
Research Article | DOI: https://doi.org/10.31579/2693-4787/020
University Hospital Leiden, the Netherlands.
*Corresponding Author: George Zhu, University Hospital Leiden, the Netherlands
Citation: George Zhu, Retrospective Survey on the Outcome of 36 Diverse Cases of Anemia. J.Clin Onco Res and Rep. 2(1). Doi: 10.31579/2693-4787/020
Copyright: © 2021 George Zhu, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 January 2021 | Accepted: 24 June 2021 | Published: 02 July 2021
Keywords: plasma protein C antigen; rocket immunoassay
Protein C, a vitamin K-dependent anticoagulant serine protease, is involved in blood coagulation. Activated protein C inactivates Va and VIIIa in purified protein systems and stimulates fibrinolysis by indirectly increasing the level of circulating plasminogen activator. In this process, protein S serve as an important factor for activated protein C. In recent years, excess protein S drives cancer cell proliferation and cell survival through oncogenic receptor Axl (Anexelekto). We determined changes of plasma protein C antigen by using rocket immunoassay both in 50 healthy individuals and 103 distinct hospitalized patients. In healthy individuals protein C antigen(PC:Ag) ranges o.6439- 1.4752 µ/ml. The results showed that plasma protein C antigen was considerably high in 22 diabetes mellitus. In contrast, the PC:Ag was significantly decreased in 19 liver cirrhosis(p< 0.001) and in closely line with serum albumin levels(p< 0.05). In 31 acute leukemias, on the average, there was slightly lower values in PC:Ag, and accompanied with the distribution of significant decrease of PC:Ag values in 5 FAB M5 subtype and in 9 hyperleukocytic leukemias. However, the 3 acute promyelocytic leukemia (APL) with overt laboratory criteria of disseminated intravascular coagulation (DIC) had protein C concentration no lower than the remaining 2 patients with infectious DIC, which suggested the coagulopathy in APL might be due to mechanisms different from other forms of DIC.
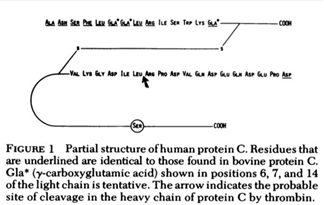
Protein C,a major of blood coagulation, is a vitamin K-dependent serine protease which was activated by thrombin and the endothelial cell cofactor thrombomodulin(1). Human protein C was composed of a light and heavy chain linked by interchain sulfide bridges(figure 1)(2). Anticoagulant properties of protein C derived from its ability to selectively inactivates factor V and VIIIa and accelerates fibrinolysis by iducing a rise in plasma plasminogen activator activity(3). Activated protein C(APC) requires the presence of protein S(4).
Protein S is a plasma protein that serve as an important cofactor for activated protein C in the blood anticoagulant system(4-5). Protein S also act as a mitogen on distinct cell types and is a ligand for Tyro3, a member of the Axl family of oncogenic receptor tyrosine kinases(6-7). The TAM family of proto-oncogenic receptor kinases(Tyro3,Axl and Mer) is implicated in human many cancers(8-11).The fullength Tyro-3,Axl,and Mer protein contain 890,894,and 999 amino acids, respectively(8). Protein S is expressed in lung carcinoma tissue,predominantly in tumors of squamous cell origin,in head and neck and oral squamous cell carcinoma(12). Most of the protein S is synthesized in the liver by hepatocytes together with the closely related protein Gas6,as an activating ligand for TAM family. Gas6 and protein S share 43% amino acid sequence identity and have the same domain structure with the exception of thrombin cleavage sites which present in protein S but not Gas6(8). The role of the TAM cognate ligands Gas6 and protein S was demonstrated in homeostatic regulation of the immune,vascular and nervous systems. Excess protein S drives oral squamous cell carcinoma proliferation and cell survival through high expression and the activation of oncogenic receptor Axl(7,11,13-14,15,16).
In literature review, Griffin etal (17)reported the first family with a congenital protein C deficiency. Bertina & Broekmans(4,18-19) reported the first Dutch family with a congenital protein C deficiency. Using an immunologic assay for protein C(20),we determined the level of protein C antigen in plasma samples due to a varity of diagnostic diseases especially bleeding and thrombotic diathesis.
Venous blood was collected in 1/10 volume of 0.11 M sodium citrate. Plasma was prepared by centrifugation of blood at 3000 rpm for 10 min. Platelet free plasma of 103 patients and 50 healthy volunteers were stored at -20℃ for the assessment of protein C levels. Three tubes with rabbit anti-protein C serum, 2 tubes indubiose-A37 and 1 tube of protein C deficient plasma were kindly supplied by Prof. RM Bertina, Leiden University Hospital, The Netherlands. The period of experimental procedure was completed in early 1986-89.
Plasma protein C assay: A 12.5 ml of 1% indubiose A37 or commercial agarose solution is obtained by boiling in gel buffer (PH8.8 Tris-BB or Tris-BB-EDTA) during continuous stirring. The solution is allowed to cool to 55℃, and a 60 µl amount of rabbit protein C antiserum and a 0.05ml of 0.11 mol/l sodium citrate solution was added during careful mixing. A 100 x 60 x 2 mm gel is prepared on small glass plate by pouring antibody- containing agarose (50~55℃) into a coated glass plate placed on a horizontal table. The gel should harden before wells can be punched. By using a gel puncher template,a row of wells (about 4 mm in diameter) with their centers at least 5 mm apart is punched in the gel. After appropriate dilution the samples (13 µl) are deposited in the wells. Standards in suitable dilutions (1:1,1:2,1:4 and 1:8) are deposited in the middle holes of the row. The test samples were diluted in 1:2. The ionic strength of the samples should preferably be approximately the same as that of the electrophoresis buffer. Subsequently, samples are applied after the glass plate has been placed on the electrophoresis apparatus. Electrophoresis is performed at 120V (4-6 mA/plate) at room temperature 12~30℃ for 20 hours overnight. After staining with 1% phosphomolybdic acid,the length of rocket immunoprecipitate was measured by using a ruler, which is linearly correlated to the amount of antigen. Results (including normal controls and patients) are plotted on log-log paper (length of rocket in mm versus percentage antigen), based on the construction of the standard curve of linear regression equation regarding protein C antigen.
1).Protein C antigen in healthy individuals
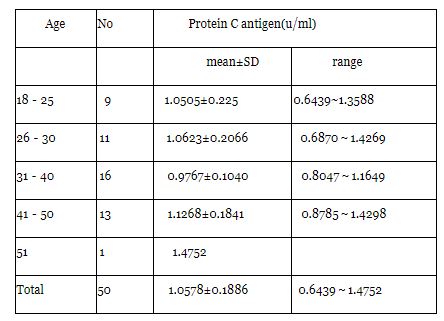
Protein C antigen was measured in the plasma of 50 healthy individuals who contributed to our pooled normal plasma. A mean protein C antigen of 1.0578 u/ml was calculated with a SD of 0.1886 u/ml; individual protein C values ranged from 0.6439 u/ml to 1.4752 u/ml.
The distribution of age on the protein C antigen concentration was evaluated in 50 healthy individuals. The results were summarized in table 1,and which indicated that no statistical differences in protein C antigen were found for the different age groups(p>0.5). Also,no difference was observed between men(mean 1.0613 u/ml) and women(mean 1.0550 u/ml).
2).Protein C antigen in distinct diseases
Diabetes Mellitus(DM)
In a group of 22 patients with diabetes mellitus(DM) an average value of protein C antigen was 1.4238 u/ml,which is considerably higher than the average value in health individuals(1.0578 u/ml). Among them,8 DM the protein C antigen level was over 1.4752 u/ml.The increased plasma protein C antigen was in turn diabetic ketoacid- osis(DKA)(n=4,1.5361 u/ml,range 1.3516~1.8434 u/ml)、diabetic angiopathy(n=5, 1.4551 u/ml,range 1.1888~2.0894 u/ml)、DM without vascular complication(n =9, 1.4403 u/ml,range 1.0834~1.8926 u/ml) and diabetic ketosis(n=4, 1.2352 u/ml,range 1.1955~1.2663 u/ml). Plasma PC:Ag level was positively correlation with urine glucose level(r=0.9581,p<0.001).
Pregnancy-Induced Hypertension Syndrome(PIHS)
In 15 pregnancy-induced hypertension syndrome(PIHS),10 severe preeclampsia the was significant increase of protein C antigen(PC:Ag) value(1.4673 u/ml,range 0.7781~2.2525 u/ml), 2 moderate PIHS the PC:Ag was normal limit range(0.7787,0.9481 u/ml respectively), whereas 3 mild patients with PIHS had decreased plasma PC:Ag level(0.5603 u/ml). Intriguing, repeat PC:Ag level was recovered to normal value (1.1455 u/ml) in one patient with PIHS after partum. Plasma protein C antigen was positively correlation with urine protein(r=0.9518, p<0.001).
Uremia
In a group of 10 uremia there were no significant changes of protein C antigen concentration when compared with normal controls(1.1387 vs 1.0578 u/ml,p>0.2)
Liver cirrhosis
19 patients with liver cirrhosis included viral liver cirrhosis 14 cases and other 1 primary biliary cirrhosis,1 scistosomal cirrhosis,1 alcoholic liver cirrhosis and 1 primary hepatocellular carcinoma, respectively. The average value of protein C antigen was 0.5501 u/ml(range:0.1436~0.9291u/ml),which was significant lower than the average normal controls(1.0578 u/ml). Moreover,13(68.4%) liver cirrhosis the protein C antigen was below the lower limit of normal control(range:0.1436~0.6188 u/ml). 14 patients with viral liver cirrhosis the protein C antigen was 0.5068 U/ml. Three severe liver cirrhosis had its the lowest value of protein C antigen 0.1436、0.1846 and 0.1919 u/ml respectively. The PC:Ag level was 1.0883 u/ml in one liver cirrhosis complicated with diabetes mellitus. Plasma PC:Ag level was positively serum albumin value(r= 0.9680, p<0.05).
Leukemias
In 20 acute leukemias,there was slightly decreased in protein C antigen level(0.9340 vs 1.0578 u/ml),but no statistical difference was found between acute leukemia and normal controls. When further analysis of acute leukemia with different cytological subtypes morphology according to FAB classification,it was shown that there was remarkably decrease of PC:Ag(0.8879 u/ml,p<0.05) in 5 M5 subtype. The decreased PC:Ag level(0.7833 u/ml) was also found in 9 hyper-leukocytes acute leukemias(WBC 23.6~280 x109/l). Intriguing,there were no significant difference in terms of protein C antigen between 3 acute promyelocytic leukemia(APL) with DIC,whereas 2 patients with infectious DIC(1 nodular panniculitis and 1 septic shock) the average value of protein C antigen was 0.2328 and 0.1646 u/ml respectively.
Protein C deficiency plasma
1 vial protein C deficient plasma which provided by RM. Bertina was measured the protein C antigen < 0.01%.
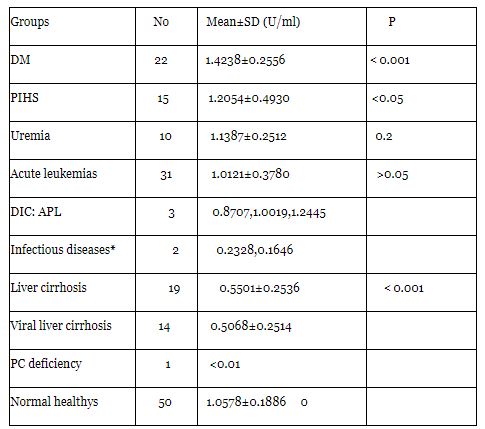
Note: DM:diabetes mellitus PIHS: Pregnancy-induced hypertension syndrome
*including 1 nodular panniculitis and 1 septic shock
This underlines the need for each laboratory to construct its own reference values for PC antigen in the laboratory determination of different methods(5,21). We set up successfully the electroimmunoassay(EIA) of the protein C antigen with the laurell method. Based on our laboratory condition,the mean PC:Ag level in 50 health individuals was 1.0578±0.1886 u/ml,which was slightly higher PC antigen levels than that of Bertina's results.
Type 2 Diabetes mellitus is characterized by vascular complication with accelerated micro and macro vascular thrombotic disease. A hypercoagulable state is appreciated in this disease. In this study,PC:Ag levels of patients especially in ketoaccidosis and diabetic angiopathy were significant higher than that of the control group(P<0.001). The results were consistent with the reports by Vigno(22) Takahashi(23),Saito(24).The decreased PC antigen was observed in type I diabetes mellitus(25,26). This may reflect the possibilty that diabetic ketoacidosis(or angiopathy) and hyper- coagulate may cause endothelial injury,which lead to elevated levels of thrombomodulin and compensatory increase the PC synthesis by hepatocytes.
Patients with the nephrotic syndrome and uremia are at increased risk of developing renal venous and arterial thromboembolism. In the measurement of PC:Ag levels in 10 uremia,there was no significant difference compared to normal controls. Cosio (27)measured the plasma concentration of protein C in 17 patients with severe proteinuria, the results was not significantly difference between the health controls and 14 patients with chronic renal insufficiency(CRI). But protein C was elevated in 71% of patients with proteinura,and was inversely correlated with serum albumin concentrations. Demaschell(28) found that PC functional activity and the antigen level were normal in 30 uremic patients before dialysis.
Our data are consistent with the previous observation. In current study,PC:Ag levels in 19 various of liver cirrhosis were significant lower than those in healthy individuals (0.5501 vs 1.0578 u/ml,p< 0.001). 68.4% of liver cirrhosis had PC:Ag level below the lower limit of normal controls. Moreover,plasma PC:Ag level was positively correlation with serum albumin. In earlier studies,Griffin(29) reported the observation that elevan of 15 patients with clinically severe liver disease(9 with positive FDP,6 with negative FDP) hss decreased plasna protein C levels. Mannucci(21,30,31) also found that in 58 chronic liver diseases protein C levels were lower than 60 health subjects,the decreased degrees roughly proportional to the severity of the disease. These findings indicated that protein C deficiencies occur the dysregulation of hepatic PC synthesis,and might play a role of predictor index in liver diseases(32).
Acute leukemias varied in PC antigen level. In this study,mean PC antigens were slightly lower than in normal in 20 patients with acute leukemia. Among FAB subtypes,the decreased PC:Ag concentrates were found in those with M5 subtype and hyperleukocytic acute leukemias. Moreover,the PC:Ag had no lower in a limited 3 patients with APL complicated by DIC,which suggested the coagulopathy in APL might be due to mechanisms different from other forms of DIC such as infectious disease(eg.septic shock)(33,34). In the recent years,for instance,the release of proteases from leukemis blasts might be responsible for the destruction of fibrinogen(factor I) and other coagulation factors(V,VII,VIII,XII,XIII), without necessarily involving an in vivo of intravascular coagulation. These results was similar to previous studies by Griffin etal(29) and Rodeghiero etal(31). The presence of 1 vial PC deficiency plasma which was provided by RM Bertina was the lower than 0.01 µ/ml, and which was consisted with the criteria of type I severe protein C deficiency. At present,some case reports and case series suggest that protein C concentrates may improve the outcome in patients with congenital(35-38) or acquired protein C deficiency(39). The use of protein C concentrates in adult septic shock(39-41) is also testable.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
