
Case Report | DOI: https://doi.org/10.31579/2641-0419/286
1MD Bait Balev Nesher and The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
*Corresponding Author: Jochanan E. Naschitz, MD Bait Balev Nesher and The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Citation: Jochanan E. Naschitz (2022). ECG at the Bedside: Atrial Bigeminy with Alternating long and Short PR Interval. J. Clinical Cardiology and Cardiovascular Interventions, 6(1); DOI:10.31579/2641-0419/286
Copyright: © 2022 Jochanan E. Naschitz, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 November 2022 | Accepted: 28 November 2022 | Published: 03 January 2023
Keywords: inter-atrial block; bachmann bundle; atrial bigeminy; left atrial extrasystole
The admission electrocardiogram of an 88-year-old woman, showed sinus rhythm, biphasic P waves in leads II, III, with the terminal vector directed upward, P duration 130 msec, PR interval 200 msec, consistent with advanced inter-atrial block. Next, atrial bigeminy occurred originating in the left atrium and delaying the sinus P waves. With the ectopic P’ measuring 60 msec, the likely path of left atrial stimuli to delaying the sinus node was through Bachmann’s bundle, by retrograde conduction. This means that inter-atrial conduction via Bachmann bundle
An inter-atrial block leads to dispersion of the atrial refractory period and contributes to generating re-entry circuits. This is illustrated by occurrence of transient atrial bigeminy. Intriguingly, P' waves and the P'R interval were shortened during atrial extrasystole, challenging our interpretation of the tracing.
The patient, an 88 year-old woman, was admitted for rehabilitation after recovering from pneumonia and hyponatremia. Her medical history was notable for arterial hypertension, ischemic heart disease, atrial fibrillation, and pulmonary embolism. Her medications, daily doses, were apixaban 10 mg, valsartan 160 mg, furosemide 40 mg, and atorvastatin 10 mg. Upon presentation she was alert, the vital signs and routine laboratory tests (CBC, chemistry, thyrotropin) were unremarkable. The ECG showed sinus rhythm 72 beats per minute, P waves duration 130 msec, biphasic P waves in leads II, III and aVF with the terminal vector directed upward, i.e. characteristic features of inter-atrial block. The PR interval measured 200 msec. The QRS had the right bundle branch block pattern. Deep negative T waves were noticed in leads III and aVF. This ECG was comparable with several tracings recorded a few months ago. Three days after admission, while the patient felt well, the ECG had changed: each regular beat was followed by an atrial ectopic beat (Figures 1 and 2). The P waves, alike in earlier tracings, were consistent with sinus rhythm and showed the morphology of advanced inter-atrial block. In distinction from the latter, the ectopic P’ waves' duration was 50 msec, P' were positive in leads I,II,II and V1-V6, and the P'R interval was 120 msec. The P-P' interval was constant. Atrial bigeminy was diagnosed.

Figure 1: Interatrial block and atrial bigeminy. Notice that ectopic atrial waves are positive in leads II and V1, and negative in aVL.
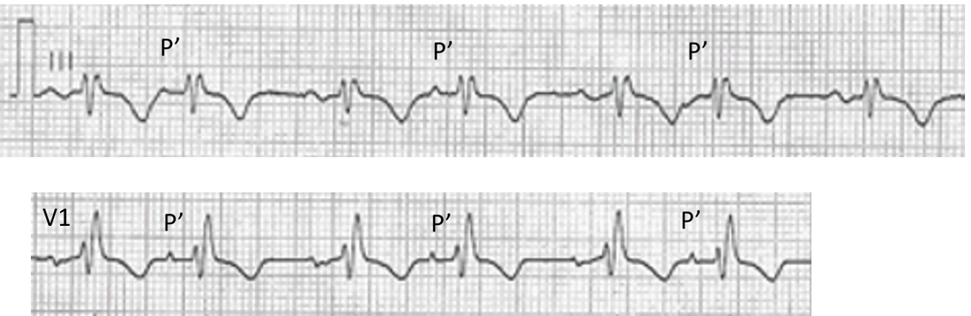
Figure 2: Details of P and P' are evident under magnification. The strips were taken from Figure 1. The P waves in lead III are biphasic, with an early downward vector followed by the late vector directed upward. The maximal P was duration is 130-140 msec, the PR interval 220 msec. In Lead V1, the large negative terminal deflection of the P waves is notched in a to-and-from pattern. P' in leads III and V1 are positive except the third P' in lead III. The P'P interval is 800 msec.
The following day's tracing showed sinus rhythm, no extrasystole (Figure 3).
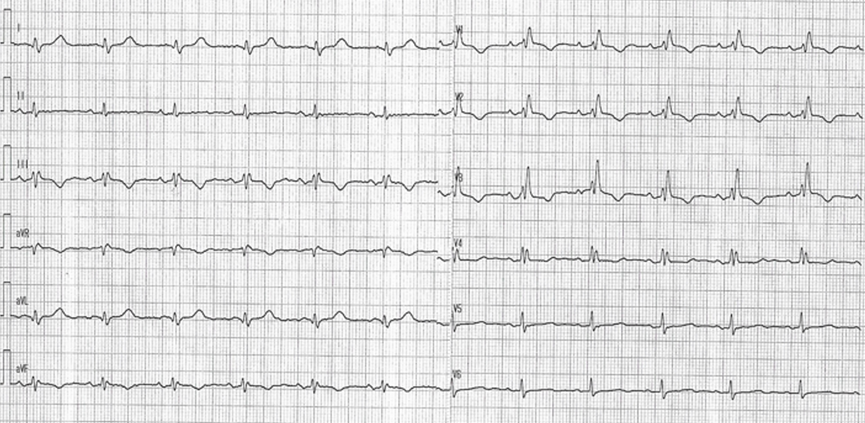
Figure 3: Sinus rhythm 74 bpm, inter-atrial block, no ectopic beats. P-P interval 800 msc. alike P’-P intervals on the previous day's tracing.
Discussion
The P waves in this tracing differ from normal atrial activation. Usually, atrial activation begins with impulse generation in or near the sinus node. From here, the activation extends anteriorly toward the lower portion of the right atrium and inferiorly toward the atrio-ventricular node. The left atrium is activated after the onset of right atrial activation by spread of the stimulus usually through Bachmann's bundle. The latter spans from the right atrium to the left atrium close to the right upper pulmonary vein. Activation proceeds in both atria downward, continuing in the left atrium after the right atrial activation is complete. Accordingly, the normal P waves are positive in lead II and usually in leads I, aVL, and aVF. The P wave in the right precordial leads is typically upright but may be biphasic in leads V 1 and V2 with an initial positive followed by a terminal negative deflection. The normal P wave duration's upper limit is 120 msec measured in the lead where the P wave is widest. The terminal negative deflection in Lead V1 is normally less than 0.1 mV in depth. The normal duration of the PR interval is 120-200 msec [1]. Abnormal P waves suggest an abnormal site of impulse formation and an abnormal course of subsequent activation. When conduction from the right to the left atrium is delayed the P wave duration is longer than 120 msec and the P waves in lead II have two humps, the first corresponding to right atrial activation and the second to left atrial activation, i.e. partial inter-atrial block [2]. With advanced inter-atrial block, the right atrial impulse reaches the left atrium late, after traveling down near the atrioventricular junction and then upward across the left atrium; consequently, the P waves in inferior leads are positive at their beginning and turn negative at termination [2,3]. Bayés de Luna et al. [2] classified these types of blocks as either partial block, when the only ECG abnormality is a P wave that equals or exceeds 120 msec or an advanced block, when the P wave duration is ≥120ms and the P wave is biphasic in the inferior leads II, III, and aVF, beginning positive and becoming negative at termination. Advanced inter-atrial block is frequently associated with left atrial enlargement but may manifest independently of left atrial size [4]. Unusual in this tracing in is the notched terminal deflection of the P wave in lead V1. This contrasts to the common smooth terminal component of the P wave in lead V1 both in partial and advanced Bachmann bundle block as well as in the presence of other left atrial pathologies [5].
Inter-atrial conduction delay leads to the dispersion of the atrial refractory periods, facilitating occurrence of re-entrant atrial arrhythmias, especially atrial fibrillation and atrial flutter [6], but also atrial bigeminy [7] as in the proposito. Atrial bigeminy refers to a sequence of at least two atrial ectopic beats, each one following a sinus beat with a fixed coupling interval. The ectopic beats can be generated from any atrial site. Focal automatism or re-entrant mechanisms may be the mechanisms of atrial ectopy [8]. The combination of a positive P’ in lead V1 with a negative or isoelectric P’ in lead aVL are consistent with the left atrial origin of atrial ectopic beats [7].
Delayed occurrence of the sinus P wave after the ectopic atrial beat (P'P equal to PP) suggests that the sinus node was depolarized by the premature atrial beat. Since the P' duration was short, there obviously was no substantial lag in right atrial depolarization, as would occur if the left atrial impulse reached the right atrium after the long way first down near the atrioventricular junction and then upward across the right atrium. The shortest to imagine course of depolarization from the left atrium to the right atrium is through the Bachmann's bundle, left-to-right, a possibility demonstrated under epicardial mapping [3]. This would mean that the inter-atrial block in this patient was unidirectional from right-to-left, while left-to-right conduction through the Bachmann bundle of ectopic atrial stimuli was not affect
Inter-atrial block is an independent predictor of supraventricular tachyarrhythmias, and it has been associated with left atrial thrombi and systemic embolization. This justified continuing in the proposito anticoagulation with apixaban, though past atrial fibrillation and long time ago pulmonary embolism.
There was no funding to this work and there are no conflicts of interest to declare
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
