
Research Article | DOI: https://doi.org/10.31579/CCOR-2021/002
Department of Medical Oncology, The Christie NHS Foundation Trust, M20 4BX Manchester, United Kingdom
*Corresponding Author: Angela Lamarca, Department of Medical Oncology, The Christie NHS Foundation Trust, M20 4BX Manchester, United Kingdom
Citation: Frizziero ., Purohit A. , Malik A. , Deshpande R. , Mairéad G. McNamara, Thomas Satyadas, Jamdar S., Pihlak R., Sheen A., Siriwardena A., Richard A. Hubner, Derek O’Reilly, Juan W. Valle, Nicola D L.i Carino, Lamarca A. (2021) Resected Pancreatic Ductal Adenocarcinoma: understanding tumour tropism to maximise benefit from surgery. Clinical Cancer and Oncology Research 1(1) DOI:10.31579/CCOR-2021/002
Copyright: © 2021, Angela Lamarca, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 May 2021 | Accepted: 05 June 2021 | Published: 23 June 2021
Keywords: pancreatic ductal adenocarcinoma; relapse patterns; risk factors for relapse; mri liver
Introduction: Relapse-rate in pancreatic ductal adenocarcinoma (PDAC) remains high. Identification of modifiable factors associated with relapse could improve patient selection for surgery.
Methods: All consecutive patients diagnosed with PDAC undergoing curative surgery between Jan’05 and Sep’17 were retrospectively analysed. Recurrence-Free Survival (RFS)/Overall Survival (OS) were estimated with Kaplan-Meier method and survival analysis performed with univariate/multivariable Cox-regression (Cox). Logistic-regression (LR) was used for identification of risk factors of tumour recurrence.
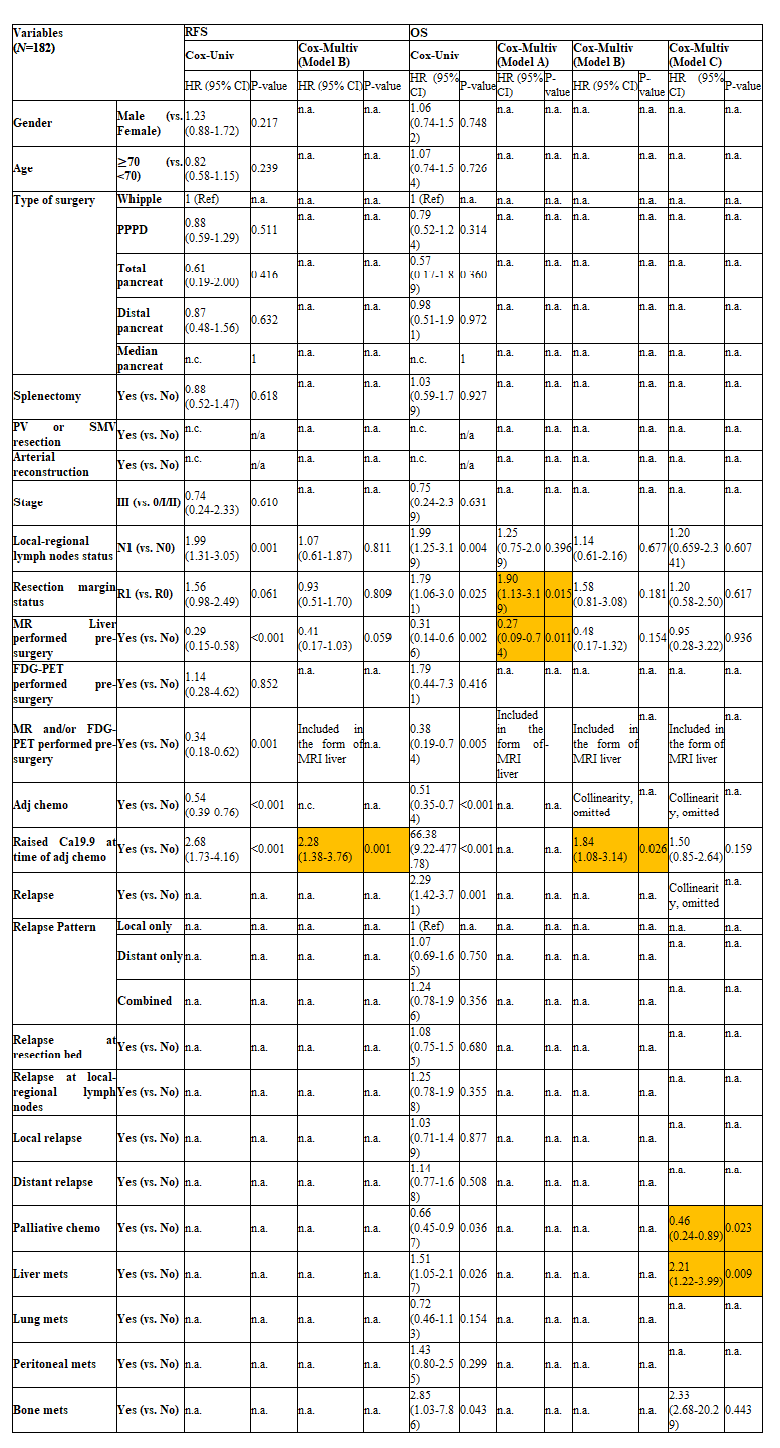
Results: One-hundred-eighty-two patients eligible: microscopically involved resection-margins (R1) 65.7%; adjuvant chemotherapy (adj) 62.1%; 78.6% relapsed. Median (months) RFS and OS were 11.4 (95%CI=9.4-13.7) and 21.6 (95%CI=17.9-18.9), respectivelly. Relapse patterns identified included: “local-only” 30.1%, “distant-only” 40.5%, “combined” 29.4%; overall, distant metastases were identified in 69.9% of patients; distant metastases were located mainly in the liver (41.3%) with a median time-to-liver recurrence of 6.64 months (95%CI 4.99-8.56)). Factors impacting on risk of relapse were: R1 [(any-pattern) (LR-multivariable: OR=4.02; 95%CI=0.02-0.23)], pre-adj CA19.9>normal limit (NL) [(‘local-only’) (LR-univariate: OR=0.23; 95%CI=0.08-0.62)] and adj [(‘combined’) (LR-univariate: OR=0.46; 95%CI=0.22-0.96)]. R1 associated with shorter OS (Cox-multivariable: OR=1.90; 95%CI=1.13-3.19) while pre-adj CA19.9>LN implied shorter RFS (Cox-multivariable: OR=2.28; 95%CI=1.38-3.76) and OS (Cox-multivariable: OR=1.84; 95%CI=1.08-3.14). Preoperative magnetic resonance imaging (MRI) liver was associated with a lower risk of relapse [(any pattern) (LR-multivariable: OR=0.06; 95%CI=0.02-0.23)] and was prognostic for longer OS (LR-multivariable: OR=0.27; 95%CI=0.09-0.74).
Conclusion: Majority of resected-PDAC patients will recur with distant metastases (liver); integrating preoperative MRI liver to patients’ pathway may improve patient selection and maximise benefit from surgery.
Pancreatic ductal adenocarcinoma (PDAC) is a lethal disease, being the fourth leading cause of cancer-related death in Europe and the United States [1, 2]. Mortality and incidence are close (estimated deaths and estimated new cases in Europe in 2018; 10.9/100,000 individuals and 11.5/100,000 individuals, respectively). Only 10-20% of patients present with early stage PDAC that is amenable to curative surgery [2, 3]. Adjuvant gemcitabine- and/or fluoropyrimidine-based chemotherapy is recommended by clinical practice guidelines [4-6], as it has been shown to reduce the risk of disease relapse and prolong recurrence free survival (RFS) and overall survival (OS) compared to surgery alone in randomised clinical trials (RCTs) [7-12].
Despite adjuvant chemotherapy, disease relapse occurs in approximately 80% of cases after initial curative treatment [10, 11], and post-resection prognosis remains poor (5-year OS; 10-30%) [2, 8, 10, 11]. More recently, an adjuvant triple-drug combination, including 5-fluorouracil, oxaliplatin and irinotecan (modified FOLFIRINOX), has been shown to provide an exceptional RFS and OS advantage over gemcitabine alone in patients with radically resected PDAC (8.8 month advantage in RFS and 19.6 month advantage in OS) [Unicancer GI PRODIGE 24/CCTG PA.6 trial] [12], and has entered the armamentarium of therapeutic options for this disease subgroup. However, patients with post-operative CA19.9 levels above 180 U/mL were excluded from this clinical trial, since raised post-operative CA19.9 levels had already been identified as negative prognostic factors in the ESPAC-3 and -4 clinical trials [10, 11]. In addition, the toxicity profile of modified FOLFIRINOX in the adjuvant setting (Grade 3-4 toxicity; 75.5%) [12], makes this combination only suitable for selected patients. Therefore, the management of resectable PDAC still represents an area of unmet need and warrants improvement.
Recent studies have explored potential identified factors related to specific relapse patters (i.e. positive lymph node ratio was predictor for distant recurrence), and concluded that distinct patterns of relapse are likely underpinned by differences in the PDAC biology [13, 14]. In addition, multiple risk factors associated with tumour recurrence have also been defined (i.e. age-comorbidity index, tumour size, CA 19-9, tumour differentiation within others) [15]. It has also suggested that specific risk factors for recurrence patterns could actually be considered for specific surveillance following surgery [16].
The present study aimed to describe relapse patterns following surgery for PDAC with a focus on identifying modifiable factors to guide development of more effective therapeutic strategies for resectable PDAC.
Materials and methods
Eligible patients were identified from those with a diagnosis of PDAC who underwent surgery with curative intent, from January 2005 to September 2017. Exclusion criteria included: any histology other than PDAC; macroscopic residual disease (R2); presence of distant metastases (M1) identified on pre-operative imaging or intra-operatively; missing information on follow-up (date of death or last follow-up visit/contact) or relapse status. Microscopic residual disease (R1) was defined as a distance between the tumour and the closest resection margin of ≤1 mm, as per indication by The UK Royal College of Pathologists [https://www.rcpath.org]. Pre- and post-operative chemotherapy were administered according to the European Society of Medical Oncology (ESMO) and the National Institute for Health and Care Excellence (NICE) clinical practice guidelines [4, 6] or in the context of ongoing clinical trials (if applicable). Clinical data and survival outcomes of patients and pathological characteristics of their tumours were retrospectively collected from electronic medical records. The disease stage was classified according to the Tumour, Node, Metastasis Classification of Malignant Tumours, 7th edition [17]. Patterns of disease relapse were classified as follows: “local only”, when the tumour relapsed at the resection bed and/or within local-regional lymph nodes, but not at distant sites; “distant only”, when the tumour relapsed at distant sites, but not locally; “combined”, when the tumour relapsed both locally and at distant sites. Time to Tumour Relapse (TTR) was measured from the date of surgery to the date of radiological evidence of disease recurrence. Relapse-free survival (RFS) was measured from the date of surgery to the date of radiological evidence of disease recurrence or death of any cause. Overall Survival (OS) was measured from the date of surgery to the date of death of any cause.
Descriptive and inferential statistical analyses were performed using the STATA v.12 software package. Means, standard deviations (SDs), medians, ranges, 95%-Confidence Intervals (95%-CIs), Student-T and Chi-squared tests, and Spearman’s Correlation were applied for continuous and categorical variables, as appropriate. Kaplan-Meier analysis was used to estimate survival outcomes. Correlation between clinical-pathological characteristics and binary outcomes (e.g. disease relapse versus non-disease relapse) was interrogated by applying univariate and multivariable Logistic regression. Correlation between clinical-pathological characteristics and survival outcomes was interrogated by applying Log-rank test, Cox-regression univariate (Cox-univariate) and multivariable (Cox-multivariable) analyses.
Baseline characteristics
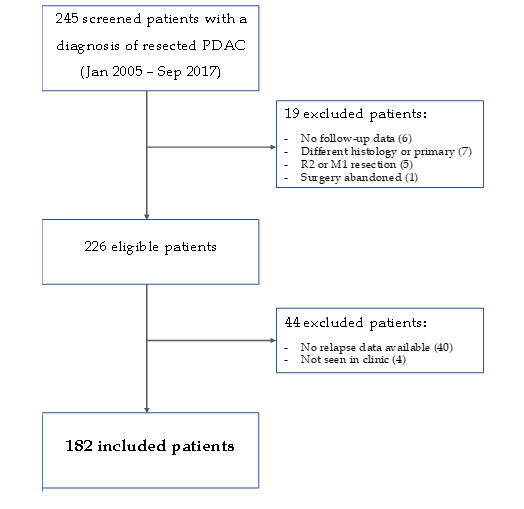
Among 245 patients initially screened, only 182 were eventually deemed eligible for inclusion in this study (flow diagram for patient selection illustrated in Supl Mat 1).
PDAC = pancreatic ductal adenocarcinoma; R2 = macroscopic evidence of residual disease; M1 = distant metastases.
The median follow-up time was 17.9 (range; 16.2-21.1) months. Baseline characteristics are summarised in
Table 1. The median age at the time of surgery was 67.9 (range; 28.3-87.2) years. Twenty-seven (14.8%) patients had a liver Magnetic Resonance Imaging (MRI) (24; 13.2%) as part of their preoperative assessment; 18-Fluoro-Deoxy-Glucose Positron Emission Tomography (18F-FDG-PET) was performed in 3 patients (1.7%).
One-hundred and seventeen (64.3%) patients received perioperative systemic treatment; 4 (out of 189; 2.2%) had only neoadjuvant chemotherapy, 108 (out of 189; 59.3%) had only adjuvant chemotherapy, and 5 (out of 189; 2.7%) had both neoadjuvant and adjuvant chemotherapy. Seventy-seven (68.1%) patients completed adjuvant treatment (6 cycles for regimens containing gemcitabine, 8 cycles for capecitabine as single agent, and 12 cycles for 5-fluorouracil as single agent). Reasons for early discontinuation of adjuvant treatment (36 patients; 31.9%) were as follows; disease relapse in 19 cases (out of 36; 52.8%), intolerable toxicities in 13 (out of 36; 36.1%), patient decision in 2 (out of 36; 5.6%) and others, not otherwise specified in 2 (out of 36; 5.6%). Among the remaining 65 (35.7%) patients who did not have chemotherapy, 7 (out of 189; 3.7%) were offered pre- or post-operative treatment, but declined, 19 (out of 189; 10.1%) had poor recovery from surgery and, therefore, were deemed not fit enough for chemotherapy, 33 (out of 189; 17.5%) were diagnosed with early disease relapse, and 6 (out of 189; 3.2%) died before starting chemotherapy. The median time between surgery and the beginning of adjuvant chemotherapy was 11 (95%-CI; 10.6-11.4) weeks.
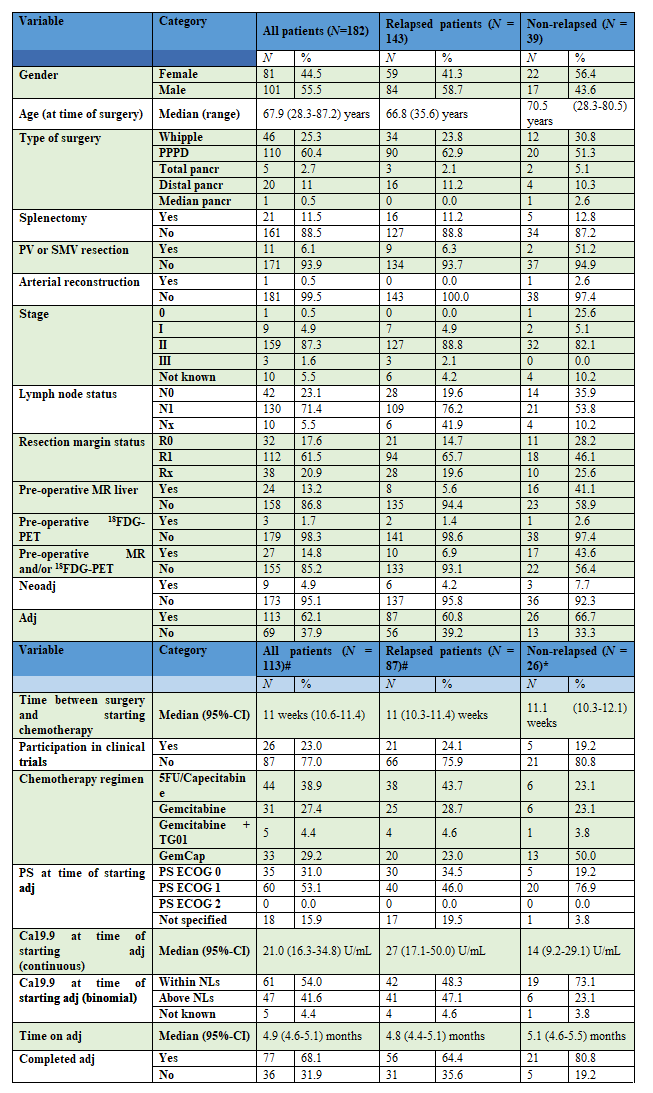
N = number; 95%-CI = 95%-Confidence Interval; PPPD = pylorus preserving pancreato-duodenectomy; pancreat = pancreatectomy; SMV = superior mesenteric vein; PV = portal vein; R0 = negative resection margin; R1 = microscopically involved resection margin; Rx = resection margin status unknown; MRI = magnetic resonance imaging; 18FDG-PET = 18-fluorodeoxyglucose positron emission tomography; Neoadj = neoadjuvant chemotherapy; Adj = adjuvant chemotherapy; 5FU = 5-fluorouracil; GemCap = gemcitabine/capecitabine; PS = performance status; ECOG = Eastern cooperative oncology group; NLs = normal limits. #Only patients who received adjuvant chemotherapy.
Tumour recurrence and associated risk factors
At the date of data cut-off, 143 (78.6%) patients had relapsed. Disease relapse was diagnosed on imaging, scheduled as part of the follow-up plan in most patients (114 out of 143; 79.8%). In the remaining cases, the development of new symptoms (27/143; 18.9%) or non-cancer related medical issues (incidental finding) (2/143; 1.4%) mandated extra-scheduled imaging which led to the diagnosis of disease relapse. Of the population of patients with tumour relapse, only 10 (5.5%) patients had a liver MRI or an 18F-FDG-PET performed before surgery. The imaging technique used to diagnose disease relapse was Computed Tomography (CT) scan (97.9%), 18F-FDG-PET (1.4%) or MRI (0.7%). Thirty-three cases (23% of those who relapsed) required further investigations to confirm the presence of disease relapse: second CT scan (2/33; 6%), MRI (12/33; 36.4%), 18F-FDG-PET (9/33; 27.3%), MRI + 18F-FDG-PET (1/33; 3.0%), biopsy (6/33; 18.2%) or re-resection (1/33; 3.0%).
Frequencies of disease relapse patterns were as follows: “local only” 43/143 (30.1%), “distant only” 58/143 (40.5%) and “combined” 42/143 (29.4%). In 85 (out of 143; 59.4%) patients, the tumour recurred at the resection bed or within local-regional lymph nodes (with or without distant metastases), and in 100 (out of 143; 69.9%), the tumour recurred at distant sites (with or without local relapse). Within the latter subgroup, the most common metastatic sites were the liver (59/143; 41.3%) and lungs (30/143; 21.0%). Among patients who developed ‘early disease relapse on post-operative imaging (POI)’, 6 (out of 32; 18.8%), 12 (out of 32; 37.5%) and 14 (out of 32; 43.7%) presented with a “local only”, “distant only” and “combined” relapse pattern, respectively, and the most common distant metastatic sites were the liver (19/32; 59.4%) and peritoneum (7/32; 21.9%).
Risk factors associated with tumour recurrence
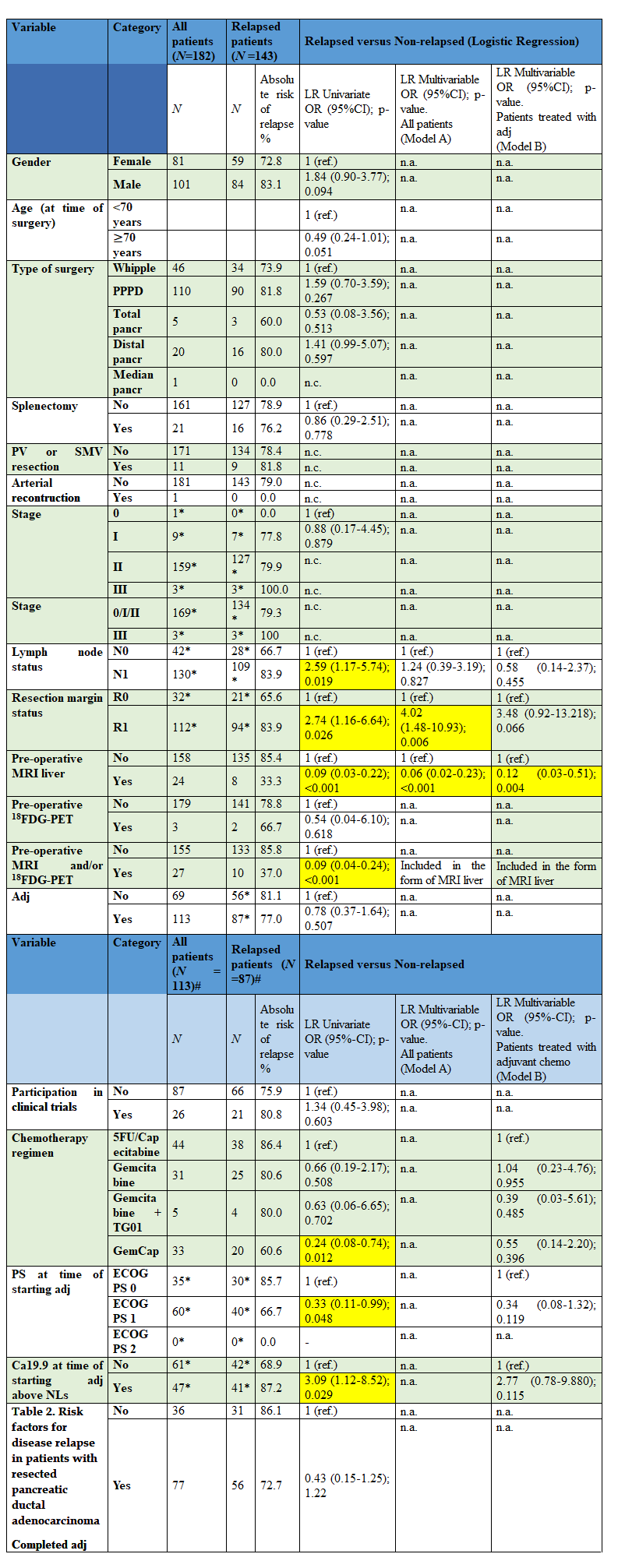
Factors associated with an increased risk of disease relapse are presented in Table 2.
In the whole patient population, the presence of microscopically involved resection margins (R1) (112/182; 61.5%) on post-operative pathological examination correlated with a significantly increased risk of disease relapse (Table 2, Model A). When limited to patients treated with adjuvant chemotherapy, levels of the serum biomarker CA19.9 above the normal limit (37 U/mL) at the beginning of the adjuvant chemotherapy, were associated with a significant increase in the risk of relapse on univariate analysis, but was not an independent factor on multivariable analysis (Table 2, Model B).
Focusing on modifiable factors amenable to easy intervention, the performance of preoperative MRI liver correlated with a significantly reduced risk of disease relapse (33.3% vs 85.4%); findings were confirmed in multivariable logistic regression both for the whole population (OR 0.06 (95%-CI; 0.02-0.23); p-value <0>
ref: category of reference; n.a.: not applicable; n.c.: could not be calculated due to limited number of observations; N = number; OR = odds ratio; 95%-CI = 95%-Confidence Interval; PPPD = pylorus preserving pancreato-duodenectomy;pancreat = pancreatectom; SMV = superior mesenteric vein; PV = portal vein; R0 = negative resection margin; R1 = microscopically involved resection margin; MRI = magnetic resonance imaging; FDG-PET = fluorodeoxyglucose positron emission tomography; LR = Logistic Regression; POI = post-operative imaging. *The sum does total 189 or 32, as cases classified as unknown/not specified were not included in the analysis and therefore are not reported in the table.
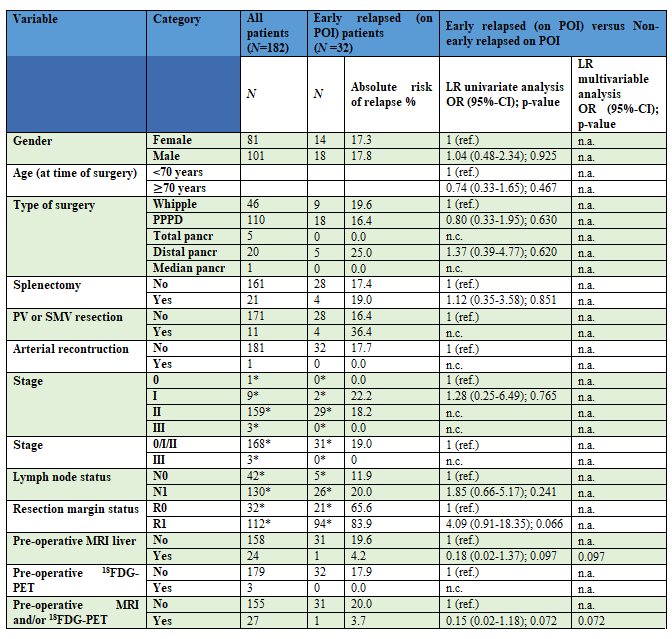
Of note, 32 out of 143 (22.3%) disease relapses were detected on POI. Factors associated with an increased risk of ‘early disease relapse on POI’ are presented in Supl Mat 2. There was a trend towards increased risk of ‘early disease relapse on POI’ for patients with R1 disease (compared to patients with microscopically clear resection margins (R0) disease), even though it did not achieve statistical significance (Supl Mat 2).
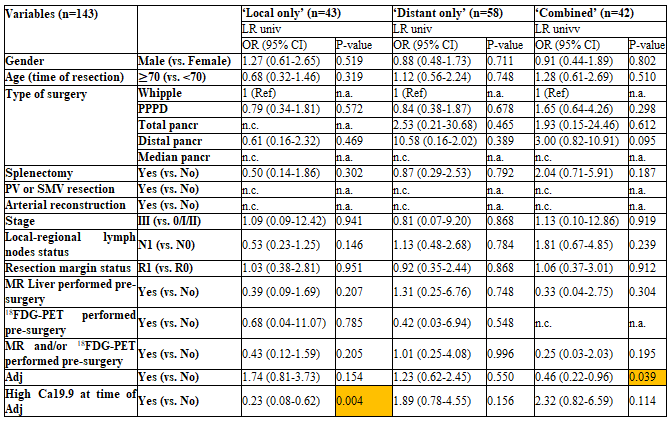
Factors related to specific patterns of disease relapse are presented in Sup Mat 3. CA19.9 levels above normal limit were associated with increased risk for ‘local only’ pattern, and the receipt of adjuvant chemotherapy was associated with a reduced risk of ‘combined’ relapse (as only a single factor for the ‘local only’ pattern and a single factor for the ‘combined’ pattern achieved statistical significance on Logistic-regression univariate analysis
(Logistic-regression multivariable analysis was not performed).
N = number; OR = odds ratio; 95%-CI = 95%-Confidence Interval; n.a.: not applicable; n.c.: could not be calculated due to limited number of observations; ref: category of reference; PPPD = pylorus preserving pancreato-duodenectomy; pancreat = pancreatectomy; SMV = superior mesenteric vein; PV = portal vein; R0 = negative resection margin; R1 = microscopically involved resection margin; MRI = magnetic resonance imaging; FDG-PET = fluorodeoxyglucose positron emission tomography; Adj = adjuvant chemotherapy; 5FU = 5-fluorouracil; GemCap = gemcitabine/capecitabine; PS = performance status; ECOG = Eastern cooperative oncology group; chemo = chemotherapy; NLs = normal limits; yrs = years; mo = months; LR Univariate = logistic regression univariate analysis; LR multivariable = logistic regression multivariable analysis. #Only patients who received adjuvant chemotherapy. *The sum does not total 189, 143, 113 or 87, as cases classified as unknown/not specified were not included in the analysis and therefore are not reported in the table. Yellow cells highlight statistically significant results.
Time-to-recurrence and relapse-free survival
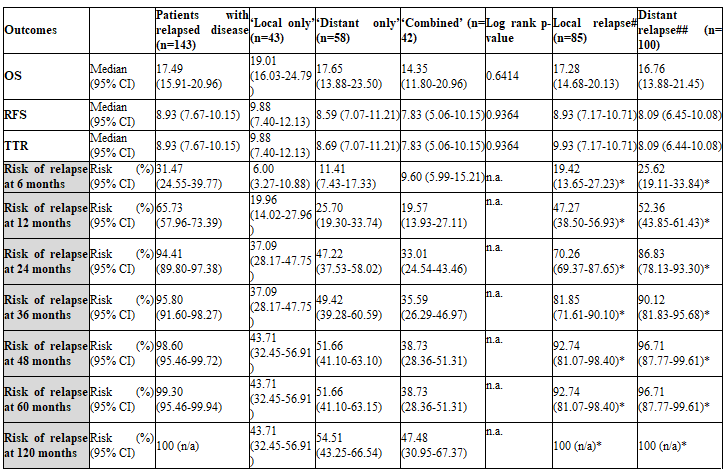
At the time of data cut-off, in the whole population: 143 (78.6%) TTR events were recorded and the estimated median TTR was 11.5 (95%-CI; 9.7-13.8) months; 144 (79.1%) RFS events occurred and the estimated median RFS was 11.4 (95%-CI; 9.4-13.7) months (Table 3).
OS = Overall Survival; RFS = recurrence free survival; TTR = Time to Tumour Relapse; 95% CI = 95% Confidence Interval; n.a. not applicable. #Local relapse = relapse at the surgical bed and/or local-regional lymph nodes with or without distant metastases; ##Distant relapse = relapse at distant sites with or without local relapse. *Risk calculated using only patients with relapsed disease as denominator.
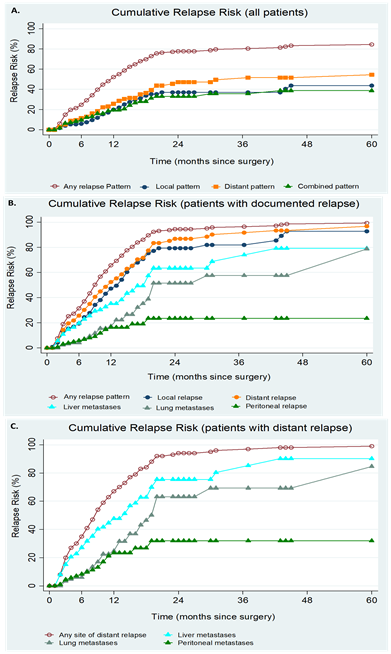
Trends in risk of disease relapse according to the relapse pattern are shown in Figure 1. Overall, the risk of disease relapse raised sharply over the first 18-24 months from surgery, then reached a plateau. Over the same time period, the risk of developing each of the three relapse patterns was similar, whereas after approximately 18-24 months, patients became more likely to develop ‘distant only’ relapse compared to the other patterns (Table 3; Figure 1). Out of the patients with documented distant metastases, liver was the site with shorter TTR (6.64 months (95% CI 4.99-8.56); full data not shown); Figure 1.C shows how liver metastases are earlier events compared to other distant sites of metastases.
Overall survival analyses
At the time of data cut-off, 122 (67.0%) deaths occurred and the estimated median OS was 21.6 (95%-CI; 17.9-18.9) months. The median OS in the subgroup of patients who did not relapse was not reached. Survival outcomes and cumulative risks of disease relapse, at different time points, in the subgroup of patients with relapsed disease and according to the relapse pattern are presented in Table 3.
Supl Mat 3: Risk of relapse according to the pattern of disease relapse in patients with relapsed disease after curative surgery for pancreatic ductal adenocarcinoma
n = number; OR = odds ratio; 95%-CI = 95%-Confidence Interval; ; n.a.: not applicable; n.c.: could not be calculated due to limited number of observations; PPPD = pylorus preserving pancreato-duodenectomy; pancreat = pancreatectomy; SMV = superior mesenteric vein; PV = portal vein; R0 = negative resection margin; R1 = microscopically involved resection margin; MRI = magnetic resonance imaging; FDG-PET = fluorodeoxyglucose positron emission tomography; Adj = adjuvant chemotherapy; LR = Logistic Regression; Local only = relapse at the resection bed and/or local regional lymph nodes but without distant metastases; Distant only = relapse at distant sites but without local relapse; Combined = local + distal relapse; LR = logistic regression; univ = univariate analysis. Yellow cells highlight statistically significant results.
Within the whole patient population, R1 status (HR=1.9, 95%-CI; 1.13-3.19, Cox-multivariable-p=0.015) and the performance of preoperative MRI liver (HR=0.27, 95%-CI; 0.09-0.74, Cox-multivariable-p=0.011) were independent prognostic factors for OS on Cox-multivariable (Supl Mat 4, Model A). Among patients who received adjuvant chemotherapy, pre-adjuvant CA19.9 levels above normal limit was the only independent prognostic factor for shorter RFS (Hazard Ratio (HR)=2.50, 95%-CI; 1.58-3.96, Cox-multivariable-p<0 HR=1.84, p=0.026)>Supl Mat 4, Model B). Among patients who relapsed, the presence of liver metastases (HR=2.21, 95%-CI; 1.22-3.99, Cox-multivariable-p=0.009) and the receipt of best supportive care (versus palliative chemotherapy) (HR=0.46, 95%-CI;
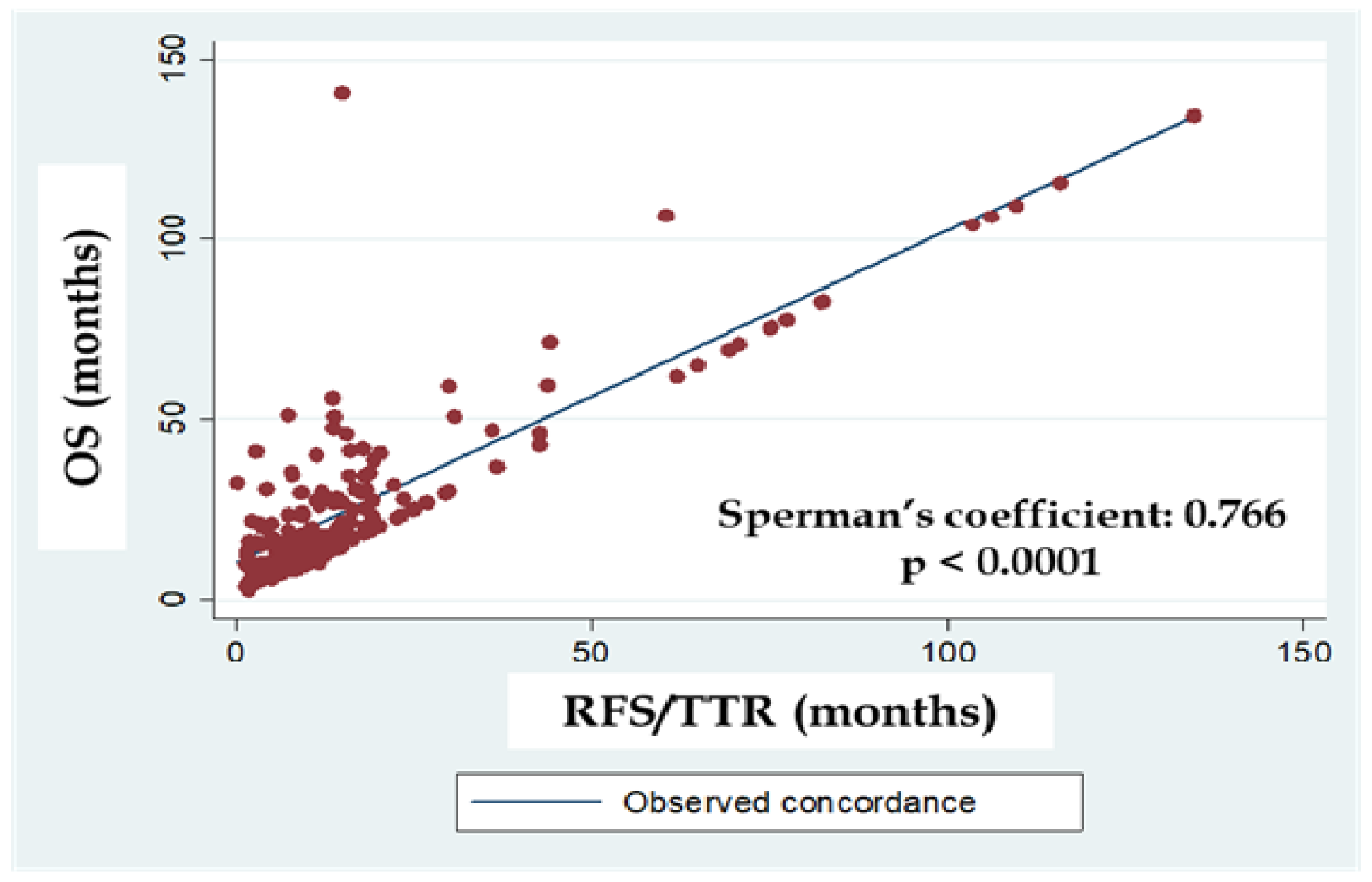
0.24-0.89, multivariable-p=0.021) were the only factors independently associated with shorter OS on Cox-multivariable (Supl Mat 4, Model C). Disease relapse patterns did not impact on OS (Supl Mat 4 and Figure 2.C). Whether survival outcomes were influenced by the regimen of adjuvant chemotherapy administered was not explored, as subgroups per chemotherapy regimen (gemcitabine alone, gemcitabine/capecitabine, gemcitabine/TG01, 5-fluorouracil or capecitabine) were too small to allow reliable comparisons. The correlation between TTR and OS was interrogated and is presented in Supl Mat 5.
Among patients who received palliative treatment (chemotherapy or chemo-radiotherapy) for advanced disease (n = 95), those with initial ‘local only’ relapse had a better median PFS (7.91 months, 95%-CI; 5.98-12.87) compared to those with ‘distant only’ (5.98 months, 95%-CI; 3.19-8.21) or combined (4.33 months, 95%-CI; 2.20-7.36) pattern of fist relapse (p=0.013).
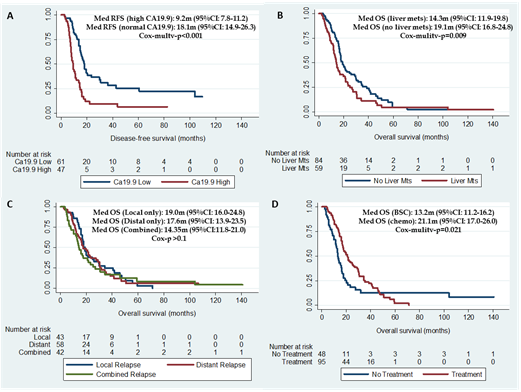
RFS = recurrent free survival; OS = overall survival; m = months; mets = metastasis; chemo = chemotherapy; BSC = best supportive care; Local only = relapse at the resection bed and/or local regional lymph nodes but without distant metastases; Distant only = relapse at distant sites but without local relapse; Combined = local + distal relapse; Cox-multiv = Cox-regression multivariable analysis.
Model A includes all patients; Model B includes patients who received adjuvant treatment; Model C includes patients with disease relapse.
RFS = recurrence free survival; OS = overall survival; N = number; 95%-CI = 95%-Confidence Interval; n.a.: not applicable; n.c.: could not be calculated due to limited number of observations; PPPD = pylorus preserving pancreato-duodenectomy; pancreat = pancreatectomy; SMV = superior mesenteric vein; PV = portal vein; R0 = negative resection margin; R1 = microscopically involved resection margin; N1 = metastatic local-regional lymph nodes; N0 = negative local-regional lymph nodes; Local only = relapse at the surgical bed and/or local-regional lymph nodes without distant metastases; Distant only = relapse at distant sites without local relapse; combined = local + distant relapse; Local relapse = relapse at the surgical bed and/or local-regional lymph nodes with or without distant metastases; Distant relapse = relapse at distant sites with or without local relapse; adj = adjuvant; chemo = chemotherapy; mets =metastases; Cox-Univ = Cox-regression univariate analysis; Cox-Multiv = Cox-regression multivariable analysis. Yellow cells highlight statistically significant results.
Discussion
The present study provides real-world data from a large retrospective cohort of patients with potentially curable PDAC, and confirms that PDAC has a high likelihood of relapse, predominantly at distant sites (mainly liver), even when diagnosed at an early stage and resected with radical intent. Results from this study also support that relapse is usually an early event following surgery in PDAC, with a significant number of patients being diagnosed with ‘early disease relapse on POI’. Based on these facts, it is likely that, in order to improve outcomes following surgery, further work may need to be done towards an adequate selection of patients for surgery. Is this high rate of early distant relapse reflection of occult metastases at time of surgery? If so, how can we avoid unnecessary surgery on this patient population?
This study showed confirmed, as previously shown, that liver metastases are main site of recurrence following reseaction of PDAC. In addition, risk of relapse seemed lower for those patients who underwent a preoperative MRI liver. Even though the number of patients in this cohort was small and results require validation, we could suggest that the integration of preoperative MRI liver to patients’ pathway may improve patient selection and maximise benefit from surgery in PDAC.
While there is no standard recommendation regarding the role of MRI liver before surgery, the most recent UK NICE guidelines [6] recommend the use of 18F-FDG-PET for all patients with early stage or locally advanced PDAC, before starting any treatment, with the aim of minimising the risk of misdiagnosis of distant metastases, and delivering the most appropriate management. This recommendation is based on the results of the PET-PANC study that confirmed that 18F-FDG-PET provides significant incremental diagnostic benefit and influences the staging and management of patients diagnosed with PDAC [18]. This study recruited 589 patients with suspected pancreatic cancer and influenced the staging of PDAC in 56 patients (14%) and influenced management in 250 (45%) patients. Based on these findings, it was concluded that use of 18F-FDG-PET in the pre-operative setting resulted in avoidance of inappropriate surgery in 58 patients (20%) who were due to have surgery based on CT scan results. It is worth highlighting that the patients reported in this series were treated before the latest update of NICE guidelines [6]; which explains the low number of preoperative 18F-FDG-PET and the challenges to assess the impact of preoperative 18F-FDG-PET due to limited power. Similar to UK practice, the 2018 US National Comprehensive Cancer Network (NCCN) guidelines also suggest considering 18F-FDG-PET (or MRI), after conventional CT scan, to integrate preoperative staging investigations in patients at higher risk for extra-pancreatic disease [5].
There is growing interest in the field and some studies have explored the role of novel techniques for identification of occult liver metastases. In the study by Katada et al. [19], hepatic micrometastases were histologically confirmed in 15% of patients without visible liver lesions; when images where retrospectively reviewed, focal circular alterations presenting arterioportal shunts were seen in 50% of the patient with micrometastases. This suggests that occult liver metastases may be missed in a significant proportion of our patients. Whether the incorporation of preoperative 18F-FDG-PET +/- MRI liver would change patient management and outcome requires further studies but seems a pathway worth exploring. In a retrospective study reporting on 117 patients who had aborted pancreatic surgery due to intraoperative evidence of micro-metastases (mostly affecting the liver and peritoneum), preoperative CA19.9 levels above >192 U/mL and the presence of indeterminate liver lesions on pre-operative imaging were amongst statistically significant risk factors for micro-metastases at diagnosis [20]. Increased CA19.9 levels have been reported to have prognostic significance in the preoperative setting [21], and their role as a potential tool for identifying the most suitable candidates for curative surgery should be explored further (however acknowledging limitations in jaundiced patients in whom a “false” elevation of CA19.9 could be observed [25]).
Identification of novel biomarkers and a better understanding of the pathways involved in the process of tumour metastasis are likely to improve our understanding in the coming years and aid patient selection for surgery [22-24]. Circulating biomarkers, such as circulating tumour cells and circulating tumour DNA, have been increasingly explored in clinical trials as prognostic and predictive markers (e.g. NCT03145961 or NCT02994511 available at https://clinicaltrials.gov) and, in the near future, may aid in early detection of micro-metastases, overcoming the limitations of conventional imaging, and, therefore optimising patient selection for surgery.
The role of peri-operative chemotherapy in PDAC is also being developed and could become a ‘game-changer’ in PDAC if shown to benefit patients. Neoadjuvant/perioperative strategies for resectable and borderline resectable disease are currently under investigation in clinical trials (e.g. NCT02749136, NCT02318095, NCT03572400 available at https://clinicaltrials.gov), with the aim of increasing the chance of achieving clear resection margins and improving systemic disease control. Furthermore, upfront systemic treatment may allow selection of patients who develop metastatic disease in the first few months from diagnosis, and who would therefore not benefit from surgery.
The current study did identify some factors which correlated with increased risk of relapse, most of them already identified by other research groups. These were non-modifiable and therefore difficult to be utilised to inform on patients management. Such factors included positive resection margins, the involvement of local-regional lymph nodes (N1) and post-operative/pre-adjuvant CA19.9 levels have been identified as independent negative prognostic factors for OS in randomised studies in the adjuvant setting of PDAC [8-11, 25].
The rate of ‘early disease relapse on POI’ in the present series was higher (22%) than that one reported in previous studies (<10>
In the present study, the presence of R1 resection margins was associated with an increased likelihood of disease relapse (any pattern) and was an independent negative prognostic factor for OS in the whole population of resected patients. The lack of impact of R1 status on RFS may be due to the small sample size of the R0 subgroup (32 patients), which may have negated a statistically significant difference. The smaller proportion of R0 resections in the present study compared to other series from the literature (65-83%) [7-10, 25] is likely the result of the use of a less restrict definition of complete surgical clearance (absence of tumour on the resection margin, 0-mm clearance) in those series, as there is disagreement surrounding the definition of pathological margin status across geographical areas. Pre-adjuvant CA19.9 levels above the normal limit did not seem to impact on the overall risk of disease relapse, but did correlate with a higher risk of ‘local only’ disease relapse. This likely indicates that high post-operative CA19.9 levels actually identify patients that should not have undergone potentially curative surgery. Interestingly, among patients who received adjuvant chemotherapy, pre-adjuvant CA19.9 was prognostic for RFS and OS, suggesting that this biomarker may be useful in clinical practice to identify patients with worse prognosis who could benefit from closer biochemical and radiological follow-up. In the present study, there was a trend towards increased risk of relapse and worse RFS and OS for patients with N1 disease, which, however, did not maintain the statistical significance when other factors were included in a multivariable model. Likewise, the receipt of adjuvant chemotherapy did not reduce the overall risk of disease relapse, nor improved RFS or OS, which is in contrast with what was shown in randomised clinical trials evaluating adjuvant chemotherapy compared to observation alone [8, 9]. The lack of impact of the status of local-regional lymph nodes or of adjuvant treatment on the likelihood of relapse and survival outcomes may be explained by the lack of randomisation and the presence of selection bias in the current series.
The relapse patterns shown in this series do match with previous studies [13, 14], with a predominance of distant metastases and a trend towards shorter time-to-relapse being identified for liver metastases. In addition, relapse rates and survival outcomes from the present cohort of patients are in line with data from large randomised clinical trials in the curative setting [7, 8, 10, 11], indicating that patients with localised PDAC treated in this series received appropriate management, in line with the current evidence. This is further corroborated by: (1) the limited length of in-hospital stay; (2) the receipt of neoadjuvant and/or adjuvant systemic treatment by nearly two thirds of patients; (3) the recruitment of approximately 25% of patients into clinical trials; (4) the completion of the pre-planned 6, 8 or 12 cycles of adjuvant chemotherapy by two thirds of patients, which fits with completion rates of adjuvant treatment in randomised studies (55-79%) [8, 11, 12]. The median time between surgery and the beginning of adjuvant chemotherapy (~90 days) was longer than in other prospective studies (36-65 days) [8, 10, 11]. However, a retrospective analysis of the ESPAC-3 trial indicates that, while the failure of completion of the whole pre-planned course of adjuvant treatment negatively affects both RFS and OS of patients with resected PDAC, delays in the start of the adjuvant treatment have no impact on survival outcomes [26]. Limitations derived from the retrospective design of the study apply. In addition, selection bias may be present for many of the variables explored (i.e. adjuvant treatment).
Limitations of the study derived from its retrospective design and single centre source. In addition, selection bias cannot be excluded and low rate of patients undergoing pre-operative MRI liver and 18F-FDG-PET difficult data interpretation. The fact that the reported series covers for a prolonged period of time, introduces the bias of practice changes during that period of time such as changes in surgical techniques and available adjuvant strategies.
In conclusion, surgery for PDAC results in cure in a limited number of patients; relapses are frequent and do happen early after surgery with a tropism for the liver. Biomarkers for early detection of occult metastatic disease with a high risk of disease recurrence are needed and while new circulating biomarkers and novel treatment strategies such as perioperative chemotherapy are developed, clinicians do rely on current imaging available to face this issue. These results suggest that the incorporation of preoperative MRI liver to patients’ pathway could inform a better patient selection by identifying occult liver metastases. Further studies are required to confirm these findings and to understand how/if to combine preoperative MRI liver and 18F-FDG-PET in patients’ pathway.
Acknowledgement:Dr Angela Lamarca was part funded by the ASCO Conquer Cancer Foundation Young Investigator Award and The Christie Charity.
Conflict-of-interest statement:Authors have no conflict of interest to declare related to this manuscript. This manuscript is not under consideration for publication elsewhere
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
