
Case Report | DOI: https://doi.org/10.31579/2693-4787/004
1 University Hospital Leiden, the Netherlands.
*Corresponding Author: George Zhu, University Hospital Leiden, the Netherlands.
Citation: George Zhu, Retrospective Survey on the Outcome of 36 Diverse Cases of Anemia. J.Clin Onco Res and Rep. 1(1). Doi: 10.31579/2693-4787/004
Copyright: © 2020 George Zhu, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 March 2020 | Accepted: 22 May 2020 | Published: 24 July 2020
Keywords: anemia; iron; vitamin B12; folate; drug induced immune hemolytic anemia (DIIHA); prevention and treatment
Anemia is clinical common event. In this study,a retrospective study of 36 different types of anemias was place in proper interpretative review for their therapeutical outcome. By using comprehensive treatment regimen according to patients’ condition, 23 patients obtained cure or complete remission (CR), with the exception of refractory cancers and uremic anemia. Iron supplement was provided in 5 iron deficiency anemia. One megaloblastic anemia required the prescription of the supplement of vitamin B12 or folate deficiency. 2 aplastic anemia obtained complete remission with the integrated protocol of methyltestosterone,adenine,leucogen,and levamisol. Steroid hormone (e.g. prednisone) mixed traditional medicine were occasionally promising benefit in a nephrotic syndrome and renal insufficiency. Among 2 cases with dug- induced immune hemolytic anemia (DIIHA), laboratory studies a patient's serum contained paracetamol -dependent antibody that in the presence of paracetamol, agglutinated in vitro with "O" red cells with or without complement. Drug antibody titer was 1:4 positive. The reactive mechanism was attributed to both immune complex type and drug-adsorption, whereas another herba origanum vulgare- induced hemolysis secondary to drug adsorption only. In addition, regarding anemia caused by malignant tumours, the molecular genetic regulation of retinoic acid in acute promyelocytic leukemia (APL) has been further illustrated(see figure in full text). Therefore,to strengthen the active prevention and/or early interceptive treatment of anemia is our care.
Anemia is the common blood condition in clinical. Anemia define the condition in which there is a reduced number of circulating erythrocytes and a smaller than normal hematocrit or a reduced concentration of hemoglobin in peripheral blood. Many hormones,in addition to erythropoietin,participate in the regulation of erythropoiesis. Hormones that affect enzyme and protein synthesis also affect synthesis of hemoglobin and production of red cells. The characteristic anemia of hypothyroidism is normochromic-normocytic,mild to moderate anemia.
There are many types of anemia. Condition associated with the causes of anemia include: bone marrow and stem cell problems(e.g. aplastic anemia,thalassemia),iron-deficiency anemia(IDA),Vitamin deficiency anemia specifically vitamin B12 or folate. Anemia also linked to other chronic diseases,such as advanced kidney failure or cancer. One of the most remarkable reports is in the field of drug antibody-induced immune hemolytic anemia. This paper will attempt to place in a retrospective survey of 36 anemias outcome in my group.
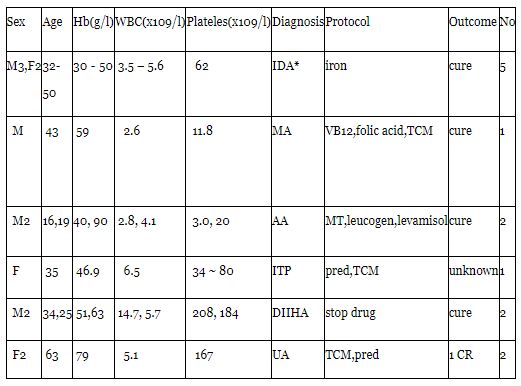
36 animas were included in the study during 1989-2019. All patients were in progressive when they were hospitalization. The sex ratio of male:female was 23:13 respectively. Among age distribution, it was ranging from 4 to 75 years. The clinical diagnosis in a broad variety of anemias included: Iron deficiency anemia(IDA) 1 case,gastric ulcer hemorrhage complicated with iron deficiency anemia 4 cases; megaloblastic anemia(MA) 1;aplastic anemia(AA) 2;Idiopathic thrombocytopenic purpura(ITP) complicated with severe anemia 1;Malarial anemia 1; Drug-induced immune hemolytic anemia (DIIHA) 2 [ 1 case following paracetamol-induced,another case following herbs Origanum vulgare(wild mint) -induced]; uremic anemia(UA) 2; 22 anemias caused by various tumors: hematologic malignancies(ALL 1,AML 3,APL 1, CML 2, CML with blast crisis 1, CLL 1,multiple myeloma 1);metastatic lymph node adenocarcinoma 1;myelodysplasia(MDS) 2; nasophyaryngeal carcinoma 2;gastric cancer 4;colon cancer 1;bladder cancer 1;and advanced liver cirrhosis complicated with gastric hemorrhage 1 case. The treatment regimen varied among different types of anemias. The criteria of complete remission(CR) and/or partial remission(PR) in cancers is according to the rules where physicians have in common with in clinics. Complete remission(CR): there was no tumor or tumor complete regressed in patients for at least 1 month; Partial remission(PR):the tumor decreased by more than 50% in patients for at least 1 month. Disease progression: the tumor increased by more than 25% in patients,or new lesions emerged. The efficacy was evaluated according to the survival time from the day when patients were at onset. The clinical data for 2 cases of DIIHA were previously described.
Anemia treatment will depend on the different types of anemias. The remaining patients achieved 9 cases with complete remission or 14 cured through different regimen of integrated western and traditional medicine, with the exception of refractory cancers, uremic anemia and one patient with ITP and liver cirrhosis complicated with hemorrhage transferred to another hosiptal.
During the schedule of drug administration(see table 1), many preparation of oral iron are available in 5 patients with iron deficiency anemia(IDA) or IDA following gastric ulcer hemorrhage. A significant increase in hemoglobin can be gained by observing the response to iron therapy. One patient with megaloblastic anemia often required the supplement of vitamin B12 and folic acid,which produced an excellent response. Steroid hormones(e.g. prednisone) and especially traditional medicine produced complete remission in one nephrotic syndrome and renal insufficiency.
As to the patients' anemias caused by malignant tumors, a short CR was achieved by the use of combination regimen of FAM or FMC(5-Fu, Ara-C, mitomycin C or CTX),and cantharidin in 3 advanced gastric cancers. On of them was a long-term survivor for 6 years. In view of the types of hematological anemias,partial remission was conducted by DA regimen (daunorubicin 40mg/m2 x3 days,Ara-C 200mg/m2 x 4 days) in 1 case with M1 type in another hospital and HA combination chemotherapy (homoharringtonine 4mg/m2 x3 days,Ara-C 50mg intramuscular injection, twice daily for 5 days) in a case with M2 type acute myeloid leukemia. An acute promyelocytic leukemia(APL) obtained CR via retinoic acid in conjunction with a 5 days of 1mg homoharringtonine intravenously and traditional medicine one month duration. He was a 20 months of survivor. A 62-year-old woman with chronic myelocytic leukemia achieved CR after busulfan and antiotics regimen. She was a survivor for near 8 years. A 62-year-old female multiple myeloma with anemia obtained CR after low-dose thalidomide and prednisone,and plant medicine vinca rosea(catharanthus roseus) . During the follow up of 3½years,she remained CR. The malignant anemias were summarized in table 2.
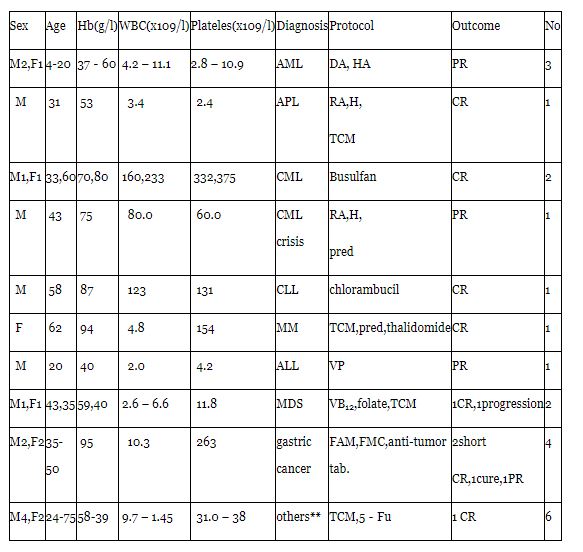
Note:others included:metastatic lymph node adenocarcinoma 1 case,Hb 58g/l; nasopharyngeal carcinoma 2; colon cancer 1; bladder cancer 1; and advanced liver cirhosis with gastric hemorrhage 1 case,Hb 39g/l,hemocrit(HCT) 13.8%,RBC 2.02x 1012/l, patient transferred into another hospital. M:male, F:female. ALL:acute lymphocytic leukemia; AML:acute myeloid leukemia; APL:acute promyelocytic leukemia; CML:chronic myeloid leukemia; CML crisis:CML with blast crisis; CLL: chronic lymphocytic leukemia; MM:multiple myeloma. TCM:traditional medicine. Pred:prednisone. VP:vincristine,prednisone.
Drug-induced immune hemolytic anemia(DIIHA) is a rare cytopenia. DIIHA is considered in 2 patients. A 25-year-old patient with paracetamol- dependent antibodies reactive by immune complex type and drug adsorption mechanisms. The direct antiglobulin test was 1:4 titer positive with polyspecific antiglobulin reagent. The patient's serum contained an antibody that, in the presence of paracetamol, results in agglutination of papain-treated "O" type of RBCs with complement. The serum also agglutinated paracetamol-coated RBC cells at 37℃(drug-adsorption). Another herbs origanum vulgare(wild mint)- treated antibody determination, the patient's serum results in agglutinatination and hemolysis of drug- treated "O" RBCs(RBCs coated with herba wild mint ) with coombs antiserum IgG at 37℃, indicating a drug adsorption mechanism. Drug antibody titer was 1:4 positive. When washing drug-coated RBCs with saline solution repeatedly, it was found to still appear a coombs test postive. Once DIIHA is considered,management included the appropriate serologic determination, immediate discontinuation of the implicated drugs and corticosteroids to ameliorate DIIHA symptoms and reduced the drug antibody.
Case 1. On November 11,1985, a 25-year-old man was admitted to hospital due to his anemia and persistent jaundice. After careful inquiry,in March 1985 and July 1985 respectively,he had a history of 4 (total 8 capsules) Ka Huang Min capsules (paracetamol, caffein, artificial cow- bezoar and chlorphenamine maleate capsules). In 1984,he once had a past history of taking 6 capsules Ka Huang Min drug. And one month later,he developed immune hemolytic anemia. At physical examination showed chronic anemia,mild icteric sclera. T 37.3℃, P 92/min, BP 100/70mmHg. There was no bleeding and lymphadenopathy. A grade II systolic murmur was audible at the apex. The lower border of his liver was paplpable 1.5cm below the right costal margin, and the spleen edge could be felt 3cm below the left costal margin. Laboratory data: Hb 63g/l, WBC 5.7 x109/l, leukocyte differential count: segmented neutrophils 48%, lymphocytes 42%, monocytes 6%, eosinophils 4%. Platelets 184 x109/l. Reticulocyte count was 10.%. Urine analysis:protein trace, urobilinogen (+), urine bilirubin (–). Icteric index(II) was 18 units. Serum AST was normal. The serum total bilirubin was 29.07umol/l. The serum haptoglobin level was 505mg/l. The serum albumin(ALB) 44.8g/l,globulin 30.8g/l. HbA2 was 5.1~5.57%,HbF 8.23~9.05%. Hemoglobin electrophoresis showed normal electrophoretic pattern. Ham test,sucrose hemolysis test, methemoglobin reduction test,and isopropanol test were all negative. Direct antiglobulin test(DAT)(Coombs) was 1:4 positive. Cold agglutinin test was 1:16. Bone marrow was hypercellularity, M:E=0.7:1, 51.6% erythroid, orthochromic normoblasts occupied the predominant cells of erythroid, and many anisocytosis abd poikilocytosis. Erythrocyte osmotic fragility test(ROFT): at initial hemolysis: patient 0.40%,control 0.48%; at complete hemolysis: patient 0.24%,control 0.28%. The results of decreased ROFT and increased HbA2、HbF level indicated the diagnosis of mild β thalassemia trait.
To confirm paracetamol-induced DIIHA,the solution of Ka Huang Min capsules containing all four ingredients were performed using serological tests(table 3). In the presence of Ka Huang Min solution,the patient serum contained an antibody that agglutinated with untreated "O" red cells with or without complement. The serum was also reactive with paracetamol -coated "O" red cells at 37℃. The results implicated that paracetamol -dependent hemolysis via both immune complex and drug adsorption. If there was autoantibodies (DAT titer 1:4), which remained testable. In December,1985, Hb reached to 92g/l, and reticulocyte count was declined to 2.6%.
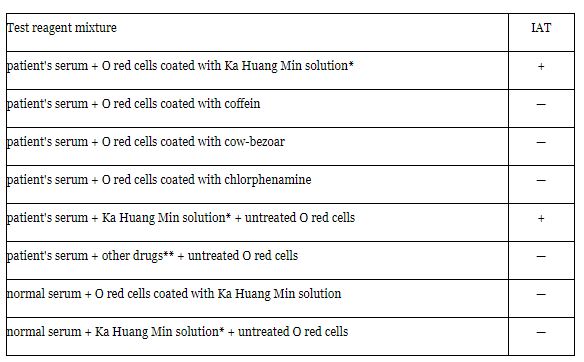
Note: *Ka Huang Min solution containing four ingredients of paracetamol, caffein, artificial cow-bezoar,and chlorphenemine. **Antibody tests including only caffein, cow- bezoar or chlorphenamine respectively.
Case 2. On September 4,1985,a 34-year-old man was admitted to hospital due to his headache,pallor and hemoglobinuria for 4 days. On August 28,1985,the patient felt sore and ache all over,and specially a pain in his right thigh. He had taken a daily dose of 3000ml traditional decoction. Traditional medicine included kudzuvine root(radix puerariae),serissa japonica(serissa serissoides),and origanum vulgare(wild mint). After 4 days,an episode of 4 days of significant hemoglobinuria(soy urine) was noted. On September 2,1985,he developed icteric skin and sclera,and his temperature reached to 38℃. His initial hemoglobin level was 50g/l. He was the suspect of "hepatitis" in a local country hospital,and subsequently as anemia cause,transferred to our hospital. He had no past history of tuberculosis. Upon physical evaluation: T 38.2℃,P 96/min,R 32/min,BP 120/60mmHg. Icteric skin,sclera and mucous membranes. There was no abnormal in his hear and lung. The liver edge could be palpable 1.5cm below the right costal margin and no spleenomegaly. Laboratory evaluation: Hb 51g/l,WBC 14.7 x109/l,leukocyte differential count:segmented neutrophils 81%,lymphocytes 16%,monocytes 2%,eosinophils 1%. Platelets 208 x 109/l. Urine samples were negative for proteins. Serum BUN 9.7mg/dl . The serum albumin(ALB) 3.56g/dl,and globulin(GLB) 3.21g/dl. Serum immunoglobulin(Ig) detection: IgG 1185.3mg%,IgA 264.9mg%,IgM 197.5mg%. Serum HBsAg was negative. AST and ALT were normal results. van den Bergh was indirect positive. Rous test,Ham test(the acid-serum lysis test),heat lysis test,sucrose hemolysis test,Isopropanol test,and cold agglutinin test were all negative. Direct antiglobulin test(DAT)(Coombs') was negative. Bone marrow was cellularity. Bone marrow differential count: 48% myeloid, 42.6% erythroid,approximately 31.0% of predominant cells was orthochromic normoblasts,and many anisocytosis and poikilocytosis. Electrophoresis of serum and hemoglobin electrophoresis were normal results.
To confirm the drug-induced immune hemolytic anemia(DIIHA),the drug-related serologic tests performed according to standard methods(table 4). The titer of drug antibody was 1:4. The experimental results indicated the diagnosis of herbs wild mint induced DIIHA,which was mediated by drug-adsorption mechanisms. After discontinuation of offending herbs,on September 5,1985,Hb was 75g/l,reticulocytosis 24.6%(control:0.5-1.5%); On September 9,1985,Hb reached to 87g/l,WBC 6.5 x 109/l,platelets 109 x109/l, reticulocytosis 28.1%; At discharging from hospital,on September 18,1985,Hb was 95g/l,reticulocyte count was 5.6%. After the follow up,the patient reached essentially near normal hematologic levels.
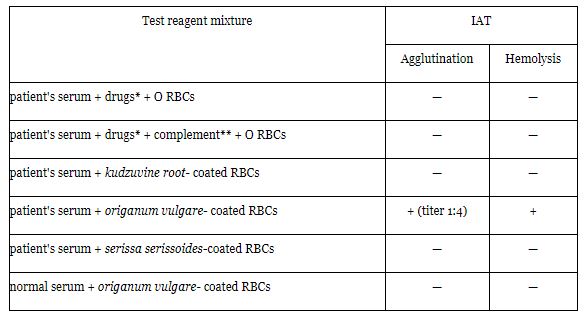
Note: *Antibody tests with three kinds of herbs(see above) respectively. Experimental methods according to Prof. Garratty's and Prof. Lin's further modification. **normal guinea pig serum as a complement source. IAT: indirect antiglobulin test
Case 3. On February 4,1990, a 16-year-old boy was the chief complaint of a sudden drops of blood from nostril,and intermittent up to about 5 hours. On February 15,1990,an episode of repeat epistasis occurred for 2 hours duration. The prescribed drugs vitamin C and ubiquinone(CoQ) revealed ineffective to his hemostasis. Since the winter of 1989, the patient presented the symptoms of fatigue and progressive weakness. On February 24,1990,the patient was adviced to be further examination in a local country hospital. Hemogram: Hb 40-53g/l, WBC 2.8-4.0 x 109/l,leukocyte differentiate count: 26-33% segmented neutrophils, 67-74% lymphocytes. Platelets count was 30 x109/l. Bone marrow was the definite diagnosis of aplastic anemia on March 6,1990. There was no useful following various combination regimen of conventional western and traditional medicine. At that time,the patient occasionally passed out,and he catched a persistent fever over 39℃. After grinding and drink with rhinoceros horn solution daily,the processed plan was considered the combination of methyltestosterone(30mg/day),leucogen,vitamin B4(adenine) and Batil,and levamisole. Remission was obtained following 4 months treatment duration. An induction of breast tumours was unexpectively uncovered by the use of 6+ months of methyltestosterone treatment,and tumour was progressive regressed after stopping this drug for four months. The patient had a health child. He is a well survivor now.
Case 4. On August 21,1996, a 34-year-old woman was admitted to the hospital due to her nephrotic syndrome and renal insufficiency for 3 years. On admission,she was chief complaint of severe pallor,fatigue,and facial edema. At physical examination,she had a percussion of bilateral flank pain. Ascites +++. BP 120/80 mmHg. Urine analysis: protein 4+; sediment: 1-2 RBC/HP and 4-6 WBC/HP. Blood chemistry showed BUN 7.7 mmol/l(control:2.9-7.1 mmol/l). She was given penicillin G sodium and dexamethasone intravenously,with traditional medicine and adjuvant intramuscular testosterone. The drugs vitamin C and Ferrous sulfate tablets were also given orally. On August 29,1996,proteinuria was declined to 1+. The traditional medicine and testosterone were continued to be taken later. On September 8 and October 24,1996 respectively, repeat urinalysis showed protein negative.Traditional medicine consisted of Codonopsis pilosula, astragalus membranaceus(30-60g), radices rehmanniae, angelica sinensis, ophiopogon japonicus, daizheshi(processed Haematite), lycium barbarum(wolfberry), poria cocos, polyporus umbellata, rhizoma anemarrhenae, orange peel. She died of severe renal failure,and she was a 8 years survivor.
Case 5. On June 27,1997, a 75-year-old woman was the chief presentation of her anemia following melena,fatigue and progressive weakness one year ago. After careful inquiry,the patient suffered from metastatic nasopharynx cancer. She had a past history of stomach bleeding,which considered its metastatic origin. On admission,a thumb lymph node behind her right ear was palpable. CR was obtained through a main regimen of traditional medicine and small dosage of chemotherapy(cyclophosphamide and 5-Fu),and enlarged metastatic lymph node was progressive regression. The detail processed method mixed cyclophosphamide or 5-Fu solution into the decoction of traditional medicine, oral use, twice daily. Traditional medicine consisted of Prunella vulgaris, astragalus membranaceus, rehmannnia glutinosa, ophiopogon japonicus, lycium chinensis(wolfberry), red date, spatholobi caulis, scutellaria barbata d. don, oldenlandin diffusa roxb. She was a 4-years survivor.
Case 6. On December 26,1997,a 35-year-old woman was admitted to the hospital because of her relapsed gastric cancer,with anemia and recurrent fever for one month duration. On admission, her temperature was 36.9℃(in the morning) and 40.5℃(at night),and blood pressure 100/70mmHg. Hemogram: Hb 95g/l, WBC 10.3 x109/l, platelets 263 x109/l. In March,1996 she was undergoing surgery in a local country hospital due to her tarry stools. At post-operatively,a rodent ulcer(5 x4 x0.8cm) with harden margin was detected in lesser curvature of the stomach, accompanied with adjacent metastatic lymph nodes. NHL was diagnosed according to her stomach tissue specimens. She had a past history of tuberculosis. CR was obtained after small dosage of FMC(5-Fu,MMC,CYT) in conjunction with cinobufacini intravenously,oral daily demethylcantharidin and traditional medicine. As an outpatient,she had continued to traditional herbs Scutellaria barbata d. don. On June 4,1998, she was consulted as an outpatient due to her fever reached to 38℃. After an injection of penicillin G and small doses of 5mg of dexamethasone,fever regressed to normal(T 36.2℃). On March 5,2000,she had a fever 39℃,and she was at the third hospitalization. Chest X-ray disclosed her dual lung tuberculosis with bullous formation. Her OT test: positive(+). Gastroscope at that time showed a normal image. Her high fever declined to 36.2-36.8℃ by the combined use of ampicillin,intramuscular streptomycin 0.75g, bupleuri injection and additional herba houttuyniae(cordata) injection. On June 6,2002,the patient was at fourth hospitalization due to an episode of her temperature ranging from 37.8℃ to 38℃. Treatment consisted of ampicillin 1g intramuscularly, bupleuri injection,with adjuvant subcutaneous BCG injection. The fever fell ranging from 36.2℃(morning) to 37.4℃(night). She was a long-term survivor for 6 years and died of severe tuberculosis(type IV).
Case 7. On April 14,1999, a 50-year-old woman was admitted to hospital due to her chronic anemia and recurrent abdominal pain for more than half a year. In september,1998,the patient presented a unexplained dull pain in the epigastrium,accompanied with acid regurgitation and belching. No nausea and vomiting were noted. Physical examination revealed anemia. The was no obvious tenderness around the umbilicus. A 10x 8cm2 harden mass was palpable in the abdomen,with a unsmooth surface and an indistinct surrounding. Gastroscope showed an advanced gastric adenocarcinoma,complicated with hepatic metastasis. Treatment consisted of the combination regimen of daily 250mg 5-Fu and 1-3mg/day of homoharringtonine for 10 days, in conjunction with intravenous cinobufacine and oral demethylcantharidin. Afterwards, a combination chemotherapy was intermittent to be given according to patient condition. On May 18,1999,she obtained a short CR. She was continued to the prescription of traditional medicine,or 5-Fu solution mixed the decoction of traditional medicine.
Case 8. On May 3,2000, a 19-year-old man was admitted to hospital because of dizziness and progressive fatigue for more than half a year,and a recent episode of epistaxis for 10 days. Physical data on admission disclosed anemia. The temperature was 38.5℃. Ear,throat and occular examination were normal. There were no obvious abnormality as to heart and both lungs. His heart rate was 105 beats per minute. There was no lymphadenopathy,hepatomegaly,or splenomegaly. He had a past history of hepatitis B. Laboratory data: on admission,blood findings were Hb 90g/l, decreased WBC, platelets 20 x109/l. Bone marrow showed a marked hypoplasia. Bone marrow differential count: 29.6% myeloid, of which band and segmented neutrophils accounting for 27.7%, 5.5% orthochromatic normoblasts, 38.8% lymphocytes,and 7.4% plasmacytes. An almost complete marrow depression was apparent. The diagnosis of aplastic anemia was made. Treatments consisted of a combination regimen of methyltestosterone, stanozol, levamisole and prednisone tablets,and adjuvant with traditional medicine. An additional use concluded intravenous phytohaemagglutinin for 1 week in order to accelerating the number recovery of CFU-S and initiating DNA synthesis of cells. After a 4 months of oral methyltestosterone, he was forced to discontinuing this drug due to his breat swelling and pain and suspected breast tumour. The patient was once receiving subcutaneous erythropoietin. On October 26,2000, complete remission in peripheral blood was obtained following the combination treatment for near 6 months. Becuse of without undergoing continuous treatment, on April 2002, the patient was transferred to another hematological hospital following the recurrence of aplastic anemia. After the follow up of 18 years, he is a survivor now.
Case 9. On october 16,2003, a 31-year-old man was the chief of his pallor and fever for 15 days. On admission,physical examination showed a marked anemia and hepatomegaly. Persistent fever reached to 39℃. Chest X-ray showed small amount of hydrothorax. Liver CT scan demonstrated a 7.0 x 4.5 cm2 mass which was considered as secondary hepatic tumor. AFP was negative. Laboratory data: hemoglobin concentration(Hb) was 53g/l, white blood cells(WBC) count was 3.4 x109/l,leukocyte differential count in blood smear:20% promyelocytes. The platelet count was 2.4 x109/l. Bone marrow aspiration revealed normal cellularity. Bone marrow differential count showed 77% promyelocytes. The patient was diagnosed as acute promyelocyte leukemia(APL) complicated with secondary hepatoma. Treatment consisted of 80mg/day of retinoic acid(RA) and 1mg/day of homoharringtonine(H) intraveously for 5 days. His high fever was declined to normal following small dose of dexamethasone and traditional medicine. On November 20,2003, repeated bone marrow smear showed only 3.5% myeloid blast and promyelocytes. On the routine peripheral blood smear uncovered no immature myeloid cells. Hemogram:Hb 102-108g/l, WBC 7.7-5.0 x109/l, platelets 229 x109/l. CR was obtained after 1 month period of RA,chemotherapy and traditional medicine. On June 5,2005,he died of APL relapse(94% blasts and promyelocytes in peripheral blood and in bone marrow). The repeated liver scan found the complete regression of his liver tumor albeit the recurrence of his leukemia.
Case 10. On January 16,2011, a 58-year-old man was diagnosed as having chronic lymphocytic leukemia(CLL) due to his anemia and leukocytosis to 118 x109/l. The patient was once treated with hydroxycarbamide in another hospital,and leukocytosis was declined from 67-97 x109/l to 27 x109/l. On admission,the most common physical signs revealed two thumb lymph nodes in his left neck region. Hemogram: Hemoglobin concentration(Hb) was 87g/l, WBC 123.88 x109/l. leukocyte differential count: 9% segmented neutrophils,90% small lymphocytes. Platelet count was 131 x109/l. Bone marrow aspiration revealed hypercellularity. Bone marrow differential count:14% myeloid,7.2% erythroid,76.8% small lymphocytes. The diagnosis of CLL was made. CR was obtained through the use of chlorambucil tablets and traditional medicine. On May 5 and July 28,2011, Hb 104-112g/l, WBC 9.54-10.1 x109/l,with a leukocyte differential count of 26.2% mature neutrophils and 63.8% lymphocytes. The platelets 101-112 x109/l. Bone marrow aspirates on May 14,2011 showed normal cellularity. Bone marrow differential count: 34% myeloid,31.2% erythroid,and 33.6% lymphocytes. As an outpatient, he continued traditional medicine. He was well until on October 15,2011 while an attack of stomach pain and tarry stools was admitted to another hospital. At that time,hemogram: Hb 69g/l, WBC 7.3 x109/l, platelets 188 x109/l. Repeat bone marrow aspirates on October 15,2011 revealed normal cellularity. Bone marrow differential counts: 50% myeloid,21% erythroid, and 27.5% lymphocytes. The patient died of another stomach cancer.
Case 11. On April 9,2006, a 43-year-old man was admitted to the hospital because of dizziness、fatigue and progressive weakness for more than half a year. At a routine physical examination,there was revealed a marked anemia. Hemogram: Hb 59g/l(control:131-172g/l), RBC 1.90 x1012/l (control: 4.0-5.5 x1012/l), WBC 2.6 x109/l, platelet count 11.8 x109/l. Urinalysis showed bilirubinuria. Bone marrow aspirates revealed normal cellularity. Bone marrow differential count: 48.4% myeloid,30.4% erythroid,2.4
In this study,a series of the long follow up of 30 different types of anemias were reported. Uptil now, about 130 drugs in DIIHA has been incriminated. Regarding drug-dependent antibody formation,the most accepted idea involves covalent binding of the drug to erythrocyte membrane, creating a neoantigen composed of membrane and drug. An antibody(usually IgG) can be created against the drug,which then binds to the drug-coated erythrocytes and is subsequently activate complement,and cause acute hemolysis. Drug-dependent antibody formation is most commonly caused by penicillin,peracillin, along with cefotetan and ceftriaxone(1-6). We reported 2 patients with penicillin- induced DIIHA previously (Lin zhusan, Zhu yuejun, Zhang guangsheng, etal, 1984, data not shown). One 16-year-old boy was identified his penicillin antibody - dependent hemolysis, which was mediated by immune complex type and drug adsorption, and autoantibody multiple mechanisms. In immune complex type detection, the drug antibody titer reached to 1:512. Another 40-year-old woman with DIIHA was mediated by the drug-adsorption only. The penicillin antibody titer: 1:16. Two additional paracetamol -dependent and herbs wild mint- induced DIIHA were presented here.
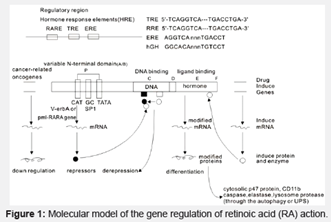
As a novel retinoic acid(RA) to APL treatment,this specific APL harboring oncogenic pml/RARa fusion. This oncogenic receptor derivative pml/RARa fusion act as a constitutive repressor of RAR and retinoic acid signaling, inducing differentiation blockade at promyelocytic stage, whereas pharmacologic retinoic acid(ATRA or cis RA) can bind to oncogenic pml/RARa, then relieve the blockage of pml/RARA repression(also derepression), and subsequently oncogenic pml/RARa degradation via autophagy or UPS proteosome system, immature promyelocytes toward maturation. Finally,APL patients obtained complete remission(CR)(see the following figure)(9-18) Therefore,we cannot say that the drug retinoic acids stimulate(bind to) a pml/RARa oncogene. This model is first described in eukaryotes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
