
Research | DOI: https://doi.org/10.31579/2637-8914/065
1 Department of Food Science and Technology, Faculty of Natural Resources and Environmental Studies, University of Kordofan, P.O. Box.160, Elobeid, Sudan.
2 Department of Food Science and Technology. Faculty of Natural Resources and Environmental Studies. University of Alsalam, Alfulah, Sudan.
*Corresponding Author: Ahmed, Adam Ismail, Department of Food Science and Technology, Faculty of Natural Resources and Environmental Studies, University of Kordofan, P.O. Box.160, Elobeid, Sudan.
Citation: Ahmed A. Ismail and Abdelgader F.R. Eltaieb. (2021). Nutritional Status of Children with Severe Malnutrition in Elnohoud Educational Hospital in West Kordofan State, Sudan. J. Nutrition and Food Processing, 4(7); DOI:10.31579/2637-8914/065
Copyright: © 2021, Ahmed, Adam Ismail. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 July 2021 | Accepted: 15 October 2021 | Published: 26 October 2021
Keywords: nutritional status; Kordofan region; severe malnutrition; WHO; child malnutrition
The present work was conducted in Elnohoud educational hospital, West Kordofan State, Sudan during the period from 2015 – 2017. The aim of the study was to identify the nutritional status among children less than five years of age. Study included 100 children. Data were collected using a structural interview questionnaire, then analyzed via the Statistical Package for Social Sciences (SPSS) software version 16. The results indicated that the majority of patients (73%) in age group of 13-24 months, and their resident in rural areas (94%) and belonged to large families' more than six family members (56%), also the birth spacing were 74% less than one year and 26% were more than one year. 84% of the mothers were housewives, while 70% of fathers were farmers and workers. and 71% of mothers were more than 24 years old. 70% of the malnourished children received insufficient breastfeeding mainly due to pregnancy or mother's illness. Nearly (89%) were introduced to supplementary food with breastfeeding before 6 months, and (75%) of surveyed received less than three meals/day of unbalanced inferior quality foods (88%). Additionally 66% of studied children used the traditional treatments such as razor cut, fire and hilba for diseases control. Also 58% of the studied children had cases of sickness previously admittance to hospital two times. A cause of nutritional status of Children with severe malnutrition problems in another places of Kordofan regions rather than Elnuhoud educational hospital need to be elaborated in future work as recommended point of view.
Child malnutrition is internationally recognized as an important public health indicator for monitoring nutritional status and health of population. The devastating effects of malnutrition on human performance, health, and survival well established today [15]. WHO global analysis demonstrated that child malnutrition is the leading causes of the global burden of diseases [13]. As a result of the increased recognition of the relevance of nutrition as a basic pillar for social and economic development, monitoring trends in childhood malnutrition has gained increasing importance in assessing the progress (Ahmed, 1991), so the objective of the present investigation to assess nutritional statues among children with severe malnutrition in Elnohood Educational Hospital, West Kordofan state, Sudan.
Study area: The study was conducted in Elnohood Educational Hospital, West Kordofan State, Sudan, using a cross sectional interventional prospective descriptive hospital based designed.
Sampling techniques: The sampling was done according to random sampling technique which used for the selection of children.
Inclusion criteria: all children of age below 5 years admitted as severe malnutrition and fulfilling the WHO criteria of severe wasting or edematous malnutrition in the hospital.
Exclusion criteria: more than 5 years old children and parental refusal to participate in the study.
The study includes 100 children under five year's age with severe malnutrition.
Data collection: A questionnaire was designed to contain full information about the nutritional status.
Statistical analysis: Data was analyzed by using Statistical package for the social sciences (SPSS) software version 16. Descriptive statistics as qualitative analysis (percentage, frequency).
Age of the malnourished children:
The results indicated that most of malnourished children 73% within the age group of 13-24momths, while 22% were more than 24-59 months, however only 5% less than 12 months (Figure 1). It is clear that the majority of children suffering from malnutrition were under three years old, the present findings were in agreement with WHO (1986) which stated that the risk of malnutrition is high at the age of 6-48 months. Similarly, Ahmed (1991) and Babiker (1994) found that the majority of malnutrition causes in Sudan occur in the age of 6-24 months. Basit, et al. (2002) reported that about 82% of the malnourished children aged one to five years in India were of 1-3 years old, while 18% their age ranged between 3 to 5 years. Also Nabag et al.(2013) reported that 63.3% of children under five years age in Omdurman pediatric hospital, Sudan their ages were ranged from one to two years, 17% were less than one year and 20% were 2 to 5 years old.

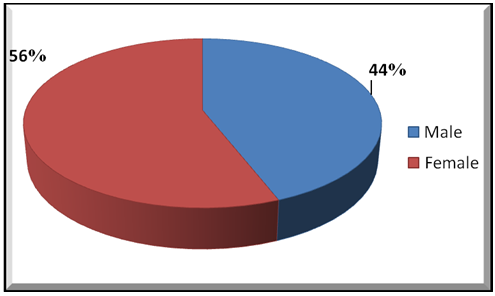
Gender of the malnourished children:
The respondents were found to be consisted of 44% males and 56 percentage of females (Figure 2). Similarly, Basit et al. (2002) reported that 48% of the malnourished in children aged from one to 5 years in India were males and 52 percentage of females. Almost the same findings were reported by Ahmed et al. (2011) who gave 44% and 56% for males and female, respectively.
Residential of malnourished children:
About 94% of the malnourished children under investigation (Figure 3), were rural residents, while 6% were from urban areas, Nabag et al. (2013) who reported 67% from rural areas and 33% from urban areas in Omdurman Pediatric Hospital, his findings enhanced the prevalence of malnutrition among rural area rather than urban population. UNICEF (1997) reported that PEM is prevalence among young children in Sudan especially in rural areas of North Kordofan state and Darfur Region. In Assuite, Egypt, 93% of the malnourished children were from rural areas, while only 7% were from urban places [1].

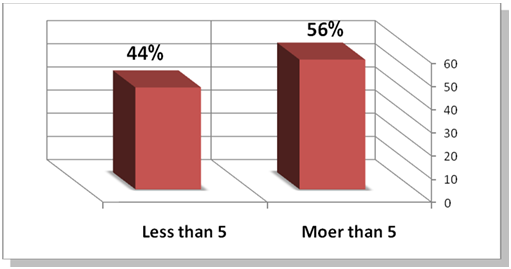
Family size of malnourished children:
The results revealed that 56% of children suffering malnutrition belonged to families of more than 5 children, while the rest respondents 44% were from families less than 5 children (Figure 4). This findings corresponding with Nabag et al. (2013) who showed that 58% of respondents in Omdurman Pediatric Hospital, Sudan had 5-6 children and 42% have less than 4 children.
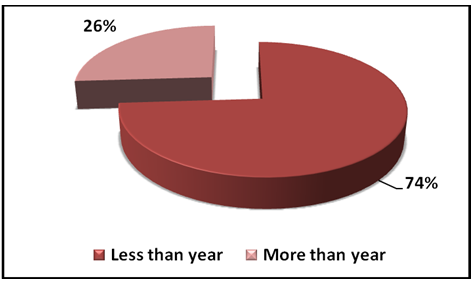
Birth spacing: The birth spacing between the malnourished children was as follows: 74% less than one year and 26% more than one year (Figure 5). It is well know that short interval between successive children may increase their risks of malnutrition and even dying, moreover pregnancies which were numerous and too narrowly spaced may be harmful for both mother and the child [6]. Therefore, the space between successive births should be at least two years [11]. In contrast Basit et al. (2012) found that the interval between births of two siblings in India was less than 2 years (55%) and 2 years or more (45%).
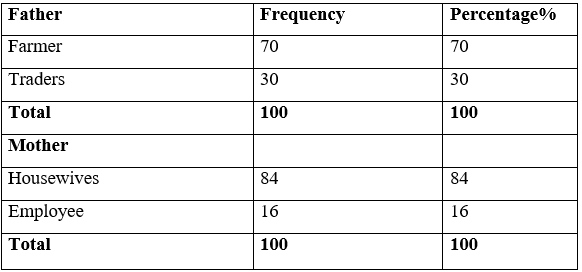
Mother's occupation of malnourished children:
The results revealed that 84% of respondents were housewives, while 16% were employees (table 1). Previously Ahmed et al. (2011) mentioned that mothers of malnourished children in Assuit, Egypt were housewives (95%), while the working mothers constituted only (5%). Nabag et al. (2013) stated that the majority of mother's malnourished children in Omdurman pediatric hospital, Sudan were housewives (78%), whereas the working mothers comprised only (22%). Conversely Ower et al. (2000) found that most of mothers of malnourished children in Kampala, Uganda were unemployed (85%), while traders and professional were (9%) and (6%), respectively.
Father's occupation of malnourished children: Most of fathers 70% were traditional farmers and labors workers (table 1), while the remaining fathers were traders 30%. Slightly different from the findings of Nabag et al. (2013) who found that the father occupation showed that 58% not professionals and 42% professional. Basit et al. (2012) reported that father’s occupation of the malnourished children in Udupi Taluk of Karnataka, India was professionals skilled (68%) and laborers/unemployed (32%).
Breastfeeding of malnourished children: The present study showed that all malnourished children investigated were breastfed, 70%received insufficient and 30% received sufficient breastfeeding (table 2). However, 46% of the malnourished children in Omdurman pediatric hospital, Sudan were on breastfeeding, while 54% were not completed breastfeeding [7]. While only 23% of severely malnourished children in Kampala, Uganda, less than 2 years were still breastfed. The high percentage of breastfed children might indicate that the majority of the mothers had information about the benefits of breastfeeding. WHO (2009) Mentioned that breast milk alone satisfy the nutritional needs for baby for six months of age.
Weaning of malnourished children: The results revealed that only 29% of investigated children were breastfed i.e. not weaned (table 2). On contrary, the majority 71% experienced early and suddenly weaning. Similarly, more than half (57%) of the patients in Bushbuckridge district-Limpopo province, South Africa were weaned early (Saloojee et al., 2007).In the Muslims world, especially in Africa and Sudan, most families obey teaching of Quran which advise weaning by two years of age. It is well known that breastfeeding for two years or long helps a child to develop and grow strong and healthy [13].

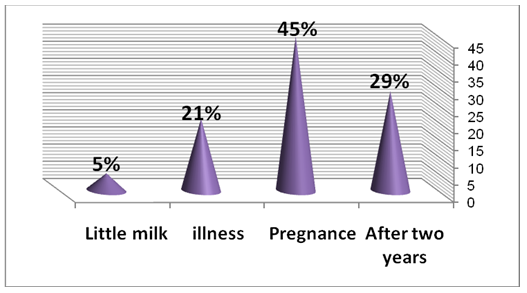
Cause of stopping breastfeeding of malnourished children:
The main reasons of stopping breastfeeding were a new pregnancy 45 %( Figure 6), there is a widespread misbelieves among mothers that during pregnancy breastfeeding harmful to the child, mothers thought that breastfeeding at the beginning of another pregnancy affected the mother health, about 21% mothers stopped breastfeeding because they were sick, while 5% were due to little milk. However Passmore (1980) reported the same reasons for cessation of breastfeeding among poor uneducated women in Malawi. Stopping breastfeeding due to mother's illness is significant risk factors for PEM [9]. However reasons behind stopping breastfeeding in Bushbuckridge District-Limpopo province, South Africa were child illness, mothers becoming pregnant, ill leaving or dying and the fear of HIV transmission [9].
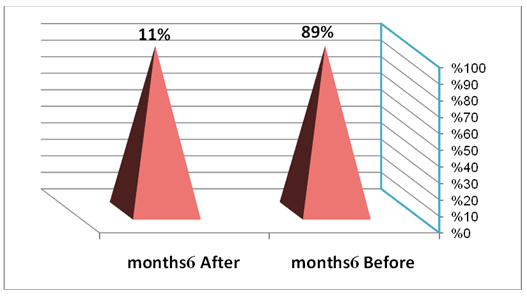
Supplementary food of malnourished children:
The majority of the respondents (89%) were introduced to supplementary food with breastfeeding before 6 months, while 11% had supplementary food after 6 months (Figure 7). In previous investigations implemented in Sudan reported by Nabag et al. (2013) only 20% of the malnourished children had additional and adult foods, more than half of mothers start additional food from 8<12>
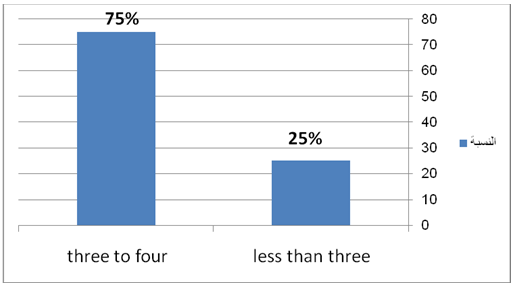
Number of meals per day for children under investigation (75%) received less than 3 additional meals per day, while 25% received 3 to 4 meals per day (Figure 8). However, WHO (2002) recommended that other foods to be given 2-4 times a day for the age of 7 to 12 months and 5 times a day for the age of 12 to 24 months.
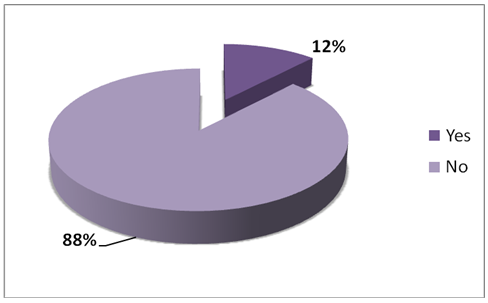
Quality of supplementary food of malnourished children:
Regarding the quality of the added foods (Figure 9), 88% of respondents acclaimed that their received bad quality food or not given food, on the other hand only 12% of the respondents received good quality and verity food. Michael (1997) stated that some mothers were not aware with infant and the child is supposed to share family meals. Since the family meal is served only twice or three times a day simply cannot eat sufficient amount of food to cover their needs, beside the family meal is too bulky and does not have concentration of proteins, vitamins and minerals needed and it is often too difficult to be digested. Ahmed et al. (2011) Mentioned that only 6% of the malnourished children in Assuit, Egypt received balanced additional foods.
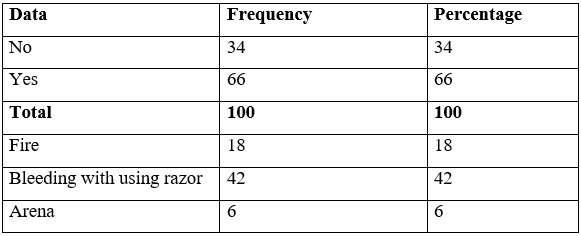
Traditional treatment of malnourished children:
The result revealed that 66% of the mothers used the traditional treatments and (42%) of them bleeding with using razor cut, while (18%) used fire only (6%) were arena (hilba), whereas respondent (34%) not used these traditional treatments(table 3), mothers argued that using traditional treatment lead to control and treat some diseases such as diarrhea, teething and others. In Uganda, some tribes at Western Uganda using traditional treatments, for children under 5 years of age, that have been one of the main causes of malnutrition in children of those region and tribe [5].
Previous children sickness of malnourished children:
The results indicated that 58% of the studied children had previous causes sickness admission at hospital two times (46% due to diarrhea and 12% due to malaria), but 42% were not have diseases (Figure 10). The diarrhea is considered as a great risk leading to occurrence of malnutrition. Many studies showed that gastrointestinal infections especially diarrhea were very important in incidences of PEM [6].

The statistical analysis revealed that there were correlation found between risk factors causes to prevalence of PEM, quality supplementary foods, traditional treatments and mother's occupation. Efforts dealing with child malnutrition issues must focus on factors associated with development outcomes such as mother's income, education and creation of employment as well as rising mother's awareness to risk factors related to PEM.
Counseling mothers about hazards by using traditional treatments, safe and nutritious food as well as appropriate amount of food and snack intake for children, encouragement the mothers improve complementary breastfeeding in first six months from birth, also introduced quality supplementary food after six months of child age.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
