
Research Article | DOI: https://doi.org/10.31579/2768-2757/016
*Corresponding Author: Brenda Arcos Vera, Third-year Resident Surgeon of the Plastic Surgery service and Reconstructive of the Central Military Hospital, CdMx.
Citation: Brenda A Vera, F A L Silva, H A M Yépez. (2021) Management and Treatment of Wounds by Projectile from a Firearm in Hand in the Plastic and Reconstructive Surgery Service of the Central Military Hospital in Two Years. Journal of Clinical Surgery and Research. 2(3); DOI: 10.31579/2768-2757/016
Copyright: ©2021 Brenda Arcos Vera, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 May 2021 | Accepted: 25 June 2021 | Published: 28 June 2021
Keywords: gunshot wounds
Introduction: Gunshot wounds are a major cause of morbidity and lead to serious socioeconomic problems. Wounds often causing severe functional sequelae. Therefore, it is vitally important to provide proper management of these wounds.
OBJECTIVES: Define the treatment of gunshot wounds at the Central Military Hospital in the period from March 2019 to March 2021.
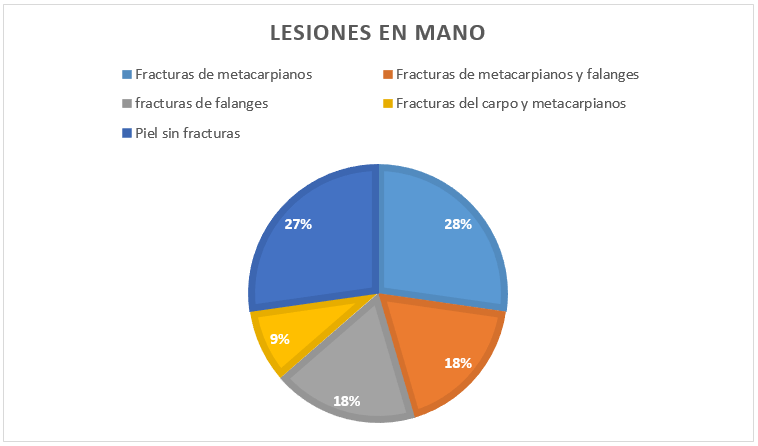
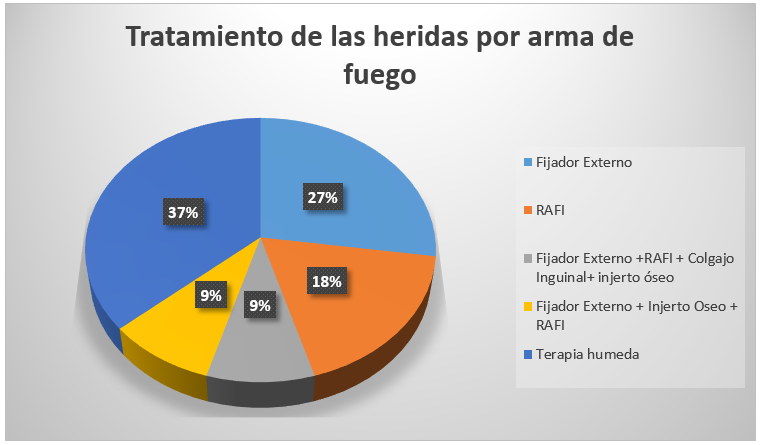
Material and Methods: It is a descriptive, retrospective, observational study, RESULTS: Patients who fulfilled the diagnosis presented 3 metacarpal fractures (27.27%), 2 metacarpal and phalangeal fractures (18.18%), 2 fractures of phalanges (18.18%), 1 carpal + metacarpal fractures (9.09%), 3 with injury only to skin cell tissue without evidence of fractures (27.27%). Therapeutic management: 3 patients received external fixator, 2 ORIF, 1 external fixator + ORIF + inguinal flap + bone graft, 1 external fixator + bone graft + ORIF, 0 wound closure, 4 management with wet therapy, CONCLUSIONS: The wounds By firearm in hand are frequent injuries, which merit immediate treatment. This depends on the complexity of the injury for a speedy recovery and integration into the workplace.
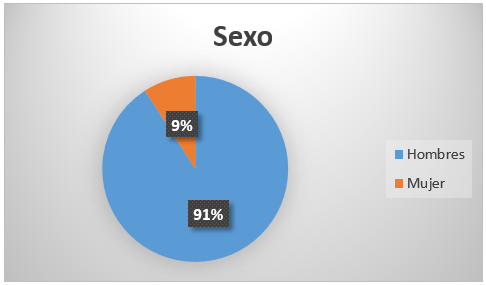
To date, gunshot wounds (HPAF) constitute a public health problem in the world. This fact is influenced by multiple factors such as: family disintegration, unemployment, early incorporation into criminal groups, experiences with drugs, uncontrolled dissemination of violent acts through the mass media, as well as greater ease in acquiring weapons [1]. In Each year in the United States, 30,000 to 50,000 people die secondary to HPAF, and they constitute the first cause of death in the first 2 decades of life; furthermore, it is estimated that for each death there are at least 3 disabling injuries. With regard to homicide, it mainly affects men; the most affected age range being 15 to 34 years [1, 2].
In Mexico, it is evident that the frequency of these injuries has increased [2]. In the last 15 years, injuries from this type of projectile have increased significantly; causing damage through tissue disruption, hemorrhage and infectious processes. These types of wounds are often contaminated with foreign materials such as cloth, dirt, stones, bullets, and splinters [3]. It is therefore important to promptly manage these injuries.
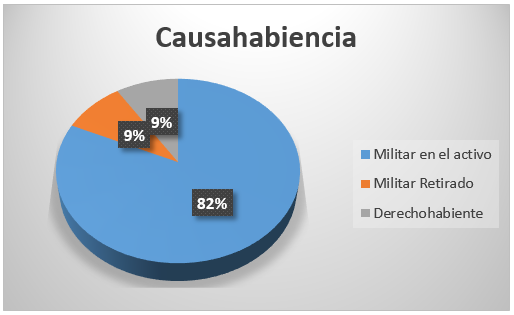
The Central Military Hospital receives both civilian patients who suffer assaults on public roads and active military patients who suffer assaults due to assaults and during confrontations against armed groups.2 Due to the use of means of protection in the thorax and head, the extremities are areas vulnerable to projectiles and explosions. These are affected with a frequency of 60-80%, and the hand in particular in about 25%, 4 being these infrequent sites. The injuries are generally caused by low speed missiles (pistols), tending to cause complex injuries to the upper extremities6, causing prolonged or permanent disabilities with a personal, social and economic impact on young adults and different degrees of severity [7].
In firearms injuries, three components can be distinguished: entry port, trajectory, and exit site [10].
Corresponds to a smaller contused wound; among its characteristics are the carbonaceous halo (false tattoo or smoking) which corresponds fundamentally to the deposit of the elements of deflagration of the gunpowder around the entrance orifice. The flash from the muzzle will cause a burn, so a period of observation is required. If it is an area where the skin is on a bone plane, the following characteristics may be present: Hoffman lesion, stellate lesion, Benassi sign and impression of the cannon on the skin. The "quarter mine" or Hoffman lesion corresponds to a pocket between the skin and the bone; produced by the sudden expansion of the jet of compressed gas after the shot.
During its intracorporeal trajectory, the projectile releases kinetic energy towards the surrounding tissues perpendicular to its trajectory, generating a shock wave that, due to their elasticity, produces a space called "temporary cavity"; but if the shock wave exceeds the resistance of the tissues, they rupture, generating a definitive cavity greater than the diameter of the projectile. If an easily accessible projectile is found, it must be removed.
It is formed by the pressure exerted by the projectile from the inside out, everting the skin, the exit orifice tends to be larger and more irregular than the entrance orifice, giving the appearance of having exploded outwards due to the energy they release [8, 10].
In the context of wound ballistics, these have 2 classifications, the 1st one classifies it as Low velocity <2500 xss=removed> 2500 ft. 2 The 2nd classification is divided into: Low velocity <350m>
Injuries caused by HPAF present multiple variables in terms of their production or ballistics mechanism, the site of the injury, the anatomical regions affected, the degrees of injury produced and the evolution that the affected organs may have. The amount of kinetic energy transferred from the projectile to surrounding tissues, internal organs and directly damaged structures, as well as the final location of the projectile, determines the severity of gunshot projectile wounds.1 These injuries are complex due to their proximity neurovascular structures and the concurrent participation of various tissues (tendinous, bone or nerve) 3; which require complex and meticulously planned treatments.








Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
