
Review Article | DOI: https://doi.org/10.31579/2690-4861/766
1 Clinic for Digestive Surgery, University Clinical Center Nis, 18000 Nis, Serbia.
2 Internal Medicine Clinic, University Clinical Center Nis, 18000 Nis, Serbia.
*Corresponding Author: Ilija Golubovic, Clinic for Digestive Surgery, University Clinical Center Nis, 18000 Nis, bul. dr Zorana Djindjica 48, 18000 Nis, Republic of Serbia.
Citation: Ilija Golubović, Goran Stanojević, Aleksandar Vukadinovic, Marko Stojanovic, (2025), Complete Mesocolic Excision for the Treatment of Right-Sided Colon Cancer: Anatomical Consideration, Surgical Technique and Outcomes, International Journal of Clinical Case Reports and Reviews, 25(3); DOI:10.31579/2690-4861/766
Copyright: © 2025, Ilija Golubovic. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 March 2025 | Accepted: 08 April 2025 | Published: 17 April 2025
Keywords: complete mesocolic excision (CME); right-sided colon cancer; anatomy; surgical technique; outcomes
Since total mesorectal excision (TME) reduces local recurrence rates, it is considered the gold standard surgical procedure for treating locally advanced rectal cancer. These discoveries led to the use of the dissection principle in colon cancer surgery using complete mesocolic excision (CME) and central vascular ligation (CVL). A successful CME operation encompasses three critical components: the specimen must be removed in the mesocolic plane, the supplying blood vessels should be ligated at their origin, and an adequate length of the colon must be removed. Education and comprehensive knowledge of vessel anatomy are essential; otherwise, there is a risk of increased morbidity. CME implementation began with the aim of developing a new concept for colon cancer surgery that would improve patient outcomes. This operation yields high-quality specimens that may suggest better long-term oncologic outcomes, although the morbidity associated with CME is typically higher than that of standard right hemicolectomy. To date, published series on CME are predominantly retrospective and heterogeneous. As a consequence, the analysis of oncological findings should be approached with caution. Evidence regarding the quality is insufficient and does not consistently demonstrate the superiority of CME.
Colorectal cancer (CRC), also known as colorectal adenocarcinoma, is increasingly widespread in developing countries and is currently the third particularly high cause of cancer mortality globally, accounting for 11% of all cancer diagnoses. Cancer of the colon is the fourth most incident, while cancer of the rectum is the eighth most incident cancer in the world [1]. GLOBOCAN 2018 estimates around 1,096,000 new cases of colon cancer detected in 2018 [2].
Using a new approach to rectal cancer using total mesorectal excision (TME) techniques, first described in 1979 by Professor Richard J. Heald, has led to changes in the rectal cancer surgery also affected outcomes [3]. Thus, with the application of TME, a higher probability for clean circumferential margin is achieved [4], with a marked decrease in local recurrence rates from 30%-40% to 5%-15%, and on the other hand, the rate of survival after five years has risen from 45%-50% to 75% [5, 6].
The surgical principles of TME, Hohenberger et al. applied for the surgery of colon cancer through complete mesocolic excision (CME) and central ligation [7, 8]. This approach focuses on the a separation of the mesocolic from the parietal plane and the central vascular ligation (CVL) of the supplying arteries and draining veins, performed as near as feasible to their junction with the mesenteric vasculature. CME has also been shown to improve survival and local recurrence rates as compared to conventional colon cancer surgery, according to several authors. The majority of these studies are retrospective cohort a series arrangement, and several lack a comparison group [9-13]. However, CME concepts have not been widely accepted [14], and colon cancer survival rates have now declined behind those of rectal cancer [15].
Furthermore, it is also important to emphasize that previously published studies demonstrated a correlation between gender and age, revealing a higher incidence of right-sided colon cancers (RSCCs) in women and older individuals [16, 17]. Patients with right-sided and left-sided colon cancer (LSCC) exhibit variations in epidemiology, perioperative evolution, histology, survival rates [18, 19], and molecular biology pathways [20].
Consequently, it has been proposed to regard CRC as three different tumor entities: RSCC, LSCC, and rectal cancer. Right-sided cancers are typically characterized as malignancies occurring proximal to the splenic flexure, whereas left-sided cancers are situated distal to the splenic flexure. A large corpus of literature exists [8-13] that recognises the importance of complete mesocolic excision for colon cancer and which ask the question: Is this the appropriate moment for a transformation in practice? We aim to describe anatomical background as well as The approach and outcomes of the CME technique for the treatment of RSCC.
Anatomical consideration
Sir Frederick Treves' observations in 1885 led to the classical anatomical classification of the mesocolon. Treves researched the anatomy of the human intestinal canal, peritoneum, and mesentery. He reported a case collection of 100 cadaveric surgical dissections to the Royal College of Surgeons in England, observing that roughly fifty percent of the cadavers examined lacked an ascending or descending mesocolon. Carl Toldt notably recognized the persistence of the mesocolon into adulthood in 1879, some years before to Treves. In 1879, he published his study of the anatomy and development of the human mesentery. Toldt also identified a specific fascial plane between the mesocolon and the underlying retroperitoneum, formed by the fusion of the mesocolon's visceral peritoneum with the retroperitoneum's parietal peritoneum (Toldt's fascia) [21, 22].
In order to explain CME, it is important to consider the anatomical properties of the mesocolon. Regarding the anatomical background of CME it is important to point out that CME involves tissue mobilization through the release of planes during dissection between the parietal and mesenteric fasciae. This avascular space is formed during the secondary attachment of the parietal and visceral fascia and it can be divided by surgery through sharp dissection [23]. Furthermore, it is important to distinguish the following terms [5, 24] defined in Table 1.
| Terms | Definition |
| Toldt’s Fascia | An extra fascial plane between the mesocolon and retroperitoneum |
| Colo-fascial interface | Confluence of colonic surface and Toldt’s Fascia |
| Meso-fascial interface | Confluence of mesocolon and Toldt’s Fascia |
| Retro-fascial interface | Confluence of retroperitoneum and Toldt’s Fascia |
Table 1: Definition of anatomical terms for better understanding of CME
To carry out CME for right colon malignancies within the appropriate anatomical planes, vascular anatomy should be thoroughly studied beforehand. The SMA contains two or three principal branches that give arterial blood to the right colon. In many cases, the right colic artery (RCA) is not an anatomical constant. The ascending colon is usually supplied by the right branch of the middle colic artery (MCA). An accessory MCA exists in 11.7%. In 100% of cases, the ileocolic artery (ICA) and MCAs are constant vessels arising from the SMA[25, 26]. The most significant of these branches is the ICA. The ICA may encircle the superior mesenteric vein (SMV) or lie underneath the ileocolic vein (ICV). This is a large difference that must be taken into account during the central vessel ligation procedure [23, 7].
To prevent vascular complications during CME, it is important be familiar with the venous architecture of the right colon and its variations. The venous blood from the cecum, ascending colon, and the right portion of the transverse colon drains into the SMV. However, there are various differences in the topographical anatomy of the right colic vein (RCV), superior RCV, gastrocolic trunk, and middle colic vein (MCV) [27, 28]. The RCV, the gastroepiploic vein, and the pancreatic veins do not routinely drain into the SMV separately. Their drainage is most generally provided by a common vein, the trunk of Henle, which is found in approximately 88 percent of all cases [26, 29]. The research conducted by Miyazawa et al. (2015) [30] revealed variations of the colic drainage veins entering the gastrocolic trunk of Henle, as identified using three-dimensional multidetector computed tomography: Type 0 is represented with right gastroepiploic vein (RGEV), and anterior superior pancreaticoduodenal vein (ASPDV); Type I is represented with RGEV + ASPDV + superior right colic vein (SRCV); Type II is represented with RGEV + ASPDV + SRCV + RCV or MCV; and Type III is represented with RGEV + ASPDV + SRCV + RCV + MCV. The drainage of these veins through the trunk of Henle or directly in the SMV underpins a difference that surgeons must consider when mobilizing the hepatic flexure of the colon. When attempting proper central vascular ligation, surgeons need to have a comprehensive understanding of the vasculature and any variations that may exist. Whit correct central vessel ligation, the extraction of the core portion of the tumor-draining lymph nodes is facilitated. This is important because it will affect the prognosis of the patients [7].
Surgical technique of CME
In our paper, only open and laparoscopic surgery in relation to CME will be presented, considering that robotic-assisted CME is a promising and safe minimally invasive procedure, as indicated by recent studies [31, 32].
Open surgery
A “lateral-to-medial” approach is generally performed in open surgery. In RSCCs, recognizing the avascular space between the parietal and mesenteric fasciae is crucial for dissection [33-35]. Toldt’s fascia defined as a single fascial layer separates mesocolon from retroperitoneum. Deviation from this dissection can lead to bleeding and even to damage of retroperitoneal structures. The dissection proceeds medially within the mesofascial interface. The dissection is thereafter conducted over the duodenum and pancreatic uncinate process to facilitate access to the superior mesenteric vein and artery [36]. At this point in time duodenal kocherization is not typically conducted [8]. Thus applying the dissection pathway medially the small intestinal mesentery, ileocecal junction, right colon, right mesocolon and mesenteric confluence are fully mobilized. It is important to emphasize that care must be taken to identify and preserve the autonomic nervous plexus [36].
The anatomy and its variations can be precisely identified by incising the peritoneum surrounding the vessels. Additionally, the central ligation of the ileocolic and right colic vessels—when present, as the RCA occurs in fewer than fifty percent of cases—at their origin from the superior mesenteric vessels ensures the retrieval of all lymph nodes draining the tumor.
The dissection is then performed centrally along the SMA, enabling removal of all associated lymph nodes [36]. The right branch of the middle colic vessels is divided [8, 36, 38] for cecal and ascending colon cancers after it is entered the lesser sac. Access to the lesser sac is achieved by transecting the right gastroepiploic artery for neoplasms found in the hepatic flexure or proximal transverse colon. To access the peripancreatic lymph nodes it is necessary mainly to divide the right gastro-epiploic artery at its origin [8, 36]. Lymph nodes located at the inferior border of the left pancreas and those along the left gastroepiploic arcade may be excised for colon tumors positioned to the left of the MCA [39].
Additionally, the MCV is divided at its junction with either the SMV or the gastrocolic trunk (trunk of Henle), whereas the MCA is divided at its origin from the SMA [8, 34, 36, 38]. At the level of the middle colic vessels [8], the colon is divided. For hepatic flexure cancers, the colon is divided near to the splenic flexure [8]. It is important to keep in mind that the veins draining into the gastrocolic trunk show a variability. The tiny veins around the trunk of Henle may rupture, resulting in significant hemorrhage; thus, caution is essential during dissection (Table 1). Given that during right-sided CME usually only the RCV needs to be cut, it is important to approach it carefully to the RCV, the RGEV, and the anterior pancreatic veins that can drain to the trunk of Henle or communicate separately to the SMV.
Laparoscopic surgery
CME can be performed laparoscopically with comparable quality to open operations [40]. A “medial-to-lateral” approach is preferable. In very unusual circumstances, a lateral-to-medial approach can be used. In right hemicolectomy, the mesocolon is incised along the mesenteric axis next to the SMV. Further, right colon vessels (ICV, ileocecal vein; ICA, ileocecal artery; RCV; RCA) are ligated at their origin. The gastrocolic trunk of Henle is then exposed by dissection along the superior mesenteric vein[40].
The MCA is recognized as arising from the SMA and diverging near the base of its right branch. Lymph node dissection is thereafter performed, preserving the left branch of the main colic artery. Simultaneously, the MCV is identified and transected near the origin of its right branch. In cases with cecum or ascending colon malignancies, the right branch of the middle colic vessels is ligated at its root, and the transverse colon is transected at the level of the middle colic vessels. In cases of proximal transverse colon or hepatic flexure malignancies, the middle colic and right gastroepiploic vessels are ligated at their root [7, 35].
After that, the right side of the greater omentum is dissected using anterior-to-median approach. Between the omentum and the transverse mesocolon, the fusion fascia is detached, and the hepatic flexure is mobilized [41]. The accessory MCVs are meticulously dissected, and lymph nodes are dissected as well. The transverse mesocolon is dissected beneath the inferior margin of the pancreas, revealing the SMV. The specimen is obtained by a mini-laparotomy, and the anastomotic approach (intracorporeal or extracorporeal) is contingent upon the surgeon's expertise and preference [7, 11, 40, 41].
The use of laparoscopic surgery to treat colon cancer near the flexures and in the transverse colon is also debatable. The open approach is the preferred procedure for these tumors in many hospitals [42].
Outcomes of CME in the literature
Two models have been suggested in the past to describe epithelial cancer nodal distribution. In Halsted's initial stepwise model, nodal metastasis occurs both temporally and spatially prior to distant dissemination. If this scenario is true, eliminating as many (possibly) invaded nodes as possible can avoid further tumor spread and result in a survival advantage. Fisher's parallel distribution model assumes that distant metastasis occurs very early in the disease. This model regards lymph node metastasis as a marker of the disease's biological activity and malignancy, asserting that the excision of infected nodes does not influence survival outcomes [43-45].
Willaert et al. (2015) demonstrated that factors such as circulating tumor cells in peripheral blood, growth rates of primary colon cancer and liver metastases, early dissemination, and information regarding the quantity and location of invaded lymph nodes and their prognostic implications indicate that the lymphatic spread of colon cancer is an unpredictable event rather than a phased one, potentially occurring early in tumor progression. Surgical attempts at optimal nodal clearance are unlikely to influence the probability of systemic dissemination. Consequently, the future of surgical oncology is oriented towards more precise, imaging-guided, less invasive, and less traumatic surgical techniques, integrated within the context of multiple modalities guided by the latest advancements in cancer biology [45].
Furthermore, colon cancer surgical resection was graded by the colonic grading system as being in the muscularis propria plane (“poor” plane of surgery), intramesocolic plane (“moderate” plane of surgery), or mesocolic plane (“good” plane of surgery) (Figure 1 and 2). A fourth category was subsequently built up when surgery is performed in the mesocolic plane with a high vascular tie near to the aorta. This method of intensive surgery is designed to remove the entire colonic mesentery, including all possible nodal and intravascular tumor spread sites [46].

Figure 1: Pathology grading of colon cancer surgical resection: Intramesocolic plane (“moderate” plane of surgery—moderate bulk to mesocolon with irregularity but the incisions do not reach down to the muscularis propria)

Figure 2: Pathology grading of colon cancer surgical resection: Mesocolic plane (“good” plane of surgery— intact mesocolon with a smooth peritoneal-lined surface)
Given all of these variables and the lack of data from prospective randomized studies with relevant clinical outcomes, CME should be regarded as investigational; therefore in our study three types of outcomes were of interest: The safety of CME, the quality of CME as well as oncological outcomes.
There is a large volume of published studies comparing CME and non-CME. It was found CME demonstrated superior survival rates despite being linked to an a higher rate of complications [47, 48]. Recent research indicates that laparoscopic CME with D3 lymph node dissection is a safe and feasible surgical alternative for right colon cancer in older individuals [49]. In an analysis of anastomotic leak, Prevost et al. (2018) found no significant difference in the rate of anastomotic leak (1.2% in the conventional versus 5.6% in the CME/CVL group). The study indicated a propensity for delayed gastric emptying in the CME/CVL group [50]. It has been demonstrated that application of CME results in reduction of locoregional recurrence from 6.7% to 2.1% for all stages; distant organ metastatic rate decreased from 18.9% to 13.3% [51]. Furthermore, CME was associated with a longer colonic resection, and more lymph nodes [9, 52, 53].
However, all of these series encompass results for both right and left colon cancer. Several recent studies have compared CME and non-CME outcomes for RSC.
According to a research by Bertelsen and colleagues [54] the 5-year results for patients with potentially curable stage I–III colon cancer show a significant reduction in recurrence to 9,7% in the CME group compared to 17,9% in the non-CME group. In a study which set out to determine the safety of CME, Bertelsen (2018) observed that complete mesocolic excision did not correlate with an elevated risk of diarrhea or diminished quality of life (55).
Furthermore, the study by Rasulov et al. (2017) demonstrated that there was no postoperative mortality following complete mesocolic excision for right colon cancer, with 17 procedures conducted via open technique and 22 via laparoscopic method. The study reported a median
intraoperative blood loss of 30 ml (range 30-300 ml) for the laparoscopic technique and 300 ml (range 30-500 ml) for the open approach. The median number of excised lymph nodes was 35.7 (range 6-68), whereas the median number of metastatic lymph nodes was 1.9 (range 0-16) [56].
Vajda et al. (2020) [57] examined a cohort of 156 consecutive patients who underwent surgery for malignant RSCC between September 1, 2016, and June 30, 2019. There were 84 laparoscopic procedures and 59 open surgeries conducted. The mean specimen length was 22.34 cm for conventional surgery and 24.97 cm for CME surgery, whereas the average number of lymph nodes was 15.4 and 16.9, respectively (p = 0.24). Preliminary data suggest that the procedure may be conducted laparoscopically, yielding outcomes comparable to open surgery, but with a reduced period of hospital stay [57].
Similar results in their study are presented by Zedan et al. (2021) comparing laparoscopic versus open complete mesocolic excision for right colon cancer [58]. The authors determined that with experienced surgeons, laparoscopic CME right hemicolectomy is a feasible and safe treatment, with long-term oncologic outcomes (recurrence and survival) comparable to open surgery for patients with stage II or III colon cancer. Additionally, the study by Huang et al. (2015) retrospectively assessed the clinical data of 102 patients who underwent right colon resection. The operative time in the laparoscopic surgery (LS) group was similar to that in the open surgery (OS) group, while intraoperative blood loss fell significantly in the LS group when compared to the OS group. In their study, there was no difference in the total number of harvested lymph nodes between the groups and length of hospital stay were significantly shorter in the LS group. It was also shown in their study that the rate of complications was similar between the groups with no recurrences in either group during follow-up (range, 6-24 months). Overall, they determined that laparoscopic CME is a safe, practical, and effective minimally invasive technique for right colon cancer [59].
Some of the studies from the literature gave an overview of disease-free survival and overall survival rates for right colon cancer (CME with CVL), which we show in Table 2.
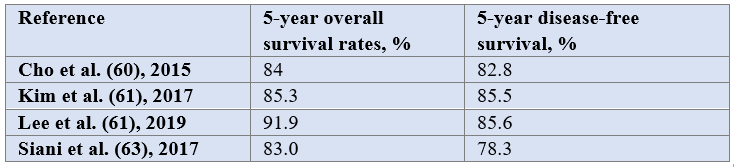
Table 2: Disease-free survival and overall survival rates for right colon cancer (CME with CVL)
Nevertheless, several studies demonstrate significant limitations, predominantly being retrospective and heterogeneous, which complicates determining of a definitive high level of evidence at this point in time, precluding the assignment of a robust grade of recommendation. These data emphasize the necessity for prospective randomized trials with large cohorts to establish CME as the gold standard for right colon cancer resection.
Taken together, these studies suggest that the morbidity associated with CME can usually be higher than that of standard right hemicolectomy. CME requires comprehensive anatomical knowledge and oncological colon surgery experience. The CME with CVL provides high-quality specimen that can indicate favorable prolonged oncological results. To date, published series on CME are predominantly retrospective and heterogeneous. As a consequence, the analysis of oncological findings should be approached with caution. The evidence quality is inadequate and does not consistently endorse the superiority of CME.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
