
Research Article | DOI: https://doi.org/10.31579/2637-8914/050
1 Clinical dietitian, Ruba Musharbash Center for Nutrition Counseling, Amman, Jordan.
2 Nutrition Department, Faculty of Pharmacy and Medical Sciences, University of Petra, Amman, Jordan.
3 Research Associate & Dietitian, Population Health Sciences Institute, Newcastle University, NE4 5PL. UK.
4 Nutritionist, Ruba Musharbash Center for Nutrition Counseling, Amman, Jordan.
*Corresponding Author: Ruba Mousa Musharbash, Clinical dietitian, Ruba Musharbash Center for Nutrition Counseling.
Citation: Ruba M Musharbash, Nour A Elsahoryi, Andrea McGrattan, Samantha Al-Alam, Lara Badawi, (2021). Prevalence of Food Addiction during Covid-19 Pandemic in Amman, Jordan: A Cross Sectional study. J. Nutrition and Food Processing, 4(4); DOI:10.31579/2637-8914/050
Copyright: © This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 April 2021 | Accepted: 30 April 2021 | Published: 05 May 2021
Keywords: food addiction; obesity; quarantine; COVID-19; food craving; chi-square test; insulin; leptin; ghrelin; homeostasis; etiology
Aim: Emerging evidence highlights the impact of stressful conditions on eating behaviours, particularly the consumption of foods high in salt, sugar and fat. The impact of the Coronavirus disease-19 (COVID-19) pandemic on food addiction is still un-estimated. This study aimed to examine the prevalence of food addiction among the Jordanian population during the quarantine.
Materials and methods: A Cross-sectional study has been conducted between the 27th of April and the 4th of June of 2020. An online survey of Yale food addiction scale v.2.0 (YFAS 2.0) was distributed. A convenience sample was collected through social media sites. Differences in socio-demographic characteristics were analysed using t-test and chi-square tests. Food addiction was classified based on the scoring scale. Determinants of food addition were predicted by using multivariate logistic regression.
Results: The results revealed that the prevalence of food addiction was 21.5% among adults. Among food addiction participants, 76.4% were diagnosed as severely food addicted. More than 50% of the participants reported high consumption of foods rich in sugar, salt, and fat (48.2%, 51.8%, and 52.5%, respectively). Overweight and obese young adults were more likely to have food addiction compared to normal weight. The multinominal logistic regression model revealed that there was no determinants of food addiction among adults.
Conclusion: During the first months of the quarantine, the prevalence of food addiction was higher among obese and overweight adults compared to normal-weight adults.
Coronavirus (COVID-19) is a severe respiratory syndrome caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [31]. It spread rapidly and causes increased worldwide [46]. The World Health Organization (WHO) declared COVID-19 as a pandemic in March 2020. On the 17th of March, Jordan declared the national defence law, where a complete lockdown was launched with strict rules on citizens’ mobility, to mitigate the spread of the virus [27]. The lockdown and quarantine, due to COVID-19, affected people’s behaviors, economics [38], social and general health status [6]. Staying at home with limitations of outdoor activities, and less mobility, caused an increase in boredom and stress [31]. Consequently, all these stressful events are well known to affect eating patterns, affecting people’s choices of food [21].
Additional stress can encourage people to overeat, especially craving specific comfort and palatable foods [37]. This intense desire to consume specific foods was previously described as a food craving, which is a multidimensional concept, including emotional, cognitive and physiological processes [43]. The concept of Food Addiction (FA) can be presented as the phase where foods, mainly rich in sugar, salt and fat are potentially addictive, and that specific forms of overeating may be viewed as addictive behaviour [36]. It is now used to explain the etiology and maintenance of some forms of obesity [29]. The Yale food addiction scale 2nd version (YFAS 2.0) is used to examine FA, it is a diagnostic self–report questionnaire of addiction eating behaviour [1].
To the best of the authors’ knowledge, the effect of COVID-19 on FA has not been studied before. Quarantine may have affected the eating behaviours of Jordanians. Thus, this study aimed to examine the FA prevalence among adults in Jordan during the first four weeks of the quarantine.
1. Study Design
A cross-sectional study was conducted among Jordanian adults -aged more than 18 years. Data were collected from the 27th of April until the 4th of June 2020 by using an online questionnaire. The respondents were chosen using convenience sampling (non-probability sampling method) due to the lack of a population sampling system [10]. The online questionnaire opened from April to the end of June 2020. A consent form was included on the first page and ‘agree and continue’ choice could be selected for those who agreed to participate in the survey.
The guidelines for strengthening the Reporting of Observational Studies in Epidemiology (STROBE-nut) were used to write this article [51].
2. Study Tool
In the current study, the questionnaire included two parts; the first part included socio-demographic. The second part included YFAS 2.0, which is an instrument that assesses addictive-like eating behaviours using the criteria for substance use [28, 30]. Valid and reliable Arabic version copy was published in previous work in Jordan [16].
The scale is composed of a 35 item self-reported questionnaire that applies eleven Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria [36,42]. The scale gives two scoring options, the YFAS symptoms count [34,41], which indicates the number of dependence symptoms that have been met and the dichotomous version [31,50]. The measures of items are scored using a scale count ranging from never (0) to every day (7) indicating the number of dependence symptoms [28]. The participants with FA are diagnosed when having at least 3 symptoms with clinically significant impairment or distress [26,45]. The scale finally will subdivide the participants into four groups according to the severity of FA: mild, moderate, severe FA and non-FA [34,41].
3. Participants
Participants were asked to complete the questionnaire and answer the questions related to their eating behaviours during the quarantine period from the beginning of the lockdown in Jordan.
The inclusion criteria of this study were: (1) adults aged ≥ 18 years old; (2) currently living in Amman (capital city of Jordan) during the lockdown due to the COVID -19 pandemic. Submitted responses that did not match the inclusion criteria were excluded. The study was approved by the Institutional Review Board and the ethical committee of Petra University, Amman, Jordan (Grant number: 2Q/3/2020).
4. Statistical Analysis
Descriptive statistics, including frequencies, percentages, and cross-tabulation were collated to find the relationship between FA and socio-demographic characteristics of the participants. Food addiction was classified as mild, moderate, severe based on the scale scoring [41] for the participants who have FA during the study time. The rest of the analysis was performed on the FA participants. Cross-tabulation was used to assess the relationship between the symptoms of FA and the FA categories. Multinominal logistic regression was used to predict the socio-demographic characteristics that could be determinants for FA among adults in this study. The significant level (p-value) in this study is ≤ 0.05. The data were analysed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). BMI was measured using self-reported weight and height and calculated by dividing weight in kilogram by height in meters squared [8].
1. Participants Characteristics
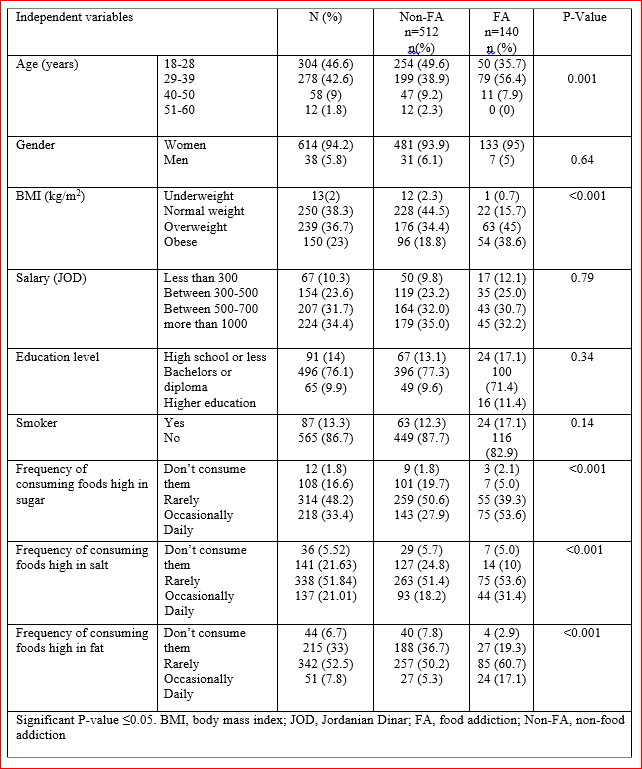
The total number of 718 participants has completed the survey, only 652 met the inclusion criteria. The majority of the participants were women (94.2%), mean age was (30 ±7.7), and more than a quarter of the respondents were between 18-28 years old (46.62%). Moreover, the anthropometric results indicated that more than the half of participants were overweight or obese (59.6%), mean body mass index (BMI) was (26.9±5.5). Nearly half of participants consumed more foods that are rich in sugar, salt and fat occasionally (48.2%, 51.8%, 52.5%), respectively.
2. Prevalence of FA categories among the study participants
From the total sample, 21.5% (n=140) met the clinical threshold for FA. Based on YFAS scale score analysis, the FA is classified into three categories: mild, moderate and severe. Within the FA group, the participants were distributed to 10%, 3.6% and 76.4% as mild FA, moderate FA and severe FA as shown in Table 1.
3. Relationship between FA groups and the socio-demographic characteristics of the study population
As shown in Table 2, The relation between age, BMI, frequency of eating foods rich in (salt, sugar and fat) and FA variables were significant, X2 (1, N = 642) = 16.002, p= 0.001, = 47.434, p= 0.001, = 20.539, p= 0.001, = 39.016, p= 0.001, = 36.253, p= 0.001, respectively. Adults who are 29-39 years old, overweight, eating foods high in sugar daily and occasionally eating foods high in salt and fat, were more likely to be food addicted than others.
4. Relationship between FA categories (mild, moderate and severe) and the socio-demographic characteristics of the study population
As shown in Table 2, a chi-square test of independence was performed to examine the relationship between socio-demographic and eating lifestyle and the FA categories. The relation between frequency of consuming foods rich in sugar and FA categories was significant, X2 (1, N = 642) = 19.28, p= 0.004.
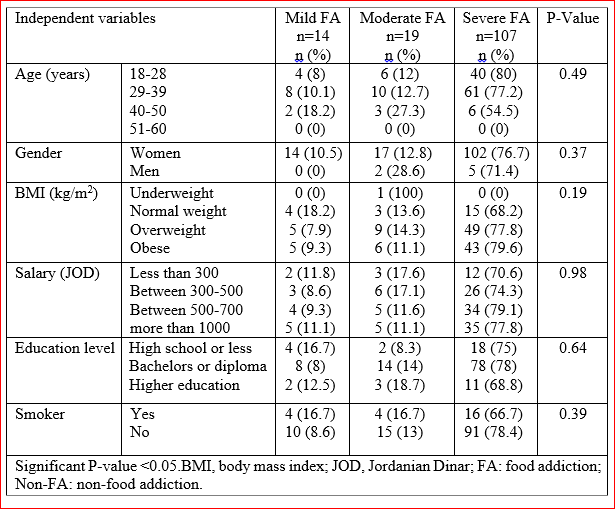
Adults who eat foods high in sugar are more likely to be severely food addicted than others.
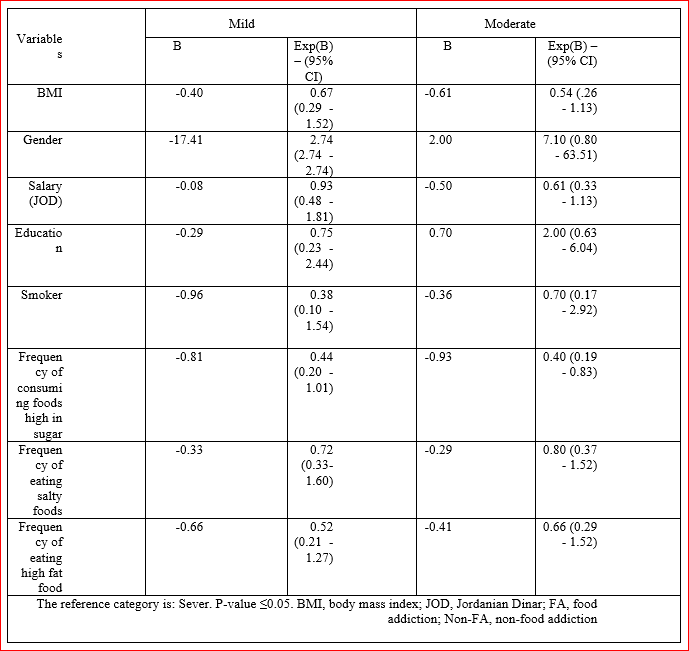
In table 3 the multinomial logistic regression results present a significant prediction between moderate FA and consumption of frequency of consuming foods high in sugar (b=-0.993, s.e.= .379, p 0.014) and these results are consistent with the chi-square test.
5. The relationship between FA symptom scores and frequency of symptoms among food addicted participants.
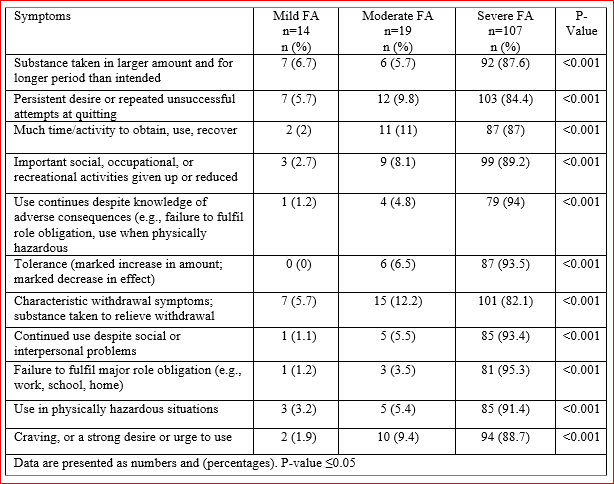
The mean symptoms score for the whole sample was 2.95± 3.50, and 7.95± 2.85 for the FA group. Table 4. Illustrates the percentages of individuals with different levels of FA that reported each of the eleven symptoms. The most frequent symptoms reported in the whole sample were “Important social, occupational, or recreational activities given up or reduced” (36.5%), and “Characteristic withdrawal symptoms; substance is taken to relieve withdrawal” (34.7%). Among individuals who have severe FA the main symptoms reported were, “Characteristic withdrawal symptoms; substance taken to relieve withdrawal” (82.1%), followed by “Persistent desire or repeated unsuccessful attempts at quitting symptom” (84.4%). Meanwhile, the less frequent symptom in both the whole sample and in the group, who met the FA criteria was “Use continues despite knowledge of adverse consequences (e.g., failure to fulfil role obligation, use when physically hazardous” 16.7%, 60%, respectively.
Many studies have been published recently on eating behaviours during the COVID-19 quarantine [12,20,21]. To our knowledge, no studies are available on the prevalence of FA during the COVID-19 pandemic quarantine.
The percentage of participants who are Food addicted in our study is considered high compared to other countries [4,5,45]. A previous study conducted in Jordan concluded that the prevalence of FA (n=4479) was 36.7%, FA was significantly greater among young adults aged 18-34 years, overweight and obese participants [16]. Another study in Egypt concluded that the FA prevalence was 15.7% in the studied sample [26]. Furthermore, a cohort study additionally reported that FA among middle aged US young women was higher among the younger proportion, and the majority of the population that was diagnosed with FA fell into the overweight category [9]. Obesity and FA have been the most studied in the literature; recent meta-analysis studies concluded that the prevalence of FA was higher in the population that fell in the overweight and obese persons [36,39].
However, Jordan is considered one of the highest countries in the prevalence of obesity and overweight, consisting of 69.6% of the whole population who are overweight [52]. Most of the women with FA in our sample were overweight or obese, and this was also evidenced in previous studies [7,17,18,19,24]. Results from the same studies showed that youth scored the most for severe FA [45,36]. One possible explanation could be that respondents from young age groups are more exposed to food cues and changes in their dietary lifestyle and habits. Furthermore, they may be at greater risk of emotion-induced eating and exposure to stress factors [36]. The stress during the quarantine could be related to changing eating behaviours and emotional eating during the lockdown time. A very recent study in Saudi Arabia concluded that half of the women in the study sample have suffered from emotional eating during quarantine, and increased intake of foods rich in sugar and fat markedly with increased stress levels [2]. A similar study during quarantine reported an increase of daily food intake by almost 50% of the respondents and by the variety of food choices; hence, consuming fewer fruits and vegetables and consuming dairy, meat and fast foods [12,21].
Stress can disrupt eating behaviour and encourage eating high palatable foods [14]. Therefore, the activation of the reward circuit; hence the mesolimbic dopaminergic system secretes dopamine in the ventral tegmental area (VTA) [16,25]. Insulin, leptin, and ghrelin also play a key role in the homeostasis of eating behaviors [11,23]. Leptin decreases food intake and decreases the firing rate of dopamine release through signalling in the ventral tegmental area (VTA) [15]. Ghrelin, leptin antagonist, increases food intake and influences the signaling in the VTA [22]. Insulin increases food intake by increasing the release and firing of dopamine in the VTA [3,13].
The results of the current study showed that some of the respondents had consumed palatable foods during the stressful condition of quarantine due to the COVID-19 pandemic. Some studies were in agreement as they mentioned that the pandemic changed the consumption patterns [32]. Respondents reported high-stress levels during the COVID-19 pandemic that led to the increased binge-eating [48]. Stress and emotional eating have also been studied as there was a strong positive relationship between increased emotional eating and stress induced by quarantine [47,53].
The mean symptoms score in the whole sample was high compared with other studies [1,29,49]. Also, higher in FA group, compared to in a previous Jordanian study [16].
There were many limitations to consider in this study. First, this study does not compare the presence of FA before and after the pandemic. Therefore, the results compared with different populations. Second, the majority of the participants who completed the online survey were women, this may be explained by higher interest in health topics in women compared to men. The strengths of this study are that it is the first study globally and in Jordan discussing the FA status during the quarantine, and the use of a strong scale to measure FA among the participants. More longitudinal studies are required in the future.
In summary, the prevalence of food addiction and the mean symptoms score were high in the FA group compared to other previous studies. Younger aged adults and overweight respondents were more likely to have FA. Intervention studies are required to manage eating behaviours among adults during times of increased stress. This study recommends the need for more longitudinal studies on FA to coincide with the increasing quarantine duration in Jordan and other countries. Moreover, awareness training and programs are recommended to increase the responsiveness toward eating and stress management and its short and long term health effects among adults.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
