5. Tools and data collection
Data were collected from the VAS registers available in the health facilities of the two districts (Kaele and Guidiguis). Two investigators (one per district) reviewed the data available. Only data for children aged 6-59 months in the study area were extracted from the registers. The data collected from the registers was entered directly into an ODK forms by smartphone and exported to KoboCollect. The data sent to KoboCollect was reviewed, processed, and compiled daily by the study investigators. A questionnaire was also administered to each health facility manager to collect data of the number of health workers and CHWs per gender who had trained to strength the VAS activities in the health area during the year 2020. This data was also entered into ODK and transferred to KoboCollect.
2.6. Data analysis
Only the children who received VAS between October 2019 and May 2020 were include in the routine VAS analysis. The data entered on ODK was exported from KoboCollect in Excel format (xlsx), then edited by an investigator from the research team. The proportions, tables and figures were generated by the pivot table using Microsoft Excel 2010.
2.7. Ethical considerations
This research uses secondary data from the literature review of health facility registers in the two target health districts. The data collected were de-identified to preserve the confidentiality of the people targeted by the study. Only the study investigators and participants in the collection and analysis of the study had access to the database. The smart phones and the Kobo Collect account on which the data was stored had password-protected access, accessible only to the study investigators. The study received health authorization for implementation from the health districts concerned.
3.1. Demographic data
Using the rVAS approach, after excluding children who received vitamin A during the campaign at the end of 2019, the census enrolled 1,058 children in the program, i.e., 49.52% (4,981) girls and 50.48% (5077) boys. The children ranged in age from 6 to 59 months at enrolment, with an average age of 23 months. Children aged 6-9 months and those over 41 months were the most recurrent, with 2,677 and 1,820 children respectively (Figure 1).
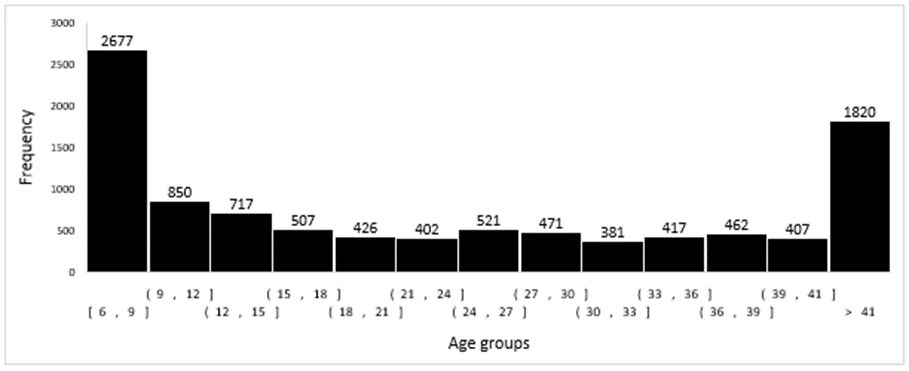
Figure 1: Breakdown of children enrolled in the routine VAS program by age group (n=10058)
3.2. Enrolment phases breakdown
A total of 3694 children were expected to receive the first dose of VAS and 6364 the second dose of VAS. Nearly, 88.8% (3283) of children initially eligible for the first dose became eligible for the second dose during the follow-up in the program. Finally, e, i.e., 9647 children eligible to receive the second dose of vitamin A. By health district, the children expected to receive first dose of VAS were 53.38% (1972) in Kaele and 46.61% (1722) in Guidiguis health districts. Of the total expected to receive a second dose at the end of the program (9647), 45.24% were from the Kaele and 54.75% from Guidiguis health districts.
3.3. VAS coverage by intervention
Routine VAS coverage was 95.29% (92.49% Kaele; 98.49% Guidiguis) for children aged 6-11 months. For children age from 12 to 59 months, coverage was 98.29% (97.71% Kaele & 98.77% Guidiguis). The table 1 showed the breakdown of VAS coverage with rVAS versus mass campaign during the MCHNAW of December 2020.
| Interventions | Target rVAS | Target MCHNAW | rVAS realized | MCHNAW realized | ||||
| Age groups | Kaele | Guidiguis | Kaele | Guidiguis | Kaele | Guidiguis | Kaele | Guidiguis |
| 6-11 months/ | 1972 | 1722 | 4314 | 7238 | 1824 | 1696 | 2666 | 5242 |
| Coverage | 80% | 80% | 80% | 80% | 92.5% | 98.5% | 61.8% | 72.4% |
| 12-59 months/ | 4365 | 5282 | 28874 | 52450 | 4265 | 5217 | 17690 | 33191 |
| Coverage | 80% | 80% | 80% | 80% | 97.7% | 98.8% | 61.3% | 63.3% |
Table 1. rVAS coverage versus mass campaign during the MCHNAW of December 2020
According to the data of the mass campaign (MCHNAW, 2020) of December 2020 in the same districts, 68.46% of coverage (61.80% Kaele 72.42% Guidiguis) was recorded among children age from 6-11 months and, 62.57% (61.27% Kaele & 63.28% Guidiguis) among the 12-59 months age. The national target for supplementation of Vitamin A among under-five in Cameroon is 80% both in routine and mass campaign activities. The coverages of MCHNAW were lower than the expected 80% national target of VAS coverage (figure 1) and routine community-based VAS show the best coverage with >92% children supplemented by Vitamin A in both health district.
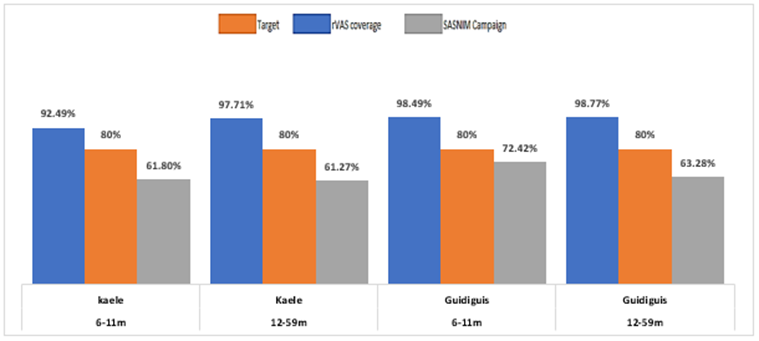
Figure 2. Routine and MCHNAW coverage in 2020 by health Districts targeted.
The integration of vitamin A into polio campaigns has been documented as a good practice in Angola, Chad, Côte d'Ivoire, Tanzania, and Togo [3]. The administration of vitamin A during national immunization days (NIDs) helps to raise awareness, improve technical capacity, and improve evaluation. Polio NIDs provide an entry point for sustainable provision of vitamin A supplementation with routine immunization services [5]. As polio programs advance and campaigns decline, there is a risk that fewer children will be reached with VAS each year [3].
Mass campaigns are expensive, donor-driven, and heavily dependent on funding for mass immunization campaigns. They require extensive macro-level planning at the national and international levels for the timely ordering, shipping, and distribution of commodities and micro-planning at all levels of the health system. Campaigns do not encourage health-seeking behaviors among vulnerable communities and do not build the capacity and resilience of routine services to meet demand [6]. According to Ousmane Ouédraogo et al, (2022), the routine community-based vitamin A supplementation strategy showed good acceptability of the strategy by all stakeholders in Burkina Faso [7]. According to the authors, 2 years of implementation of community-based VAS, the national coverage of VAS was maintained at a high level (above 90 % and there was a reduction in operational costs.
Gaël Bita AI et al, (2023) showed that, the capacity building of HWs and CHWs to involve in VAS programs can used many contact points for VAS as: health facilities; advanced strategies in the communities and home visits. According to the authors, involve the CHWs and Heath workers by capacity building is a form of community engagement who could help catch up children with difficulties to access the health facilities services for VAS [8].
The main challenges for the community-based VAS included delayed Community-Based Health Workers remuneration and weak communication and supervision [9], the financial costs associated with CHW incentives should therefore be considered when reinforcing the VAS with community members.
Strengthening community participation in VAS may be the best practice versus mass campaigns for good VAS coverage in health districts. However, this study has not analyzed the cost of both strategies of VAS. We recommend a cost-effectiveness study of the implementation of routine VAS through strengthening routine community-based VAS.
The authors thank Helen Keller International Cameroon; the Ministry of Public Health of Cameroon; and the health workers of Kaele and Guidiguis health districts.
The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
