
Review Article | DOI: https://doi.org/10.31579/2693-4787/030
Department of Medical Biology, Meram Faculty of Medicine, Necmettin Erbakan University, Konya, Turkey.
*Corresponding Author: Hasibe Vural, Department of Medical Biology, Meram Faculty of Medicine, Necmettin Erbakan University, Konya, Turkey.
Citation: H Vural. (2022). Are anti-CTL4 and anti-PD-1 an effective biomarker in immunotherapy?. Clinical Oncology Research and Reports. 3(1); Doi:10.31579/2693-4787/030
Copyright: © 2022 Hasibe Vural, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium provided the original author and source are credited.
Received: 12 October 2021 | Accepted: 29 December 2021 | Published: 06 January 2022
Keywords: cancer; immunotherapy; CTLA-4; PD-1
The task of the immune system is to prevent foreign organisms from entering the body, if microbes have entered the body, to destroy them, to prevent or delay their spread. One of the most important features of the immune system is that it has the ability to recognize and distinguish millions of different microbes that are foreign to it. The immune system, like the brain, evaluates and synthesizes the situation, which is this breeding organ, and produces different training and special responses to microbes, cancer. This is a feature that does not exist in any system or organ except the brain and immune system. In summary, the task of the immune system is to protect the essence of the individual. For this reason, he knows himself first and does not harm the essence. In this context, it can be said that the immune system spends as much effort on self-knowledge as it does on fighting the enemy.
This rewiev article is intended to provide an overview of the CTLA-4 and PD-1 pathways and the description of their efficacy in cancer therapy or immunotherapy.
Immunotherapy, which started with the treatment of melanoma, a type of skin cancer, after years of chemotherapy and targeted smart drugs, is currently being used as a treatment method in more than 20 cancer types abroad. With immunotherapy, the person's immune system is activated and the person's own immune system cells are provided to fight cancer cells more effectively. The aim of cancer immunotherapy is to create an effective anticancer response by increasing the activity of the immune system. Although there are many different types of immunotherapies such as cell and vaccine treatments, in our country, when it comes to immunotherapy, it is perceived as "Check Point Inhibitors". In our country, there are repayments of immunotherapies in three types of cancer called kidney cancer, melanoma and hodgkin lymphoma.
Macro applications, which are among the elements of the immune system, are produced by NK and active uses such as T are used for their own possibilities. Some of the commonly used treatment methods can be listed as follows:
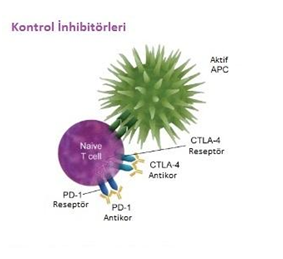
Immune Checkpoint inhibitors (Checkpoint inhibitor)
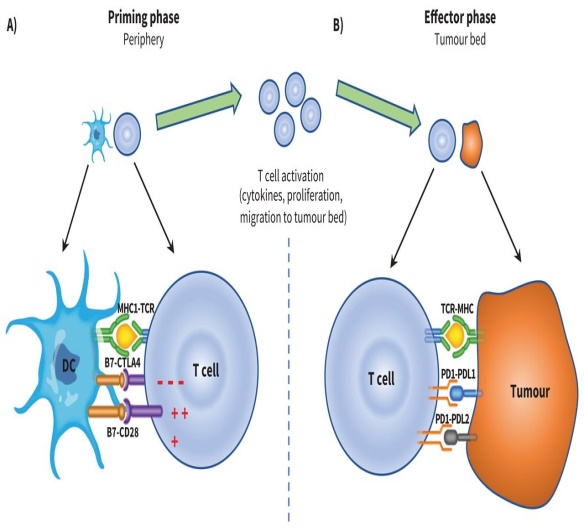
Today, they are drugs that provide dramatic improvement in many cancers and their use is becoming increasingly common. These special molecules eliminate the natural brake mechanism in the immune system, enabling the activation of T cells that recognize and attack the cancerous cell. In other words, these molecules act by blocking 'checkpoint proteins' that stop the immune system from attacking the cancerous cell. Immune checkpoint inhibitors (ICIs) offer effective treatments for an ever-growing array of advanced malignancies. The mechanism of action of ICIs is the coordination of innate and adaptive immune systems, including the blockade of cytotoxic T-lymphocyte antigen-4 (CTLA-4), programmed cell death receptor-1 (PD-1), and PD ligand-1 (PD-L1) reflects. The researchers noted that this blockade increases the activity of T cell lymphocytes to attack cancer cells.Immune checkpoint inhibitors (ICI) are effective on cancer as a result of the elimination of pressures on the immune system, however, overactivity of the immune system is one of the main causes of many autoimmune diseases. Today, reducing the side effects of ICIs or developing antibodies that will cause less side effects is an active research topic. Compared to conventional cancer treatments, immunotherapy can help the patient lead a cancer-free life for many years, but according to clinical studies, ICIs are not effective in all patients who use them. Knowing which users will benefit from it will be used in CTLA-4 to benefit from a project like the PD-1. These checkpoints, in particular, are critical for the environment. Immunotherapy plans to combat this immune control score by restoring and improving reevaluability for blocking. Particularly prominent checkpoints are CTLA-4 and PD-1/PD-L1, against which monoclonal antibodies have been developed. Inhibition or suppression of these targets leads to increased activation of the immune system. PD-1 and CTLA-4 differ greatly in inhibiting immune responses, including antitumor responses. For example, CTLA-4 is known to regulate T cell proliferation.Immunotherapies with antibodies targeting immune checkpoints, such as cytotoxic T-lymphocyte antigen-4 (CTLA-4) or programmed death-1 (PD-1)/PD-1 ligand (PD-L1), did not respond well in the majority of cancers. Cancers express transforming growth factor beta (TGFbeta), which often drives immune dysfunction in the tumor microenvironment by stimulating regulatory T cells and inhibiting CD8+ and TH1 cells.Immune checkpoint is a kind of signal to regulate antigen recognition of T cell receptor (TCR) in the immune response process. The immune checkpoint contains two types of signals:• Co-stimulatory immune checkpoint: stimulating immune progression such as CD28, ICOS and CD137,• Co-inhibitory immune checkpoint: inhibiting immune progression such as PD1, CTLA-4 and VISTA.As the immune system attacks pathogens, these immune checkpoint molecules can protect normal tissues from damage.
Cancer cells cleverly evade immune attack by dysregulating immune checkpoint-related proteins. Immune checkpoint therapy relies on the functioning of the immune system with agonists of co-stimulatory signals or antagonists of inhibitory signals.
There are two immune checkpoint receptors that have been actively studied over these years: Cytotoxic T-lymphocyte-associated antigen 4 (also known as CTLA4; CD152) and programmed cell death protein 1 (PD1; also known as CD279). Corresponding antibodies can inhibit the functioning of receptors and increase antitumor immunity.
Also, a large number of additional immune checkpoints that represent promising targets for anti-cancer therapy are under active development, with more immune checkpoint-based treatments coming to market for more cancers.
Immune Checkpoint Therapy in Cancer Patients;
Immune checkpoints are a key target of cancer immunotherapy. In cancer cells, these checkpoints can be up- or down-regulated depending on their role in activating or inhibiting the immune response.
CTLA-4 is an immune checkpoint that is upregulated in many cancers. It is present in regulatory T cells after activation and plays a role in the inhibition of the immune response. Immune system checkpoints, which include the signaling pathway, are very important in preventing tissue damage that may develop due to the natural immune response to pathogenic infection and in the development of self-tolerance of the body that is, in controling or regulating the development of autoimmunity. The first clinically targeted immune checkpoint is CTLA4.
Inhibitory stimuli from immune checkpoints are a homeostasis mechanism. Currently, studies have focused on the CTLA-4 (Cytotoxic T-lymphocyte-associated Antigen 4) and Programmed Death-1 (PD-1) pathway. Programmed cell death (PD)-1 and programmed cell death ligand (PDL-1) pathway are checkpoint PD1/PDL-1 pathway; It inhibits proliferation, survival and effector function, including cytokine production of T cells, and plays a role in the escape of tumor cells from the immune system.
PD-1 has two ligands, PD-L1 and PD-L2. In order for PD-1 to inhibit T lymphocyte functions, it must be combined with PD-L1 and PD-L2 ligands. The ligand mostly found in tumor cells is PD-L1. PD-L1 expressed in the tumor microenvironment suppresses the immune response to the tumor.
In mouse models, it has been shown that increased expression of PD-L1 on the tumor cell surface inhibits the immune response against the tumor in the tumor microenvironment, so that tumor cells can escape from the immune system and proliferate. PD-1 ligand distribution on cell surfaces of different tumors shows heterogeneity.
One of the main interaction points between cancer cells and the immune system is PD-1/PD-L1. Programmed death protein 1 (PD-1) and its ligand (PDL-1) have been recognized as inhibitory molecules that cause disruption of the immune response against cancer cells
[1, 2, 3]. The PD-1 (Programmed cell death-1) receptor is located on the surface of active T and B lymphocytes. Studies have shown that PD-L1 (Programmed cell death ligand-1) is found in many different tumor types [4, 5].
In line with these data, various agents have been developed that inhibit the PD-1/PD-L1 interaction in cancer cells. These agents, which have strong effects such as long-term survival with minimal toxicity, have been a hope for many cancer patients and researchers. Accordingly, there are currently 11 PD-1 or PD-L1 antibodies, 5 of which are FDA approved. When it binds to the Programmed Cell Death-1 (PD-1) receptor specific ligand, Programmed Cell Death-1 (PD-L1), it causes predominantly negative regulation of the effector function of T cells. This also occurs in tumor cells [6, 7, 8, 9, 10]. The PD-1 receptor has two ligands. PD-1L is also known as CD274 or B7-H1 and is expressed by somatic cells exposed to pro-inflammatory cytokines. PD-L2, also known as CD273 or B7-DC, has a more limited expression on antigen presenting cells [11, 12, 13]. Increased PD-L1 expression due to inflammation in the tumor microenvironment causes depletion of PD-1-mediated T cells, preventing the formation of the antitumor T cell response [13, 14]. Antitumor T cells repeatedly recognize congnate tumor antigens during the progression of cancer from primary to metastatic lesions. Triggering T cell receptors (TCR) results in the production of proinflammatory cytokines, including interferon G, the most potent stimulator of PD-L1 expression [15, 16 17].
Immune checkpoint regulation has been heavily researched over the past decade. However, the underlying mechanisms regulating PD1 and PD-L1 expression are not fully understood. However, several oncogenic signaling pathways, epigenetic alterations, and genetic variations have been proposed for this regulation [1, 2]. Immunotherapy, which has been proven to be effective in many types of cancer in recent years and has started to be used in the treatment, is also a promising example for the treatment of glioblastoma.The PD-1/PD-L1 checkpoint, which is one of the current immunotherapeutic targets, has been blocked with monoclonal antibodies in many cancer types, and successful results have been obtained in making cancer cells the target of T cells.Especially when there is resistance to PD-1 or PD-L1 targeted drugs, using these drugs together with anti-CTLA4 agents or some cancer vaccines that will increase PD-1, PD-L1 sensitivity or with messengers that stimulate cells (IFN-gamma) such as GM-CSF; or as a different strategy, there are many studies in progress on treatments with genetically engineered T cell sensors (TCR or CAR) against cancer cells [18, 19, 20].
Immunotherapy, which has developed with the field of immunogenetics, aims to detect and find solutions in cases where genetic mutations cause the immune system to be functionally defective.
Immunogenetics refers to the scientific discipline that studies the molecular and genetic basis of the immune response. Genetic conditions that affect the development or function of components of the immune system lead to uncontrollability of infectious pathogens or susceptibility to autoimmunity or cancer.
Immune checkpoints are very promising and are a recently developed cancer treatment. Here, I tried to describe the PD-1/PD-L1 and CLTA-4 immune checkpoints and their effectiveness in monoclonal antibody detection and the importance of immunotherapy. Given the interaction of the tumor microenvironment with normal cells and the increasing incidence of cancer, there is an urgent need to improve existing therapies and develop new alternatives worldwide. Current immune checkpoint blocking therapies target receptor-ligand interaction. This approaches show that modulation of intracellular and cell surface receptor-ligand signaling stimulates antitumor immunity.In this sense, immunotherapy is the most effective way. Ongoing OMIC technologies and epigenetic analyzes are expected to provide invaluable new insights on this topic.
Hıghlıghts
Immunotherapy, a new way to treat cancer groundbreaking to detect tumor types and reduce the patient rate. Biological mechanisms need to be investigated. In this context known anti-CTLA4 mechanisms and it is necessary to know anti-PD-1 immune checkpoint inhibitors very well. Because there is a close relationship between tumor development, differentiation and proliferation of cancer cells, necrotic formation and immunogenetics.
We researchers recognize that the field of immuno-oncology is complex. In particular, I would like to emphasize that the field of immunogenetics is extremely important for the whole scientific world to better understand the relationship between the immune system, tumor biology and tumor microenvironment.
Regulatory mechanisms of PD-L1 are generally effective at the PD-L1 expression, RNA level (inflammatory signaling, abnormal oncogenic signaling, miRNA regulation, epigenetic regulation, mRNA stabilization), while at the DNA level (genomic modification, epigenetic regulation) and protein level (each localization, phosphorylation, glycosylation etc.) are effective.
The suppressive functions of immune checkpoints are generally provided by ligand-induced signaling. Here, I have tried to briefly describe the ligand interaction and signaling mechanism of two well-studied immune checkpoints.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
