
Case Report | DOI: https://doi.org/10.31579/2578-8949/090
Dermatology, Venereology and Andrology Department, Faculty of Medicine, Assiut University, Assiut, Egypt.
*Corresponding Author: Ayman Mahran, Dermatology, Venereology and Andrology Department, Faculty of Medicine, Assiut University, Assiut, Egypt
Citation: Ayman Mahran , (2019) Generalized Granuloma Annulare Can Be Presented With Different Clinical Morphologies In The Same Patient: A Case Report 4(2) DOI: 10.31579/2578-8949/090
Copyright: © 2019. Ayman Mahran This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 October 2019 | Accepted: 23 October 2019 | Published: 30 October 2019
Keywords: generalized granuloma annulare, atypical granuloma annulare
The term granuloma annulare (GA) appropriately describes the classic type characterized by ringed erythematous plaques with histological palisaded granulomatous inflammation. However, GA now includes a range of disease. Over time, more atypical, rare types have been reported in isolated case reports or small case series. Here, we describe a unique case of generalized GA presented by two morphologically different lesions in a 52 years old diabetic man. To the best of our knowledge, this association has never been reported in the literature.
Granuloma annulare is considered a noninfectious granulomatous skin condition.[1].GA can be presented by multiple clinical types; including localized, generalized, subcutaneous, perforating and many atypical morphologies[2]. Histologically, GA shows collagen degeneration, mucin deposition, and either a palisaded or interstitial histiocytic infiltrate[3].Although the exact etiology is unknown, a cell-mediated hypersensitivity reaction is suggested[4].There are multiple reports of systemic associations with GA, including diabetes mellitus (DM), thyroid dysfunction, malignancy, lipid abnormalities, and infection[5].
A fifty two years old man presented to our clinic by asymptomatic skin lesions over the neck and extremities of 5 months duration. It started on the forearms then spreaded to the neck one month later and gradually increased in size and number. The medical condition of the patient is unremarkable except for diabetes mellitus which was diagnosed four years earlier. Dermatological examination revealed multiple erythematous infiltrated plaques symmetrically distributed over the dorsal aspect of both forearms and hands. (figure 1).

Another lesions of different morphology composed of flesh-colored to erythematous papules, some of them are discrete and others are coalescing into annular plaques over the neck and upper part of the chest (figure 2).

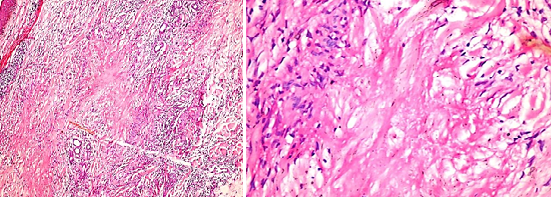
Routine and relevant laboratory investigations were normal except for elevated random blood sugar level: 12.5 mmol/L (normal value: 4-7.8 mmol/L). Two skin biopsies were obtained (one from annular lesions over the neck and the other from infiltrated plaque over the forearms) which revealed almost similar findings in both with the presence of areas of degenerated (necrobiotic) collagen, surrounded by palisaded infiltrate of histiocytes and fibroblasts with few multinucleated giant cells and moderate perivascular and interstitial lymphocytic infiltrate in the surrounding dermis. (figure 3 and 4).


Here we present a case of 52 -year-old diabetic man presented with two clinical morphologies. The lesions over the neck and upper part of the chest are identical to the classic annular presentation of GA with strict photosensitive distribution. On the other hand, the lesions over the forearms and hands are composed of multiple large infiltrated plaques which is an unusual presentation of GA. Although many reports described cases of generalized GA presented with plaques [6] and others reported cases with photosensitive distribution, [7]. none described the coexistence of such two variants (annular and infiltrated plaques) like in our case.
The differential diagnosis for the neck lesions revolves around GA, actinic granuloma, sarcoidosis and porokeratosis. While, the differential diagnosis for the upper limb lesions included GA, leprosy, sarcoidosis and mycosis fungoides. Histological examination of two biopsies from two different lesions confirmed typical feature of GA. We considered this case as a case of generalized GA with atypical presentation.
Granuloma annulare is a benign inflammatory skin disorder with varying morphologies, and multiple subtypes [5].Generally, the age incidence is between the 3rd and 5th decades of life, with a female to male ratio of about 1-2:1[8,9].The most common subtype is localized GA, occurring in 75% of cases[10].Generalized GA is the second most common variant, it occurs in about 15% of patients[11].Whereas localized GA affects young adult females, generalized GA is slightly more common in males with two peak age incidences, children under 10 years and adults over 40 years[12]. Both age and sex incidences perfectly correlate with our case.
Granuloma annulare may be idiopathic, but many studies reported associations with many systemic conditions. Diabetes is one of the most reported diseases associated with GA,[13] which is the case in our patient[5].
Localized GA is usually asymptomatic and self-resolving within two years, however, the patient may need treatment for cosmetic reasons. Treatment is often challenging for generalized GA, because of its recalcitrant nature and a paucity of evidence-based therapy. Many different treatment modalities have been described for GA with different results. These include topical potent corticosteroids, intralesional triamcinolone, topical calcineurin inhibitors, dapsone 5% gel and topical vitamin E. Systemic therapies include dapsone, doxycycline, retinoids, antimalarials, nicotinamide and infliximab. Phototherapy may also be helpful.[10].
The new clinical remark about GA which was noted for the first time in the literature in our case is: Generalized GA can be presented by different clinical morphologies (annular and infiltrated plaques) in the same patient which may create confusion and delay in the diagnosis, and, hence appropriate management.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
