
Case-Report | DOI: https://doi.org/10.31579/2641-0419/059
*Corresponding Author: Hieu T. Huynh, Mount Sinai Morningside Hospital Al-Sabah Arrhythmia Institute 440 W 114th St, New York, NY 10025
Citation: Huynh H., Siroky G., Bisht D., Lam P., Mohammad A., Mehta D., (2020) Partial Fracture of a Subcutaneous ICD Lead from Mechanical Trauma. J. Clinical Cardiology and Cardiovascular Interventions, 3(6); Doi:10.31579/2641-0419/059
Copyright: © 2020 Hieu T. Huynh, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 March 2020 | Accepted: 16 April 2020 | Published: 23 April 2020
Keywords: subcutaneous ICD; lead fracture; electrode failure
Transvenous implantable cardioverter-defibrillators (TV-ICD) have electrode failure rates as high as 20% over a 10 year followup with 12% as a result of lead fractures. [1] The development of the Boston Scientific subcutaneous ICD (S-ICD) promoted the benefit of significantly reduced post-implant complication rates. [4] We present the first reported case of a S-ICD electrode failure secondary to partial fracture as a result of mechanical trauma.
Implantable cardioverter defibrillators (ICD) are life saving devices that monitor and treat fatal ventricular arrhythmias. Indications for an ICD broadly include a secondary prevention population who have survived prior cardiac arrest, sustained VT/VF, or syncope caused by ventricular arrhythmia and a primary prevention population who are at an increased risk of fatal ventricular arrhythmias.[2] ICD technology has progressed since first developed by Dr. Mirowsky. The development of the subcutaneous ICD system allowed for the implantation of an ICD system without the need for placement of the ICD lead transvenously with the traditional transvenous ICD (TV-ICD) systems. S-ICDs bypassess the TV-ICD complications which include lead dislodgement, lead fracture, externalization, embolization, insulation break, and tricuspid valve damage.[5] S-ICD systems are safe and effective. S-ICDs are recommended for patients who meet criteria for a TV-ICD but do not have vascular access or at high risk of infection. [2,3]Boston Scientific’s Emblem S-ICD has very low post implant complication rates, which is limited to localized infection or hematoma. [4] Recently, there was a single case report of electrode failure due to cable externalization. [6]
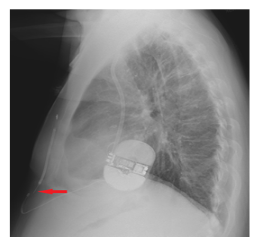
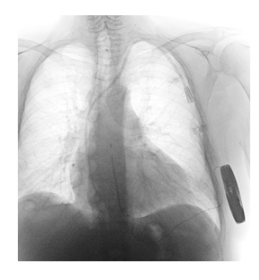
A 54 year old male with a past medical history of ischemic cardiomyopathy and heart failure with reduced ejection fraction (HFrEF) of 15% who was implanted with a Boston Scientific Emblem S-ICD for primary prevention after his initial TV-ICD was explanted due to a lead infection. The patient arrived at the emergency department status post a mechanical fall and was discharged on the same day. The patient’s home monitoring system notified us that the impedance of his defibrillation electrode was greater than 400 ohms, suggesting a lead fracture. A two view chest x-ray confirmed that the S-ICD lead fracture proximal to the defibrillation coil (Figure 1 and Figure 2). This fracture is most evident on the lateral view chest x-ray (Figure 1).
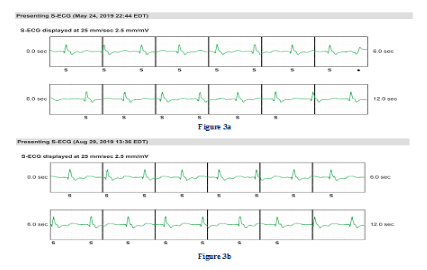
The sensing component of the lead remained intact as shown in (Figure 3a and 3b). Comparing the electrogram before and after the chest trauma shows no change.
During lead extraction, the S-ICD was severed completely and removed in two pieces with manual traction at the most proximal end of the lead. A new S-ICD lead was then successfully re-implanted.

Transvenous ICD/pacemaker lead fractures are a known complication secondary to chronic tension and stress from repetitive cardiac and thoracic movement, subclavian crush, twiddler syndrome, thoracic trauma, thoracic outlet syndrome and multiple other etiologies.[7-9] Post operative S-ICD implant complication rates are low and generally limited to localized infection and hematoma.[4] To date, there has only been a single case report of an S-ICD lead externalization demonstrating potential lead complications, however, there has not been any reported cases of a S-ICD lead fracture.
This case demonstrates that S-ICD leads are in fact susceptible to fracture. Direct mechanical trauma to the chest was the most likely cause of lead fracture and associated stretching of the lead from the fall likely contributed to the fracture asit occurred just beyond the retaining suture. As the sensing function was still intact, there was a selective fracture of the defibrillator coil. This case also illustrates the importance of home monitoring. The patient was unaware of damage sustained to the S-ICD lead from the fall which could have led to failure of appropriate defibrillation therapy in the future.
Complications related to S-ICD implantation have been limited to localized infection and hematoma. We report the first known case of a partially fractured S-ICD lead secondary to mechanical trauma confirmed with a two view chest x-ray and elevated impedance (>400 ohms) readings on the patient’s home monitoring system.
Hieu Huynh D.O.: None
Gregory P. Siroky M.D.: None
Devendra Bisht M.D.: None
Patrick Lam M.D.: None
Asad Mohammad D.O.: None
Devendra Mehta M.D. Ph.D.: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
