
case report | DOI: https://doi.org/10.31579/2637-8876/026
Dept. of Emergency Medicine, Singapore General Hospital
*Corresponding Author: Richmond R Gomes, Dept. of Emergency Medicine, Singapore General Hospital.
Citation: Richmond R Gomes. (2022) Lemierre Syndrome: a Forgotten Disease, Complicated by Nocardial Necrotizing Fascitis and Pyomyositis of Right Calf. J. Immunology and Inflammation Diseases Therapy. 5(2); Doi:10.31579/2637-8876/026
Copyright: © 2022 Richmond R Gomes. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 December 2021 | Accepted: 06 January 2022 | Published: 13 January 2022
Keywords: lemierre syndrome; fusobacteriumnecrophoru; necrobacillosis; septic thrombophlebitis; pyomyositis
Once coined the “Forgotten Disease,” Lemierre’ssyndromealso known as human necrobacillosis is a rare condition that results from oropharyngeal infection with an obligate anaerobic gram-negative bacterium Fusobacteriumnecrophorum characterized by septic thrombophlebitis of the internal jugular vein, high fevers, and metastatic septic emboli. Necrobacillosis is the English term describing the necrotic abscesses associated fusobacterium sepsis. Most cases of F. necrophorum occur in association with an antecedent pharyngitis or head/neck infection; We describe an unusual case of necrobacillosis later complicated by lower extremity nocardialpyomyositis and necrotizing fasciitis in a 9 year old otherwise healthy female child with a history of a preceding pharyngotonsillitiswhich required incision and drainage with surgical washout in addition to long term systemic broad antibiotics.
Lemierre Syndrome (LS), also known as human necrobacillosis, was first described in 1900 by Courmont and Cadebut In 1936, the French bacteriologist Andre Lemierre published a report detailing the link between septicemia and pharyngitis that he had observed while working at the Claude Bernard Hospital in Paris1. The postanginal septicemia which now bears his name is most often precipitated by a suppurative oropharyngeal infection. The infection is typically caused by the gram-negative, anaerobic Fusobacteriumnecrophorum. Fusobacteria can be found as normal flora inthe upper respiratory tract of humans 2. Other anaerobic bacteria have been identified as sources of infection, but these are atypical 3. The disease mostly affects young, otherwise healthy adults. The first symptom is typically a sore throat secondary to exudative tonsillitis or peritonsillar abscess. The infection then spreads into adjacent structures,such as the internal jugular vein and carotid artery. Thrombophlebitis of the neck veins can cause pain, swelling, and dysphagia. Sepsis with complicating metastatic spread of septic microemboli is the typical progression of illness[4].The most common site of metastatic spread is the lungs, with 85% of cases demonstrating pulmonary infiltrates [5]. Other feared complications include spread of infection along the carotid sheath and into the mediastinum [4]. Mortality rate before advent of antibiotics was extremely high, with 18 of Andre Lemierre’s 20 identified patients succumbing to their disease[1]. In the modern era of medicine, mortality rates range from 6.4 to 17% [6,7].Timely recognition and prompt treatment are cornerstone’s in prevention of complications.
Case Report
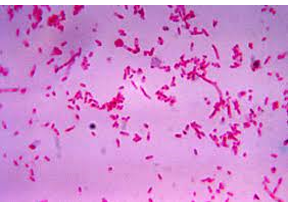
An otherwise healthy 9-years-old female child from rural Bangladesh presented with 1-week history of sore throat and high fever. The pain was continuous and was radiating to the right ear and the right side of the neck. The pain was aggravated by swallowing both solid and liquid diet. The pain was also aggravated by neck movements. There was no breathing difficulty.4 days before, she hadstarted amoxicillin by a local physician (250 mg od) for suspected streptococcal acute pharyngotonsillitis,obtaining only partial relief of the throat pain.She denied any recent dental procedures or tooth infections. She had no significant past medical history and was taking no medications. On examination, she was alert, conscious but hypotensive(blood pressure 90/50 mm of Hg), her temperature in the emergency department was 104° Fahrenheit, and her heart rate was 120 beats per minute (bpm), respiratory rate 15 breaths per minute.Neck palpation revealed swollen neck with fullness and tenderness in the anterior and posterior cervical lymph nodes bilaterally. She was unable to open his mouth more than 1.5–2 inches due to pain and swelling. Her oropharynx appeared erythematous. On respiratory system examination,she had good air entry bilaterally without wheezes or crackles.Laboratory tests showed neutrophilic leukocytosis(white blood cells count 16.26 × 109/L, neutrophils 87%), and elevated C-reactive protein (135.9mg/dL). An unexpectedly high procalcitonin value (29.4 ng/mL) raised the suspicion of bacterial sepsis. Other lab reports were normal: creatinine was 1.03mg/dl, glucose 105mg/dl, albumin low at 2.6, sodium 138 mmol/L, potassium 3.7mmol/L, and alanine aminotransferase (ALT) 30U/L. The chest radiograph showed a right perihilar infiltrate.After drawing blood culture (aerobic,anerobic culture was not available),an empirical treatment with meropenemwas started. Two days later, the patient was stillfebrile and mildly lethargic, with toxic appearance. Bloodculture failed to revealed growth of any organism.A neck ultrasoundwas performed, showingmultiple enlarged cervical lymph nodes,bilateral peritonsillar multiloculated enhancing fluid collections. It also showed punctate foci within the rightinternal jugular vein, which was thought to represent partialthrombosis. Surgical debridement was done and as wound swab gram stain showed Fusobacteriumnecrophorum, ananaerobic gram negative rod(figure 1), intravenous clindamycinwas added to meropenem.
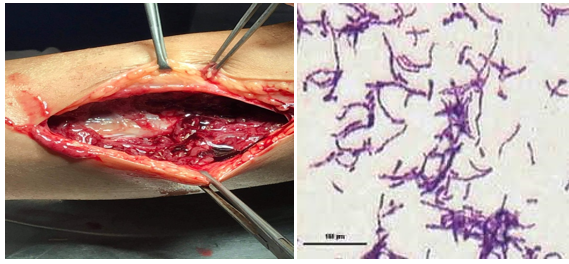
Five days later, which she noted right calf pain that she attributed tom“slipping and hyperextending her ankle”. On local examination Her right calf was moderately swollencompared to the left and was tender. She had good pulses inboth dorsalis pedis and posterior tibialis in both legs inaddition to full range of motion in his ankles. A right lower extremityultrasound was ordered due to the pain and swelling in hisright calf. This study was negative for deep vein thrombosis. There was edema within the fascial compartments between thegastrocnemius and soleus muscles, as well as in the superficialfascia. A crescent-shaped subfascial fluid collectionwas also noted over the medial head of the gastrocnemius
muscle, indicative of right lower leg fasciitis. The decisionwas made to proceed with incision and drainage of the fluidcollection, in addition to a debridement of the right legnecrotizing fasciitis (figure 2). Abscess drainage resulted in approximately500 ml of purulent foul-smelling fluid, some of whichwas sent for gram stain and culture. A wash out of the rightlower extremity wounds would be performed several dayslater with subsequent placement of negative pressure wounddressing. Gram smear (Figure 3 ) showed Gram-positive filamentous bacteria which were weakly acid fast (Nocardia sp.).
She was initiated on treatment with intravenous amoxycilin and clavulanic acid. With regular dressing and antibiotic treatment her condition improved. On discharge, antibiotics were switched to oral from. There was a plan to continue clindamycin for 6 weeks and amoxycilin and clavulanic acid for 6 months. On follow up, 4 weeks later she was asymptomatic and doing well.
Discussion
The increased use of antibiotics to treat pharyngitis has led to a decreased occurrence of Lemierre’s Syndrome, earning it themoniker “the forgotten disease.” One source states incidencein the early 1990s was as low as 0.8–1.5 per million persons per year [8].However, there have been an increased number ofcases reported over the last 20 years[9].There have beenseveral proposed reasons for this increase in incidence. Onepossible cause is a decreased use of antibiotics to treat uncomplicated
pharyngitis.Another postulate is that improved anaerobic culturing techniques have led to increased
detection of Fusobacteriuminfection.Yet another theory is that the increased number of cases is due toemerging antibiotic resistance amongst Fusobacteriumspecies.A recent study showed the resistance rate to erythromycinwas as high as 15% amongst strains of Fusobacteriumnecrophorum[10]. Penicillin resistance has also been reporteddue to production of beta-lactamase by some strains ofFusobacteriumnecrophorum[11].
The first case of human necrobacillosis was reported in 1900 by Courmont and Cade [12]. This was followed by a report in 1936 by Lemierre, which identified a series of patients with Fusobacterium spp. infections; since this report, the eponym “Lemierre’s syndrome” has been used to describe Fusobacterium spp. infections of the internal jugular vein complicated by metastatic abscesses[1]. In both original and recent case descriptions, most patients had an antecedent pharyngotonsillitis presenting as a sore throat and pharyngeal hyperemia. In a recent review among 87% of cases, the primary source of infection was the palatine tonsils and peritonsillar tissue[6].Up to one third of patients presents a mixed infection frequently with streptococci and other gram negative anaerobes.
F. necrophorumis a non-spore-forming gram negative anaerobic rod belonging to the normal flora of the oropharynx and is recognized as the causal agent of approximately 10% to 20% of pharyngitis cases in adolescents[2,13-15].The disease is often initially misdiagnosed as a viral pharyngitis, especially mononucleosis2. Several clinical clues can be helpful in distinguishing Lemierre’s syndrome from mononucleosis. For instance, mononucleosis typically presents with more generalized lymphadenopathy in contrast to the more localized cervical lymphadenopathy of Lemierre’s syndrome. Another clue, and one of the most typical findings of a Lemierre’s syndrome, is the presence of lung infiltrates. In young patients with pharyngitis, the presence of concurrent lung lesions should raise the clinical suspicion for Lemierre’s syndrome. Critical to the diagnosis of Lemierre’s syndrome is the prompt collection of blood cultures and the culturing of any fluid drained from abscesses that may be present. However, Fusobacteriumnecrophorumtakes at least 48 hours to grow in culture and sometimes as long as seven days [2], so clinicians may find it necessary to treat empirically while awaiting culture results.
Infection typically occurs in distinct stages beginning with pharyngitis followed by local invasion into the pharyngeal space leading to thrombophlebitis of the internal jugular vein. Timing of the second stage is variable, but usually occurs within one week. Patients with Lemierre’s syndrome may have a proceeding bacterial or viral (e.g., infectious mononucleosis) pharyngitis, which may contribute to the translocation of the Fusobacterium spp. into the deep spaces of the neck. The third stage of infection is metastatic spread, most commonly to the lungs (80%) followed by the joints (17%); occasionally, the liver, spleen, bones, kidneys, and meninges are involved6. Today, the term “Lemierre’s syndrome” is used to describe Fusobacterium spp. infections originating not only in the pharynx, but in any structure in the head and neck (e.g., otitis, sinusitis, mastoiditis, parotitis, odontogenic infection, or facial skin infection) [7].
Most cases of classic Lemierre’s syndrome occur in young, otherwise healthy, adults, ages 16-23 years, with a propensity for development among males[10]. Necrobacillosis may occur in association with a primary infection of the skin, genitourinary or gastrointestinal systems16, as F. necrophorum is part of the normal flora of these areas as well as in the oropharynx. Bacteremia may occur when host defenses are compromised and the organism penetrates the mucosal surfaces such as cancer patients undergoing chemotherapy who develop mucositis.
Thediagnosis of Lemierre’s syndrome requires full awareness of this rare condition and high index of clinical suspicion. The disease should be suspected in young patients with history of oropharyngeal infection who failed to improve either spontaneously or after antibiotic treatment and developedclinical and laboratory evidences of sepsis, respiratory symptoms, or atypical unilateral neck pain and swelling. The latter symptoms are characteristic of Lemierre’s syndrome, being the consequence of unilateral jugular vein thrombosis. Confirmation of the diagnosis requires the detection of the internal jugular thrombophlebitis and septic embolization to lung and other organs by imaging studies (duplex ultrasound, computed tomography, and magnetic resonance ) and by blood and wound cultures that demonstrate F. necrophorum; anaerobic cultures are required for growth of this organism. Laboratory data may reveal leukocytosis (75%), thrombocytopenia (24%), increased bilirubin (19%), or hematuria (6%)6; elevated liver function tests and creatinine have also been described[17,18]. Chest radiography may show a cavitating pneumonia, pulmonary infiltrates, an abscess, pleural effusions, pneumothorax, pneumatoceles, or may be normal.
Our patient was a young, immunocompetent children who presented with fever, neck pain, dysphagia, pharyngitis later complicated with pyomyositis and fasciitis of his lower extremity. The origin of his Fusobacterium spp. infection remains unclear (as in 8% of cases)[6].
We searched the English literature (MEDLINE, 1950-2006; EMBASE 1980-2006) for cases of pyomyositis due to Fusobacterium spp. using the search terms “Fusobacterium” or “Lemierre’s” and “pyomyositis” or “myositis”. Four cases with detailed clinical information have been published in the literature, all of which occurred in association with an adjacent septic joint (most frequently the hip, shoulder, or knee)[19-22], and all were due to F. nucleatum. Our case is unique in that there was no evidence on arthroscopic examination or synovial fluid cultures of a concurrent septic arthritis and that the organism was the more virulent species of Fusobacterium, F. necrophorum.
Pyomyositis, classically an infection of the tropics, is defined as a primary suppurative infection of the skeletal muscle, first described by Scriba in 1885[23]. Predisposing factors include conditions characterized by immunodeficiency (T cell deficiency, Chronic granulomatous disease, hyper-IgE syndrome, HIV, Malignancy, Diabetes, use of steroids and immunosuppressants), trauma, concurrent infection (with Toxocariasis, Varicella or Arbovirus) and malnutrition.[24,25]. The common causative organisms are Gram positive bacteria, such as Staphylococcus aureus (90% in tropics and 75% in temperate regions) and Group A Streptococcus (1-5%).[25]. Seventy-five percent of cases occur in immunocompromised individuals, the thigh being a common site[26]Nocardial pyomyositis is extremely rare but responds well to treatment if initiated early [27].Three clinical stages of disease process have been described: invasive (bacterial seeding), suppurative (abscess formation) and septicaemic stage (dissemination in blood with multiple organ dysfunction). The presentation of localised muscle pain, edema, low grade fever in first stage leads to misdiagnosis of muscle strain or contusion. Pain and swelling in the second stage leads to differentials of deep vein thrombosis, septic arthritis or osteomyelitis. By definition, pyomyositis never occurs secondary to contiguous infection of soft tissue or joints nor due to penetrating trauma. However in third stage as a part of septicaemia when it involves skin, leading to cutaneous gangrene, it can present as necrotising fasciitis like picture.
Aspiration of pus from the muscle or muscle biopsy (in case of absent macro abscess as in the early invasive stage) with culture and gram staining is the gold standard for diagnosis. But in tropical regions, pus cultures are sterile in 15-30
Lemierre disease is suppurative thrombophlebitis of internal jugular vein secondary to oropharyngeal infection and can be complicated by septic emboli. Early diagnosis and prompt treatment with long term antibiotics with beta-lactamase anaerobic activity results in complete resolution of the condition.The present casesuggests that (1) the recommended oral antibiotic treatmentfor acute pharyngeal infections does not always prevent theprogression of the disease into the life-threatening Lemierre’ssyndrome; (2) an anaerobic infection and the Lemierre’ssyndrome should be suspected in patients affected by pharyngotonsillitis with a severe and unusual course; (3)in these patients an empirical antibiotic therapy, active alsoagainst anaerobic microorganism, has to be started early;moreover, an imaging study of the neck, searching for jugularthrombophlebitis and parapharyngeal abscesses, should beobtained as soon as possible.
Conflict of Interest: None declared
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
