
Case Report | DOI: https://doi.org/10.31579/CCOR-2021/001
*Corresponding Author: Christos Sotiropoulos, Department of Gastroenterology-Hepatology, University General Hospital of Patras “Holy Mary the Help”, Patra, Greece
Citation: Christos Sotiropoulos, Sakka E. (2021) Radiographic Evaluation of Supraclavicular Lymphadenopathy: A Case Report. Clinical Cancer and Oncology Research 1(1) DOI: 10.31579/CCOR-2021/001
Copyright: © 2021, Christos Sotiropoulos, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 May 2021 | Accepted: 14 June 2021 | Published: 21 June 2021
Keywords: lymphadenopathy, supraclavicular lymphadenopathy, cervical lymph nodes, radiographic evaluation, malignant disease
Lymphadenopathy is defining the swelling of lymph nodes and may be a clue of an underlying disorder from a usual self-limited infectious disease in younger patients to a malignant disease in older ones. In the absence of supraclavicular lymphadenopathy the normal skin diving in the supraclavicular fossa defines a radiopaque line over and parallel to the upper lip of the clavicle in the chest X-ray examination. We report an 85-year-old female patient with a medical history of breast cancer in both breasts and bilateral mastectomy with no signs of supraclavicular lymphadenopathy at presentation and a chest X-ray examination revealing a radiopaque line over and parallel to the upper lip of the clavicle. Six months later, the same patient developed swollen supraclavicular lymph nodes in the right supraclavicuar fossa and a chest X-ray examination revealed a disappearance of the normal radiopaque line above the clavicle. The appearance of this radiographic sign may indicate swollen cervical lymph nodes and may be an alert to search for a malignancy. Thus, clinicians should take a careful history, examine thoroughly the patient and perform a detailed radiographic evaluation.
Lymphadenopathy refers to the swelling of lymph nodes and can be central and/or peripheral [1]. Peripheral lymph nodes are located deep in the subcutaneous tissue and clean antigens from the extracellular fluid [2]. In general, a normal sized lymph node is less than one cm in diameter, but can be palpated if enlarged [2]. The enlargement can be caused by bacterial, viral and fungal infections, autoimmune diseases and malignancies [1]. Detection of swollen lymph nodes is an alerting sign that advocates for a detailed examination of the patient [2]. When inspecting for lymphadenopathy the physician should perform a careful examination of all anatomical regions, including the head and neck, supraclavicular, axillary and inguinal regions [1]. Cervical lymph nodes are a common site of metastases [3]. The commonest malignant tumors include aerodigestive tract malignancies, thyroid tumors, skin cancers, head and neck malignancies, lymphomas, breast cancer, lung cancer and tumors of the central nervous system [3].
We report a patient treated in our department for anemia presenting with supraclavicular lymphadenopathy, whose radiographic evaluation revealed a useful radiographic sign. This case report supplements and supports the literature exposing the necessity of careful and multiple investigations in order to establish a nearly diagnosis for adequate treatment.
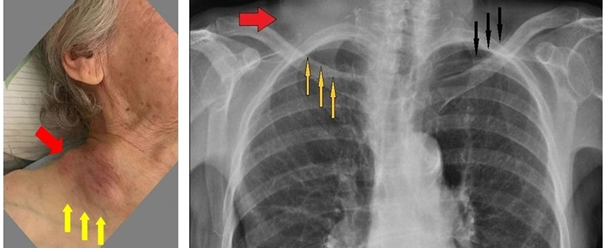
An 85-year-old female patient with a medical history of breast cancer in both breasts and bilateral mastectomy, colon diverticulosis and gastric angiodysplasias was admitted to our hospital for blood transfusion due to anemia. The physical examination revealed a normal skin diving in the supraclavicular fossa and no signs of supraclavicular lymphadenopathy (Figure 1) and the chest X-ray examination revealed a radiopaque line over and parallel to the upper lip of the clavicle (Figure 2).
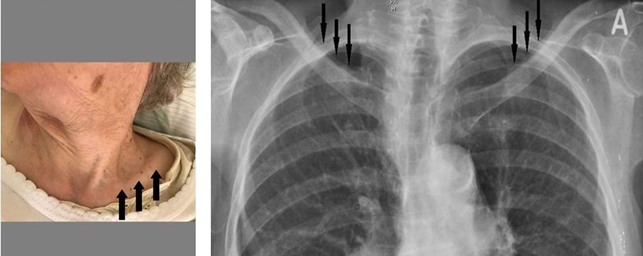
Six months later, the same patient was hospitalized again for blood transfusion and during the physical examination we discovered swollen supraclavicular lymph nodes in the right supraclavicuar fossa (Figure 3) and a chest X-ray examination revealed a disappearance of the normal radiopaque line above the clavicle (Figure 4).
Peripheral lymphadenopathy is frequently due to a local or systemic, benign and self-limited infectious disease [2]. However, it could be a manifestation of underlying malignancy [2]. Malignant supraclavicular lymphadenopathy can be present in the context of abdominal/thoracic neoplasms, thyroid cancer, Hodgkin's disease, non-Hodgkin's lymphoma and breast carcinoma [2].
Imaging can identify lymph node characteristics more accurately than can physical examination [2]. Ultrasonography is a useful imaging tool in the assessment of the number, size, shape and internal structure in patients with peripheral lymphadenopathy, whereas Computed Tomography scan and Magnetic Resonance Imaging are more useful in the evaluation of the thoracic and abdominopelvic cavity [2].
During the radiographic imaging of the body structures in the chest X-ray examination the normal skin diving in the supraclavicular fossa defines a radiopaque line over and parallel to the upper lip of the clavicle. When a body structure in the supraclavicular fossa raises the skin this normal skin diving is elevated and this results in the radiographic disappearance of this line.
This radiology sign is extremely useful when in a chest X-ray we have a unilateral or bilateral absence of this line, then the physician should repeat thoroughly the physical examination by focusing on palpation and searching for swollen supraclavicular lymph nodes. However, further radiographic imaging can identify the size and distribution of the nodes more accurately.
Peripheral lymphadenopathy is a common finding in routine clinical practice. According to this case report, the radiographic sign described above due to supraclavicular lymphadenopathy can be a useful red flag sign for patients suspected for malignant disorders. Our observation does not come to replace other diagnostic tools and findings but only to strengthen the physician’s effort during the diagnostic approach.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
