
Case Report | DOI: https://doi.org/10.31579/2690-4861/152
1 Hospital Nacional El Salvador. Physician, Intensive Care Department. San Salvador-El Salvador.
2 Hospital Nacional El Salvador. Physician, Head of the Intensive Care Department. San Salvador-El Salvador.
3 Hospital Nacional El Salvador. Physician, Head of Teaching and Research Department. San Salvador-El Salvador.
4 Hospital Nacional El Salvador. Resident Physician, Intensive Care Department. San Salvador-El Salvador.
5 Hospital Nacional El Salvador. Resident Physician, Intensive Care Department. San Salvador-El Salvador.
6 Hospital Nacional El Salvador. Physician, Intensive Care Department. San Salvador-El Salvador.
7 Hospital Nacional El Salvador. Physician, Intermediate Care Coordinator, Intensive Care Department. San Salvador-El Salvador.
8 Hospital Nacional El Salvador. Physician, Intermediate Care Coordinator, Intensive Care Department. San Salvador-El Salvador.
9 Student, fifth year medical degree. Universidad Jose Matias Delgado. San Salvador-El Salvador.
*Corresponding Author: Tamayo Ortiz Jose Luis, Hospital Nacional El Salvador. Physician, Intensive Care Department. San Salvador-El Salvador.
Citation: Tamayo Ortiz JL, Bello Quesada M, Camputaro LA, et al. (2021) Lupic Outbreak and Covid-19 Pneumonia Lupus Flare and Pneumonia Covid-19-Case Report. International Journal of Clinical Case Reports and Reviews. 7(5); DOI:10.31579/2690-4861/152
Copyright: © 2021 Tamayo Ortiz Jose Luis, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 June 2021 | Accepted: 13 July 2021 | Published: 21 July 2021
Keywords: sle; covid-19; lupus-flare; sars-cov-2
Coronavirus disease 2019 (COVID-19) is a respiratory infection that can cause mild symptoms or even death, to patients who suffer from it. It affects all population groups without distinction. Systematic Lupus Erythematosus (SLE) is a chronic and fluctuating autoimmune disease. One of the goals of the treatment is to avoid flare-ups and thereby reduce mortality. Their innate alterations in immunity, added to the use of immunosuppressive drugs to control the disease and prevent outbreaks makes them more vulnerable to develop severe symptoms in SARS-CoV-2 infection. We present the case of a patient with SLE infected by SARS-CoV-2 with a lupus flare during hospitalization, entailing a diagnostic and therapeutic challenge.
It has been more than a year (March 11, 2020) since the World Health Organization (WHO) declares the coronavirus disease 2019 (COVID-19) as a pandemic [1]. There are still many questions about severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). In its mild form, infected patients develop well-tolerated respiratory, gastrointestinal, and neurological symptoms, but in its severe form they can developed septic shock and multiple organ failure [2-4]. The most affected populations are the elderly and especially those with comorbidities. The immune response plays an important role against viral diseases, both as antiviral defense and in disease progression. Systemic Lupus Erythematosus (SLE) is a chronic, autoimmune and multisystemic disease with a fluctuating clinical course. It mainly affects women, being more prevalent African and Hispanic [5]. Research has been conducted prior to the pandemic showing that patients with SLE are at increased risk of infection, a risk that is greater if patients have higher levels of disease activity, the use of corticosteroids on a regular basis, or who have previously received treatment with cyclophosphamide or rituximab [6,7]. However, some studies suggest that immunosuppression secondary to SLE management may be beneficial by reducing the immune system's response to COVID-19 [8-9], while other studies report that intense immunosuppression does not allow an effective antiviral response to the exposure to COVID-19, triggering a more severe form of the disease [10,11]. The COVID-19 global rheumatology alliance reported one of the largest series of 600 Covid-19 patients, with various underlying rheumatological disorders from 40 countries. Although the study did not report on the incidence of Covid-19 in these patients, although describes that a glucocorticoid dose greater than 10 mg per day was associated with a higher risk of hospitalization [12].
Despite the various available treatment options at present, only 20-30% of patients with SLE have an inactive or active chronic disease [13,14], the rest experiment flare-ups periods that can cause permanent organic damage with increase of morbidity, mortality, and health costs [15-19].
The consensus definition of lupus flare refers to a measurable increase in the disease activity involving new or worse clinical signs and symptoms and/or laboratory markers. This should be considered clinically significant by the physician and generally leads to evaluate a treatment change or upscale [20]. Of the Instruments available and used to date to assess disease activity, the SLE Disease Activity Index (SLEDAI) with modifications (SLEDAI 2K, SELENA-SLEDAI) [21] and the British Isles Lupus Assessment Group 2004 (BILAG 2004) [22] are the most widely used in both clinical practice and research studies. SLEDAI reflects disease activity in the last 30 days and has a significant prognosis value of mortality in the next 6 months [23]. Among the serological markers, the increase in the titers of the anti-dsDNA double-chain antibody, and the low levels of complement are part of the evaluation.
The European League against Rheumatism (EULAR) guide, within its recommendations establishes that outbreaks can be treated according to the severity of organ involvement by adjusting ongoing therapies (glucocorticoids, immunomodulatory agents) to higher doses, changing, or adding new therapies. The goal of preventing flare-ups is to avoid permanent organ damage and thereby improve the prognosis [24].
Strict control and monitoring are a fundamental part to reduce outbreaks in patients with SLE, however, the coronavirus pandemic has limited controls in this type of patients given that exposing them to public and hospital circulation leads to an increased risk of contagion. This situation generated a higher risk of poor adherence, greater presence of decompensations, outbreaks or worsening and the possibility of coexisting a flare and coronavirus infection.
The following report is a clinical case of a patient with lupus outbreak and SARS-COV-2 infection.
A 23-year-old female patient with history of systemic lupus erythematosus (SLE) approximately diagnosed 3 years ago with lupus nephritis and HBP.
Usual medication: cyclosporine 100 mg/day, mycophenolate 250 mg every 8 hours, enalapril 10 mg day, ASA (acetylsalicylic acid) 100 mg/day, Omeprazole, Furosemide 40 mg / day.
She consulted in a peripheral hospital due to clinical presentation characterized by persistent non-productive cough associated with dyspnea on moderate efforts. She was admitted for COVID-19 suspicion and treatment according to the Covid-19 Protocol was initiated. Faced with the refusal of the diagnosis by relatives, voluntary discharge is requested and continued with outpatient medical treatment. At home, she continued with persistent cough, fever, adds anosmia, ageusia and progression of dyspnea. On 01/14/2021, after 1 month of clinical symptoms, she re-entered the peripheral hospital and later was transferred to El Salvador´s National Hospital.
At Emergency area of Hospital El Salvador, the patient present desaturation, fever and drowsiness. Vital signs upon admission: BP: 128/65mmHG, HR: 148 bpm, RR: 28 rpm, SatO2: 88%, T °: 38.5°. Laboratory admission: Hematocrit: 39.2%, Hemoglobin: 13.4 gr/dl, Platelets: 358,000, White blood cells: 7,600, Neutrophils: 93.9%, Lymphocytes: 3.30%, Urea: 39.1 mg/dl, Creatinine: 0.68 mg/dl, Sodium: 139 meq/l, Potassium: 5.3 meq/l, AST UI/l: 115, ALT: 36.9 UI/l, LD: 662 UI/l, CRP = 8.1 mg/l, Ferritin: 2065 ng/ml, IL6: 33.8, Fibrinogen: 349 mg/dl, DD: 2824.98 mg/l. She was admitted to the intensive care unit and started with ventilatory support with a reservoir mask, achieving SATO2: 95%. The COVID-19 Protocol continues. A chest X-ray is performed (Fig.1) it showed bilateral infiltrates, left predominancy and bilateral blunting of costophrenic angles. Arterial blood gas: PH: 7.38, PCO2: 33.5, PO2: 65.9, HCO3: 20.1, SATO2: 92%. COVID-19 treatment protocol was continued during hospitalization.

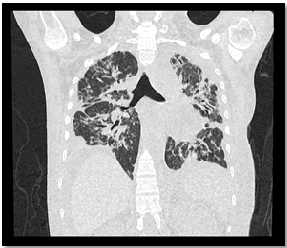
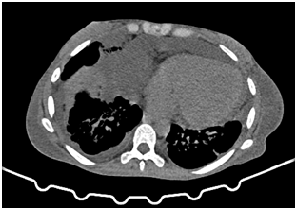
Twenty four hours after admission the patient presented drowsiness, delirium, radiographic infiltrates progression, hypoxemia, increased breathing effort and arterial hypertension. Oxygen support device was change to a high-flow cannula and set with the following parameters: 50 lts/min flow and fio2 50%, improving saturation to 96%. Thoracic (Fig. 2,3,4) and abdominal (Fig. 5,6) CT scan without EV contrast was performed, it showed: multiple ground glass opacities in both lung fields, which compromised more than 75% of each one, subpleural septal thickening, bilateral basal subpleural bands, and some areas of subpleural honeycombing changes in the apex. Pericardial effusion with 3.2 cm thickness extends to the pericardial recesses and basal bilateral laminar pleural effusion was also observed. Within the mediastinum findings, inflammatory nodes were identified. The presence of free perihepatic, perisplenic fluid, was an incidental finding in upper abdomen. Both kidneys were enlarged, swollen, with bilateral pararenal laminar fluid. Soft tissues and bone structures present no abnormalities.



Clinical finding seven days after admission suggested deep vein thrombosis in right inferior limb and venous doppler scan shows right femoral and saphenous vein thrombosis. Due to COVID-19 protocol the patient received anticoagulation treatment with enoxaparin 1 mg/k/day, dose was increased to 1 mg/kg every 12 hours, and antiplatelet agents were add.
Given the CT scan findings associated with arterial hypertension and altered level of consciousness, in addition to COVID-19 pneumonia, clinical signs of lupus outbreak were suspected. SLEDAI scale was performed: 20 (Organic brain syndrome: 8, Urinary casts: 4, Proteinuria: 4, Pleurisy: 2, Pericarditis: 2), corresponding to high activity or very high activity. The general urine test and 24 hrs urine collection test informed: Creatinine clearance: 56 ml / min, proteins in 24 hrs: 6.31 gr / 24hrs. Given these findings with high suspicion of a lupus outbreak and without evidence of active infection (negative cultures), it was decided to start high-dose corticosteroid pulse therapy (methylprednisolone: 1 gram / day) for 3 consecutive days.
The patient had a favorable response to treatment, presented remission of arterial hypertension, drowsiness, headache, delirium, without progression of respiratory failure. Corticosteroids were tapered down until10 mg per day dose was achieved, then immunosuppressive treatment was started.
During hospitalization the patient presented asymmetric edema of the left upper limb. Due to deep venous thrombosis clinical suspicion, a vascular doppler was performed, which informed left upper limb cephalic vein thrombosis. Anticoagulation with oral anticoagulants was prescribed.
The present case report represents a great medical dilemma, due to diagnostic approach and therapeutic decisions complexity of patients with chronic multisystemic diseases admitted to critical care units [8-11]. Patients with SLE in an advanced-stage renal failure represent a medical challenge itself, in this case report severe COVID-19 pneumonia obscure the medical diagnosis. Despite the substantial bilateral involvement of the lung parenchyma, the latent risk of mechanical ventilation gradually decreased over the hospitalizacion. However, we noticed clinical manifestations (altered level of consciousness, fever, joint pain, arterial hypertension), laboratory and imaging (proteinuria, increased inflammatory parameters, serositis) that could not be fully attributed to COVID-19, which generated a reasonable clinical uncertainty of a Lupus Outbreak [20].
To corroborate our clinical suspicion all the methods available in our institution were performed [21-22], to prescribe corticosteroid pulses therapy because of the risk that this therapy entails. The use of corticosteroids is justified in the lupus flare [24], but in COVID-19 there was no evidence available of the benefit of corticosteroids until the publication of the RECOVERY study [25] and to date the METCOVID trial did not show benefit in mortality to 28 days in those under 60 years of age [26].
In the present clinical case, it was pondered the lupus outbreak as the principal cause of the patient's health deterioration, for which the decision was made to perform corticosteroid pulses therapy, achieving remission of symptoms, reduction of inflammatory parameters and clinical improvement significant. Based on the clinical evolution, we can interpret the benefit of the therapy with high-dose corticosteroids pulsed in relation to the lupus flare, but we do not know if it could have contributed to limit the COVID 19 cytokine storm [27].
Patients with autoimmune and immunosuppressed diseases always present a great challenge when they are admitted to the critical care unit. We have witnessed that COVID-19 generates a different impact in each population group and to date we still have many questions about how its approach should be in certain patients. The clinical suspicion, the sum of variables, the multidisciplinary intervention in decision-making together with the best available evidence is an adequate strategy in the fight against this terrible disease.
ABBREVIATIONS
WHO: World Health Organization
SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2
SLE: Systemic Lupus Erythematosus
SLEDAI: Systemic Lupus Erythematosus Disease Activity Index
SLEDAI 2K: Systemic lupus erythematosus disease activity index 2000
SELENA SLEDAI: The Safety of Estrogens in Lupus Erythematosus-National Assessment Trial SLEDAI
BILAG 2004: British Isles Lupus Assessment group
anti-dsDNA: Anti-double stranded DNA
EULAR: European Alliance of Associations for Rheumatology
AST: Aspartate transaminase.
ALT: Alanine transaminase
LD: L-lactate dehydrogenase
CRP: C-reactive protein
IL6: Interleukin 6
NA: sodium
K: Potasium
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
