
Research Article | DOI: https://doi.org/10.31579/2768-2757/081
Clinic for Pediatric Surgery, Clinical University Center Sarajevo, Bosnia and Herzegovina.
*Corresponding Author: K. Karavdić, Clinic for Pediatric Surgery, Clinical University Center Sarajevo, Bosnia and Herzegovina.
Citation: N. Džiho, K. Karavdić, (2023), Pediatric Cholelithiasis Single Center Experience Results of the Clinic for Pediatric Surgery kcu Sarajevo in Period 2010.-2022. Journal of Clinical Surgery and Research, 4(3); DOI:10.31579/2768-2757/081
Copyright: © 2023, K. Karavdić. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 May 2023 | Accepted: 30 May 2023 | Published: 07 June 2023
Keywords: cholelithiasis; cholecystitis; choledocholithiasis; gallstones; laparoscopic treatment of cholelithiasis; pediatric cholelithiasis; adolescence; hemolytic
Introduction. Cholelithiasis is occurance of one or several gallstones in the gallbladder. It can be complicated with choledocholithiasis, acute or chronic cholecystitis, cholangitis, biliary pancreatitis, biliary ileus, etc. Causes for this disorder in pediatric population can be hemolytic (hereditary spherocytosis, thalassemia, sickle cell anemia) or non hemolytic - other hereditary disorders as cystic fybrosis, Wilson's disease or ileum disordes, total parenteral nutrition, usage of certain medicaments, choledochal cysts, organ transplantation and, in adolescency, those similar to adult patients (obesity). Mostly gallstones found in children are cholesterol ones or pigmented gallstones. There are many diagnostic imaging methods for objectifying gallstones and its complications (as choledocholithiasis that requires ERCP). There is also some differential dyagnoses that should be taken in consideration before the tretment (billary dyskinesion, Odii sphincter dysfunction, neonatal jaundice, cholestasis, pediatric cholecystitis, pediatric pancreatitis and pancreatic pseudocysts as well as pediatric pyelonephritis). First line of treatment of cholelithiasis is with diet, saline infusions and medicaments and if cholelithiasis is symptomatic and/or complicated then cholecystectomy is recomended. Having in mind operative approach it can be open procedure of laparascopic one. Some study show that injuries of bile ducts are more common in laparascopic tretment of pediatric cholelithiasis but nevertheless it is shown that with experienced team and good preparation this is the golden standard in the treatment of pediatric cholelithiasis.
Objectives. Hereby we present a comprehensive review of literature for the clinical presentation, pathophysiology, diagnostic evaluation, and management of cholelithiasis in pediatric population.
Methods. Between 2010. and 2022, retrospectively, we explored data points of children who underwent laparoscopic cholecystectomy reviewed with included demographics properties, indication for cholecystectomy, used surgical technique, operative time, complications, and length of hospital stay. We performed 37 laparoscopic cholecystectomies (due to cholelithiasis and one case of cholecystitis without calculi) with 2 conversions to open procedures and via open approach we treated 3 cholecystes in this period. Male to female distribution was: 12 male patients and 25 female patients
Results. Thirty-seven children (12 male patients and 25 female patients with ages ranging from 7 to 18 years, mean: 11,9 years) underwent laparoscopic cholecystectomy. The indication for surgery was associated to symptomatic cholelithiasis in almost all patients. The surgery was performed under general anesthesia and classical 4-port approach was done in twenty-two patients, and 2-port approach in combination with 2 portless 2.3-mm percutaneous graspers was used in two patients. The operating time ranged between 45 and 120 minutes (mean: 77 minutes). Two patients were treated by open surgery. Only one patient had leakage due to choledocholithiasis, and open surgery and ERCP had to be performed. Median of hospital stay for all patients was 3-4 days.
Conclusion. Laparoscopic cholecystectomy is safe and effective in children, and shows the same advantages reported in adult series.
Cholelithiasis is existence of one or several gallstones in gallbladder or bile ducts [1]. Cholecystitis refers to inflammation of the gallbladder. This disease is much more common within adult population, but due to obesity in adolescence and survival of neonates with short bowel syndrome (due to necrotizing colitis) or need for total parenteral nutrition or some hereditary conditions as spherocytosis, gallstones can also be formed within pediatric population [2, 3,]. Cholelithiasis is occurance of one or several gallstones in the gallbladder. It can be complicated with choledocholithiasis, acute or chronic cholecystitis, cholangitis, biliary pancreatitis, biliary ileus, etc. Causes for this disorder in pediatric population can be hemolytic (hereditary spherocytosis, thalassemia, sickle cell anemia) or non hemolytic - other hereditary disorders as cystic fybrosis, Wilson's disease or ileum disordes, total parenteral nutrition, usage of certain medicaments, choledochal cysts, organ transplantation and, in adolescency, those similar to adult patients (obesity). The pathogenesis of cholelithiasis is similar in adult and pediatric populations. There are two main types of gallstones: cholesterol gallstones and pigmented ones [4]. Causes of cholelithiasis within pediatric population are mostly connected to preexisting conditions as can be divided in: hemolytic, nonhemolytic and idiopathic [5]. 20-40% of the children with cholelithiasis have some kind of hemolytic disease: hereditary spherocytosis, sickle cell anemia and thalassemia are the most common ones and are considered to be the biggest risk factor in the development of symptomatic cholelithiasis in pediatric population [6]. Obesity It is considered that increase of the obesity is one of the main reasons for the increase of cholelithiasis in pediatric population. Obesity as well as sudden weight loss leads to increased bilious secretion of bilirubin [7]. Infants and children younger than 5 years usually have nonspecific symptoms due to the lack of possibility of describing their discomfort [8]. Children aged 2-14 years most often have common bilious colic (50%) or nonspecific abdominal symptoms (25%), nonspecific pain and nausea. Acute abdominal pain due to cholecystitis, cholangitis and pancreatitis is rare in this age group (5-10%) and 20% of those are asymptomatic [9]. Adolescents (14-18 years) have typical bilious colic as adults. Intolerance of fatty food that is typical symptom in adults is present only in adolescents [10]. Diagnostic procedures in pediatric population are similar to those made in adult patients. Diagnosis includes laboratory findings (complete and differential blood count, ALT (alanine transaminase), AST (aspartate aminotransferase), ALP (alkaline phosphatase), total bilirubin, direct and indirect bilirubin, GGT, amylases and lipases and urine evaluation [11]. There are many diagnostic imaging methods for objectifying gallstones. Radiographic methods are X rays, ultrasound that is sensitive, cheap and reliable diagnostic method and bilious scintigraphy, CT, MRI, fluoroscopic cholangiography, ERCP (endoscopic retrograde cholangiopancreatography) where there is a suspicion for obstruction, choledocholithiasis, biopsy of suspicious lesions, obstructive jaundice, cholangitis and bilious pancreatitis [12]. There is also MRCP, ERCP. Open cholecystectomy was golden standard until early 90.s when it is replaced by laparoscopic cholecystectomy that becomes new golden standard in this disease. Carl Langebuch performed first successful cholecystectomy in 1882. and Phillip Mouret, French gyneacologist, performed first laparoscopic cholecystectomy in 1987 [13].
Between 2010. and 2022, retrospectively, we explored data points of children who underwent laparoscopic cholecystectomy reviewed with included demographics properties, indication for cholecystectomy, used surgical technique, operative time, complications, and length of hospital stay.In the present series, all patients were intervened using the 4-port technique (except one that was operated with 3-port tecnique). The pediatric laparoscopic cholecystectomy is completed with dissection of the gallbladder of the liver bed through identification of the Calot’s triangle and subsequent binding of the cystic duct and the cystic artery. However, it should always be kept in mind that the biliary system can vary from patient to patient in the pediatric group just like in the adults. Bile duct injury is a frequently reported complication of cholecystectomy in adult patients. The bile duct and cystic canal junction can be easily observed in children by exposing the presence of stone in the bile duct is another problem. We had one patient 14 years old with acute acalculous cholecystitis that was administred to Intensive care unit due to septic condition or unknown etiology. Inflamatory parameters increased and bilirubin and transaminase were within physiological limits. Abdominal ultrasound showed: „... gallbladder with a wall thickness up to 0,5 cm, filled with dense biliary content with pronounced pericholecystitis edema which diameter is 1,28 cm. Intrahepatic and extrahepatic bile ducts are not dilated. Choledochal duct is 0,49 cm in diameter. Pancreas is appropiate sized and homogenous... “. CT was done (arrow shows nonspecific finding of pericholecystic fluid with no signs of gallstones) and laparoscopic cholecystectomy performed.
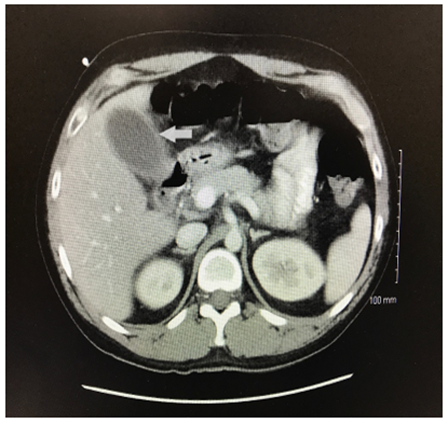
Figure 1: CT in acalculous cholecystitis - arrow shows nonspecific finding of pericholecystic fluid with no.

Figure 2, 3: Acalculosis gangrenous cholecystitis with biliary peritonitis.

Figure 4: Punction of the gallbladder.

Figure 5: Ligation of cytic duct and artery.
During time frame between 2010. and 2022 we operated laprospopically 37 cholecystes (due to cholelithiasis and one case of cholecystitis without calculi) with 2 conversions to open procedures and via open approach we treated 3 cholecystes in this period. Male to female distribution was: 12 male patients and 25 female patients. (Diagram 1)
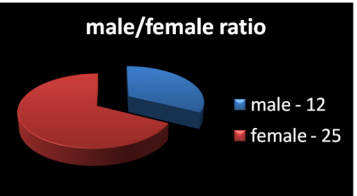
Diagram 1: Gender representation: 25 female and 12 males.
Patients distribution concerning age through years is presented in diagram 2. Most patients in the specified period with cholecystectomy were treated in 2017 (6):
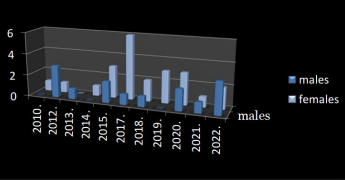
Diagram 2: Patients distribution considerin sex throug years.
Median age concerning distribution in all years was 11,9, and it is presented in diagram 3.
Distribution of patients per age:
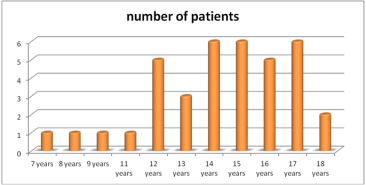
Diagram 3: Distribution of patients per age.
Number of hospitalisation days for patients (table 1) - median of hospital stay for all patients was 3-4 days and stay is shortening as we are closing to the later years as can be seen from the table below:
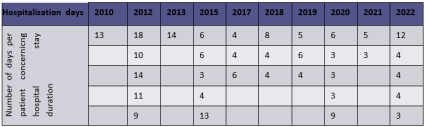
Table 1: Number of hospitalisation days for patients.
Most of patient were chronical cases of cholelithiasis, 3 patients were having acute symptoms and one was acute noncalculosis choleystitis with septic condition who was hospitalized at ICU and operated on our Clinic (diagram 4).
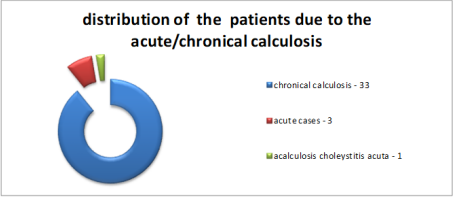
Diagram 4: distribution of the patients due to acute/chronical calculosis.
Procedure time was observed during last three years in 9 patients and median is 77 minutes (diagram 5).
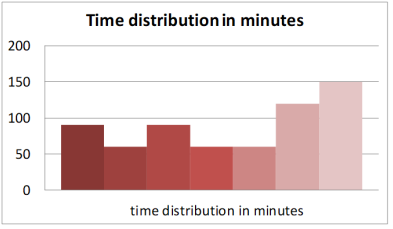
Diagram 5: Duration of the surgical procedure.
Causes of the cholecystectomies is presented on diagram 6. Out of 37 patients, 5 had hereditary spherocytosis (one had open splenectomy a year after laparoscopic cholecystectomy), one patient had sepsis and noncalculosis cholecystitis and other patients were adolescent and therefore had causes like adults:

Diagram 6: Causes of the cholecystectomies.
Drain is extracted between first and fourth postoperative day with median of 1,16 days. In several cases we do not have data about time of the drain extraction (diagram 7).

Diagram 7: Duration of abdominal drainage.
6 patients had obstructive jaundice (one had direct bilirubine 50,6), others (31) did not (diagram 8).
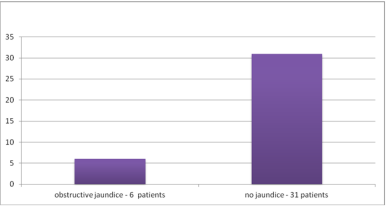
Diagram 8: Existace of obstructive jaundice in patients with cholelithiasis.
Antibiotic therapy
Most of the patients were given antibiotics (not to several patients), 4 were treated on ICU, and of those who were administrated with antibiotics (median of antibiotic usage is 6,5 days) these are the data: (Table 2)

Table 2: Types of antibiotics, number of patients and duration of antibiotic administration.
Boys and girls are equally affected in early childhood, but as in adults, most previous studies reported a female predominance in pediatric gallbladder disease starting from puberty [13,14]. In the study by Wesdrop et al. [15], a female predominance was noted only after the age of 14 years. Kennedy et al [16]. reported equal gender frequency overall. Female gender then increased to 55?ove the age of 12 years, although there was no significant difference in sex distribution. In the present study, we found out of 37 patients 67,5% were female patients whereas 32,4Persentage were boys. Above the age of 10 years, females were predominant (p=0.004). As in adults, this corresponds with the time at which cholesterol saturation in bile increases partly due to the secondary effects detected asymptomatic calcified stones should be intervened through a surgical procedure. 4 of gallbladder stones in our series were symptomatic at the time of administration for operative tretment and we detected only 6 patients who had specific symptoms (jaundice). In our series, the diagnosis was made using ultrasonography for all patients. There are differences between adults and children regarding the cholecystectomy indications and results. While cholecystectomy is frequently performed due to acute inflammation in adults, the main reason for cholecystectomy in pediatric patients without inflammation signs is the prophylactic removal of gallbladder stones [20]. In our study, we operated on only 10,81Persentage of patients in an acute condition, while 89,1Persentage were operated on as a chronic calculous disease. All but one patient had calculous cholecystitis. Since 1987, the year when it was first performed on an adult patient; laparoscopic cholecystectomy has been increasingly used in gallbladder pathologies [21]. In 1991, laparoscopic cholecystectomy was reported to be safe and effective to use in pediatric patients for the first time. (22) After that date, laparoscopic cholecystectomy has become a standard method implemented in children. Laparoscopic cholecystectomy can also be performed through the single-incision laparoscopic surgery technique despite the need for longer time and difficulty of the manipulation of the anatomical structures [23]. The 4-port laparoscopic cholecystectomy is considered as the gold standard for treatment of gallbladder pathology [24]. In the present series, all patients were intervened using the 4-port technique (except one that was operated with 3-port tecnique). The pediatric laparoscopic cholecystectomy is completed with dissection of the gallbladder of the liver bed through identification of the Calot’s triangle and subsequent binding of the cystic duct and the cystic artery. However, it should always be kept in mind that the biliary system can vary from patient to patient in the pediatric group just like in the adults [25]. Bile duct injury is a frequently reported complication of cholecystectomy in adult patients [26]. The bile duct and cystic canal junction can be easily observed in children by exposing the presence of stone in the bile duct is another problem. Although intra-operative cholangiography can be performed in such cases, it is not always a necessity, since this situation is relatively rare. None of our patients needed intra-operative cholangiography during laparoscopy. Postoperative endoscopic retrograde cholangiopancreatography has been suggested to be performed following laparoscopic cholecystectomy in patients in whom such a situation is suspected [27]. If the surgical team encounters difficulties related to previous cholecystitis (e.g., bleeding, perforation of the gallbladder), they may use the alternative of open procedure; however, the open technique was necessary for 1 of our patients [28].
There are certain specifities in diagnose and treatment in pediatric population when it comes to cholelithiasis that should be taken in consideration. Children (if not adolescent who usualy have same causes for cholelitiasis as adults) can have cholelithiasis due to hereditary hemolytic and non hemolytis diseases, medicaments as well as ceftriaxone and total parenteral nutrition due to existance of ICU where babies who reqire this tretment now can survive and need this kind of tretment if it is not a case of transient chollithiasis. Pediatric cholelithiasis is more prone to complications in some cases so its presentation can occur with complication symptoms. Unlike in adults where cholelithiasis is not recomended to be treted immediately, in pediatric population cholelithiasis should be treated when it is diagnosed due to possible and often complications. When it comes to treatment although there are some studies that show that in pediatric population injuries of bile ducts are in higher percentage when it comes to pediatric laparoscopy, this method of treatment is golden standard for tretment of pediatric cholelithiasis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
