
Case Report | DOI: https://doi.org/10.31579/2768-2757/020
*Corresponding Author: Georgina David Dhalwale, Behind Hotel Suman, Balaji nagar, Sakri road, Dhule, India.
Citation: Georgina D Dhalwale. (2021). Ossification of Non-vascularized Free-Fibula Graft for Mandibular Reconstruction after Resection of Ameloblastoma: Review of Literature and Presentation of 2 cases. Journal of Clinical Surgery and Research. 2(4); DOI: 10.31579/2768-2757/020
Copyright: ©2021 Georgina David Dhalwale, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 June 2021 | Accepted: 30 July 2021 | Published: 09 August 2021
Keywords: ameloblastoma; maxillofacial surgery; fibula graft; reconstruction; mandibular resection; surgery
Introduction: Ameloblastoma is a benign neoplasm of odontogenic epithelial origin occurring more commonly in the mandibular posterior region and rarely in the maxilla. About 50-60% of ameloblastomas occur in the mandibular ramus area, while only 10% is seen in mandibular anterior region. Ameloblastomas are slow growing, locally invasive, rarely malignant tumours affecting the jaw. Mostly commonly seen in the 4th-6th decade of life affecting males more commonly than females. The resection of the mandibular segment without adequate reconstruction leads to functional as well as esthetic loss.
Case Report: Here we describe two case reports of ameloblastoma with segmental resection and reconstruction using fibula graft.
Discussion & Review of Literature: Avascular fibula graft with its high bone density, ease of access to harvest, and tendency to show less resorption helps to achieve satisfactory esthetic contour and function in reconstruction of segmental defects of mandible
Conclusion: This article describes two case reports of ameloblastoma with segmental resection and reconstruction using fibula graft along with review of literature.
Ameloblastoma is a neoplasm of odontogenic epithelium of enamel organ‑type tissue that has not undergone differentiation to the point of hard tissue formation [11, 18, 25]. Ameloblastomas are rare, benign tumors, representing 1% of the oral tumors and cysts. (13) It is locally invasive with high chances of recurrence [1, 8, 9, 18]. According to WHO 1992, ameloblastoma is defined as, “a benign but locally invasive polymorphic neoplasm consisting of proliferating odontogenic epithelium, which usually has a follicular or plexiform pattern, lying in a fibrous stroma” [4, 5, 6, 8]. Clinically, ameloblastoma is often asymptomatic and slow growing. Ameloblastoma can cause the onset of symptoms such as swelling, dental malocclusion, pain, paraesthesia and anesthesia of the affected region, facial asymmetry, and displacement of teeth and pathological fracture [1, 2, 8, 9, 10]. Surgical management is the measure of treatment of ameloblastomas. It has been proposed that treatment options should be based on clinical signs and symptoms. It has been suggested that conservative measures for peripheral and unicystic ameloblastoma and a more radical approach of management for the multicystic subtype should be undertaken [3, 14]. Treatment by wide excision is curative in up to 95% of cases [26]. Chana et al. proposed a 1 to 2 cm normal margin, and the large defect left after resection guarantees reconstruction preferably with the free fibula graft [1]. In 1989, the first mandibular reconstruction with a fibular flap, using osteotomies to imitate the shape of the mandible, was described [7]. Non-vascularised bone graft with implants provide good contour and aesthetics but are most successful in non-irradiated patients who have adequate soft tissue and where the defect is minimal. Factors like need for skilled professionals and equipment, increased intra-operative time, post-operative period, economic reasons, increased age and compromised medical condition of the patient are against vascular grafting. Thus non-vascularised bone grafts are a viable option for mandibular reconstruction. It can be used for primary reconstruction of mandibular defects due to benign pathologies [27]. Further functional rehabilitation with implants and removable prosthesis can also be done after 6 weeks of reconstruction [12].
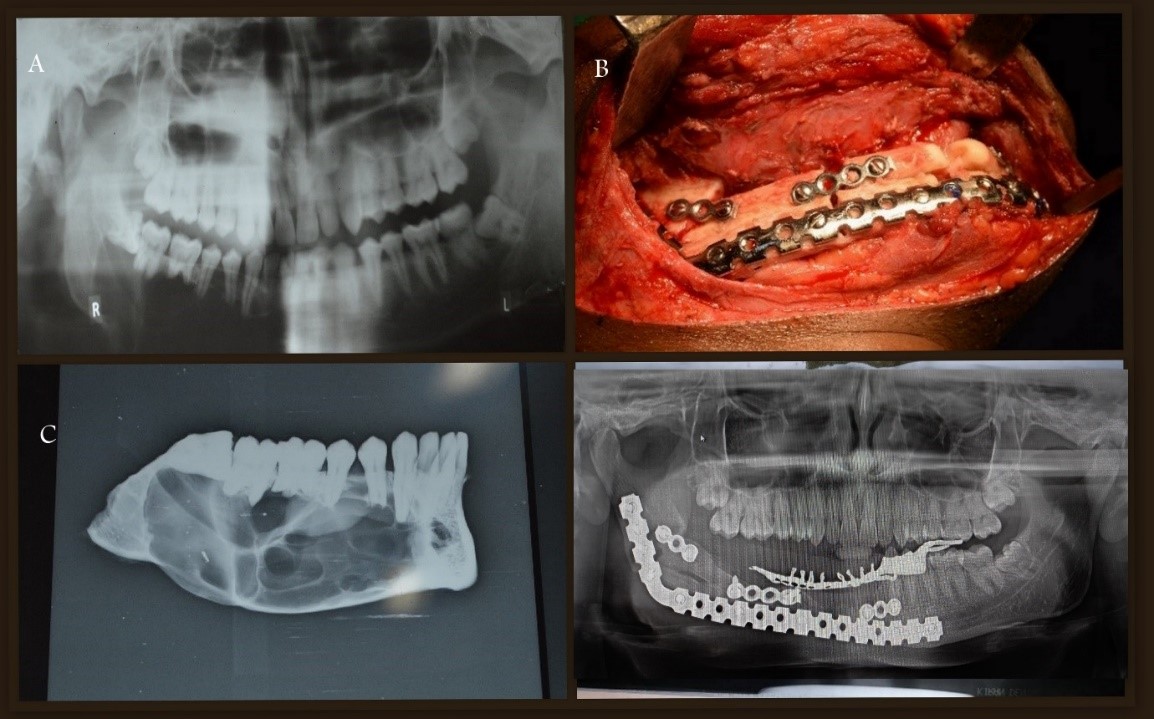
A 25 year old female patient, visited our institute with a complaint of pain and swelling in the lower right back region of the jaw since 4-5 months. On extra-oral clinical examination, a single round to oval, ill-defined swelling approximately 5x4 cm in dimension over the right angle and ramus region was noticed. The swelling was hard to firm in consistency, tender on palpation. On intra-oral examination, a single ulcerative lesion of dimension 2x2 cm was seen in the lower right back region of the jaw in the retro-molar triangle region, which was tender on palpation. Incisional biopsy report was suggestive of Plexiform Ameloblastoma. Wide local excision of the lesion with segmental mandibular resection and reconstruction with free fibula graft was done on the right side. (Fig. 1A, 1B, 1C, 1D) Weight bearing on the donor leg was allowed 1 week post-operatively. Regular follow up was done to ensure the uptake of fibula graft. (Fig. 1E).


A 21 year old male patient, visited our institute with a complaint of swelling in the lower right back region of the jaw since 2 months. On extra-oral clinical examination, a single round to oval, ill-defined swelling approximately 5x3 cm in dimension over the right lower border of the mandible was noticed. The swelling was hard to firm in consistency and non-tender on palpation. On intra-oral examination, a single, round to oval, diffused swelling of dimension 4x3 cm approximately was seen extending from the canine to the second molar on right side, vestibule was obliterated and non-tender on palpation. Incisional biopsy report was suggestive of Ameloblastoma. Wide local excision of the lesion with segmental resection and reconstruction with free fibula graft was done on the right side. (Fig. 2A, 2B, 2C, 2D) Weight bearing on the donor leg was allowed 1 week post-operatively. Regular follow up was taken over a period of 2 years. (Fig. 2D, 3A).

Ameloblastoma or admantinoma, according to World Health Organization (WHO) (1991) defined as a benign but locally aggressive tumor with a high tendency to recur, consisting of proliferating odontogenic epithelium lying in a fibrous stroma. Robinson in 1997, defined ameloblastoma as “a tumour that is usually unicentric, non-functional, intermittent in growth, anatomically benign, clinically persistent”. It was described in 1827 by Cusack and was initially known as adamantioma in 1885 by the French physician Louis-Charles Malassez. It was renamed as ameloblastoma in 1930 by Ivey and Churchill [2, 18, 23]. The clinical signs & symptoms of ameloblastoma in mandible include swelling, malocclusion, pain, paraesthesia, and anesthesia of the affected region, but most of the patients are asymptomatic unless infection leads to pain and are diagnosed during routine plain radiographic films. Therefore, most of the patients are diagnosed late when the mass has grown to an extent that it is clinically evident. When planning the treatment of ameloblastoma, it is important to recognise the growth characteristics and to remove the full extent of the tumor, including the surrounding tissues [2]. Patients with ameloblastoma can be treated in a number of different ways. The best treatment modality is still controversial. Ameloblastomas tend to infiltrate bone trabecula of the cancellous bone on the lesion’s periphery and expand through the medullary cortex, before a true bone resorption becomes radiologically evident. Therefore, the true tumor margin goes beyond the clinical or radiographic margin [15]. Conservative treatments for ameloblastoma have lower success rate and chances of local recurrences are high. Segmental resection of the mandible is the current treatment of choice for ameloblastoma. Resection with safety margins of up to 1 cm and immediate reconstruction in the same operating time can provide low recurrence rate, good oral function, and high quality of life [2]. Shirani et al [2007] in a series of 7 patients introduced a technique of removal of large ameloblastoma with immediate reconstruction [16]. Immediate reconstruction is especially significant because unobliterated dead space can accumulate fluids in the operated site that may cause secondary infection leading to un-esthetic appearance and difficulties in mastication, swallowing and speaking. It is concluded that there are less chances of infection, scarring and morbidity with immediate reconstruction procedures following resection. Both the patients in our report were treated with segmental resection, one with disarticulation and one without disarticulation, followed by immediate reconstruction. Also in our cases revascularization of the graft was seen which is not seen often with cases of fibula reconstruction. It is very rare for a non-vascularized graft to be readily accepted, to see revascularization happen and graft being taken up by the bone is remarkable in such cases which can avoid further resorption of bone. Eppley [2002] did a series of 60 mandibular ameloblastoma cases which showed that there was no recurrence of those cases treated via en bloc resection as compared to enucleation and curettage in which the recurrence rate was high. There are different methods of mandibular reconstruction [16]. Pogrel’s comparison study of vascularised and nonvascularised fibula for mandibular reconstruction suggested that any defect <9 cm with adequate soft tissue closure can be successfully reconstructed by means of avascular graft [22]. The ideal flap for such a defect must provide adequate bone length, thickness, and width which should be similar to the mandible, for reconstruction of the bone component of the defect and allowing osseointegration [2]. The various sources for non-vascularized bone graft include iliac crest, fibula, calvarium, rib and tibia [12]. The healing process of non-vascularised bone grafts is by creeping substitution. The graft acts as supporting structure and is replaced by new bone arising by the process of osteoconduction and osteoinduction after resorption of the matrix [17]. Fibula is situated posteriolateral to tibia, with its tubular structure being similar to mandible, dense cortical plates, and presence of endosteal blood supply allows for multiple graft osteotomies to contour without compromising the bone. Availability of 20–25 cm of bone for harvest and least donor site morbidity makes it an ideal choice for reconstruction of such defects. Since it is not the prime weight bearing bone, its removal does not affect the function of the leg. Thus avascular fibula graft is the reconstruction choice for segmental defects of mandible [12, 24]. In our report, in both the patients fibula graft was taken for reconstruction of the mandibular defect and regular follow up was done to check the gait of the patient which was unaffected. Graft was readily accepted by the bone without any complications. (Refer Fig. 1E, 2D). Graft union was defined as bony trabeculae bridging between three and four cortices on both the proximal and distal junctions of the autograft with the host bone on radiographs. If union or bony bridging occurred at only one site, it was considered as a nonunion. Long-term post-operative radiograph monitoring was done to evaluate graft union on all patients. Grafts were evaluated to have nonunion if no radiographic bony trabeculae would have crossed the bone junctions on both ends on latest follow-up [28]. The main advantages of fibula grafts are quicker graft harvest with less blood loss, enough length of fibular bone segment for any length of mandibular defect. Disadvantages of fibula are the straightness of the bone, necessitating osteotomies for curvature, which increase the operating time. The common recipient-site complications are dehiscence of intra oral wound due to underlying bony defect [12, 17]. None of our patients showed any complications with respect to the graft. Thus avascular fibula graft with its high bone density, ease of access to harvest, and tendency to show less resorption helps to achieve satisfactory esthetic contour and function in reconstruction of segmental defects of mandible [17]. Vayvada et al. reported no recurrence in any of his 11 patients undergoing segmental resection and fibula reconstruction with a mean follow up of 29.3 months [20]. Chaine et al. reported similar results where none of his 44 patients had any recurrence with a mean follow up of 53 months [21, 19]. We have treated 2 cases by resection and fibula reconstruction and have not observed any case of recurrence.
It is a good choice to reconstruct mandibular defect with non-vascularised free fibula bone graft to get a better contour and function. The non-vascularised free fibula graft provides a good alternative to other bone grafts for mandible reconstruction. The main aim of this paper was to highlight the union of non-vascularized fibula graft with the adjacent bone. It is a good choice to reconstruct mandibular defect with free fibula bone graft to get a better contour.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
