
Case Report | DOI: https://doi.org/10.31579/2690-4861/441
Department of Surgery, Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), PMB 5022, Awka. Anambra State, Nigeria.
*Corresponding Author: Nonso Mbah, Department of Surgery, Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), PMB 5022, Awka. Anambra State, Nigeria.
Citation: Nonso Mbah, (2024), Idiopathic Ileocolonic Intussusception in the Elderly: Case Report and Literature Review, International Journal of Clinical Case Reports and Reviews, 17(2); DOI:10.31579/2690-4861/441
Copyright: © 2024, Nonso Mbah. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 April 2024 | Accepted: 11 April 2024 | Published: 18 April 2024
Keywords: adult intussusception; idiopathic; 9th decade of life; ileocolonic; surgical operation
Background: Adult intussusception is rare, in sharp contrast to childhood intussusception. It’s often considered a distinct disease entity from the paediatric intussusception because of dissimilarities in the aetiology, clinical presentation and management options. Operative treatment is mandatory for the management of colonic intussusception in the adult patient as many cases are associated with bowel tumours.
Case presentation: An 86-year-old male retired civil servant presented with clinical and radiological features of ileocolonic intussusception. He had extended right hemicolectomy. The histology revealed an idiopathic ileocolic intussusception without an associated bowel tumour. He made an uneventful recovery and was discharged on the 8th day after surgery.
Conclusion: Adult intussusception is not only rarer than the childhood disease, but requires mandatory surgical operation for treatment. This case involving an elderly patient in his 9th decade of life is reported to highlight the deviation from the usual pattern of presentation of this disease in an adult patient.
Intussusception, the invagination of a part of the bowel into the adjacent segment, affects both children and adults [1]. However, the aetiology, clinical features and management of adult intussusception are quite different from the paediatric disease [2]. Intussusception represents only about 1% of bowel obstruction in the adult population, 0.08% of all abdominal operations and < 0.1% of overall hospital admissions among adults [3].
Unlike childhood intussusception, the adult condition rarely presents with the classical triad of colicky abdominal pain, abdominal lump and the passage of red currant jelly stool.4 Indeed, the clinical presentation of intussusception in adults is often ambiguous, elusive and nonspecific, thereby making the diagnosis very challenging.5 This is because adult intussusception is an infrequent cause of abdominal pain and intestinal obstruction. Likewise, the clinical examination of these patients is often negative. However, meticulous clinical history and physical examination combined with ancillary imaging investigations, like abdominal ultrasound scan and multi-detector computed tomography (MDCT) scan, readily provide the accurate diagnosis in the adult patient [6] .
Whereas the uncomplicated childhood intussusception could be safely managed non-operatively, colonic intussusception in adults require mandatory operative treatment because many cases are associated with malignant bowel tumors [7,8].
Mr G. I. E, 86 years old retired civil servant, presented via the Accident and Emergency department of the hospital on referral from a peripheral hospital in September 2023 with 5-days history of post-prandial central abdominal discomfort, abdominal distension, poor appetite, inability to open his bowels properly and occasional haematochezia. He had a single episode of vomiting at the onset and admitted to have lost some weight. He was a known hypertensive and was regular with his medications. His past surgical history was unremarkable.
Clinically, he appeared frail and dehydrated. His vital signs were unremarkable. The abdomen was distended, globally soft and slightly tender, but not peritonitic. There was a palpable mobile mass, the size of an avocado pear, situated at the right upper abdominal region and partly extended into the right lower quadrant.
He came with an abdominal ultrasound scan report which confirmed intussusception.
The abdominopelvic CT scan showed “the small bowel telescoping through the transverse colon up to the splenic flexure. The intussusceptum measured 16.9cm while the intususcipiens measured 18.5cm. There was associated dilated central bowel loops with air-fluid levels”. The radiological conclusion was colo-colonic intussusception involving the transverse colon.
From all the foregoing, our clinical diagnosis was incomplete large bowel obstruction secondary to colonic intussusception.
His PCV was 28%, the serum potassium was 2.8mmol/L but the viral markers were negative for HIV and hepatitis B and C.
He was duly worked up for an exploratory laparotomy. The patient received 1-unit of blood transfusion and correction of hypokalaemia. He had urethral catheterization, bowel preparation and was commenced on total parenteral nutrition.
Intra-operatively, we found the invagination of the terminal ileum, proximal part of the vermiform appendix and caecum into the ascending and transverse colon. The intussusceptum extended up to the splenic flexure (figs. 1, 2 and 3). The right iliac fossa was empty and there was 300mls of serosanquinous fluid in the peritoneal cavity.
An extended right hemicolectomy was performed with primary ileo-colonic anastomosis. Anal dilation was done at the conclusion of the operation.
The histology report revealed haemorrhagic necrosis with marked mucosal fragmentation and vascular congestion in the ileal section of the intussusceptum and colonic parts of the intususcipiens. No malignancy was identified.
The patient made an uneventful post-operative recovery and was discharged home on the 8th day after surgery. He’s been followed up at the outpatient surgery clinic for 6-months and has remained clinically well.

Figure 1: Intussusception insitu.
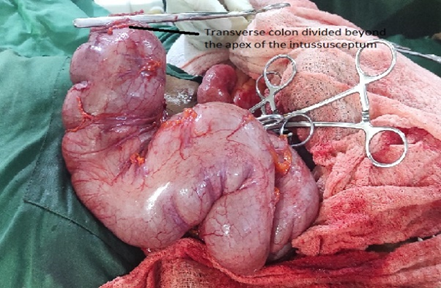
Figure2: Transverse colon divided distal to the apex of the intussusceptum
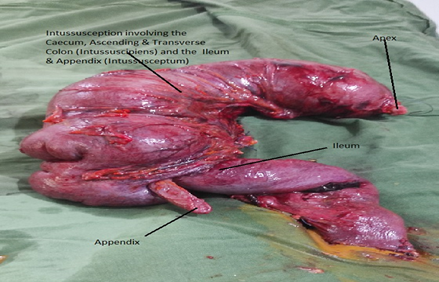
Figure 3: Right hemicolectomy specimen comprising the complete intussusception.
Our patient presented in the 9th decade of life, an uncommon age for the development of intussusception. About 95 % of cases of this disease are seen in children below 16 years, with the majority presenting during infancy [1].
The triad of colicky abdominal pain, presence of a palpable abdominal lump and the passage of red currant jelly stool in a child is pathognomonic of intussusception. This classical triad is only present in about 2% of adults with the disease [9]. The patient presented in this report had a palpable lump and abdominal discomfort, but red currant jelly stool was absent. Rather, the history of occasional haematochezia was obtained. These clinical features mimicked the manifestation of intussusception in children and therefore simplified the diagnosis of this disease in our patient.
Where imaging investigations like abdominal ultrasound scan and CT scan are available, the definitive diagnosis of adult intussusception is straight forward, as in the case presented [6].
The definitive management of adult intussusception requires mandatory surgical treatment because the majority is due to a primary pathology, which may be bowel tumour [7]. When the colon is involved in adult intussusception, malignancy must be excluded [8]. Laparoscopic surgery where available, rather than the open surgical approach, provides a minimally invasive and preferred option for the management of intussusception particularly in the elderly adult patient.10 Less blood loss, lower morbidity and shorter time to recovery are some of the benefits of the laparoscopic procedure. Our patient received the open surgical operation because laparoscopic surgery was not available at our centre at the time of treatment.
Idiopathic intussusception, where no primary lesion is macroscopically and histologically identified as being the cause and lead point of the disease, occurs mostly in children [2]. Curiously, our patient presented with this form of the disease in his 9th decade of life. The colonic site of involvement necessitated resection of the intussusception by an extended right hemicolectomy in the case presented.
In conclusion, adult intussusception can present with clinical features which are similar to those of the paediatric condition, even in the 9th decade of life. The definitive diagnosis in such cases is often straight forward, both clinically and radiologically. However, surgical treatment is mandatory in adult colonic intussusception in order to exclude a possible neoplastic cause and to treat any associated intestinal obstruction.
None
None
This case report is exempt from ethical approval in our institution.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
