
Case Report | DOI: https://doi.org/10.31579/2693-2156/053
Department of Anesthesiology, Zhongshan City People’s Hospital, Zhongshan, China.
*Corresponding Author: Xiaozu Liao, Binfei Li, Department of Anesthesiology, Zhongshan City People’s Hospital, Zhongshan, China.
Citation: Xiaozu Liao, Miaoyun Guo, Shi Zhong, Junlin Wen, Binfei Li (2023), Application of Myocardial Contrast-Enhanced Ultrasound in Heart Transplantation in Patients with Acute Myocardial Infarction:A Case Report, J Thoracic Disease and Cardiothoracic Surgery, 4(2); DOI:10.31579/2693-2156/053
Copyright: © 2023, Xiaozu Liao. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 March 2023 | Accepted: 06 April 2023 | Published: 17 April 2023
Keywords: mce; ecmo; heart transplantation
Background: MCE is a safe and effective myocardial perfusion assessment technique; it is used for the assessment of post MI viability.
Case Presentation: A 52-year-old male with cardiogenic shock caused by secondary acute myocardial infarction and successful coronary stent implantation with ECMO, IABP and ventilator assistance and with no significant recovery of postoperative cardiac function. The result of MCE was also reported. The allograft was successfully performed 8 days after ECMO-assisted support. The patient was successfully transferred to the general ward 8 days after surgery and successfully discharged on day 86 of admission.
Conclusions: ECMO provides effective mechanical assistance support for patients with end-stage heart failure, buys time for heart transplantation surgery, and was an effective cardiopulmonary support treatment. An evaluation of myocardial perfusion and survival quantity was an important reference for emergency heart transplantation.
The mortality rate in patients with cardiogenic shock due to acute myocardial infarction is up to 50% [1]. In patients with refractory cardiogenic shock, Extracorporeal membrane oxygenation (ECMO) provides hemodynamic support to reduce secondary organ damage and for early revascularisation to rescue the myocardium with ECMO assistance, thereby improving patient survival [2]. However, although some patients underwent revascularisation, cardiac function was still severely impaired and even separated from ECMO,he patients needed heart transplantation. Therefore, when patients have been assisted with ECMO for a long time, evaluating their myocardial functional status to determine the indications for performing heart transplantation is needed. Myocardial contrast echocardiography evaluation (MCE) is a safe and effective myocardial perfusion assessment technique; it is used for the assessment of post myocardial infarction(MI) viability [3]. In this report, a patient with cardiac shock caused by secondary acute myocardial infarction successfully underwent coronary stent implantation assisted by ECMO and ventilator with no significant recovery of postoperative cardiac function. The end-stage cardiac failure and successful heart transplantation diagnosed by combined MCE was reported.
The patient is a 52-year-old male who was admitted to the hospital. He presented with chest distress for 2 years and another half-hour episode with psychiatric change. Results of physical examination after admission showed the following: blurred mind, passive position, thick breathing in both lungs, dry and wet rales, Heart rate 96 beats per minute, and blood pressure of 63/43 mmHg; N-terminal pro brain natriuretic peptide (NT-pro BNP): 2,425 (pg/ml); Highly sensitive troponin T (TnT-HS): 10,000 (ng/L); Creatine kinase (CK): 14,147 (U/L); And creatine kinase isoenzyme (CK-MB): 587 (U/L). ECG showed that: sinus tachycardia and acute anterior and lateral myocardial infarction (Figure 1).

Figure 1: ECG change at disease onset (acute inferior wall and posterior wall myocardial infarction ECG change; old and extensive anterior wall infarction ECG change)
Cardiac colour ultrasound indicated that the left ventricular wall activity was generally weakened. The following were observed: left atrial and LV enlargement, incomplete mitral valve closure (mild-moderate) and ejection fraction EF: 0.18. So the patient was diagnosed acute myocardial infarction and cardiogenic shock . The patient was given a 0.2 ug/kg.min dose of adrenaline and norepinephrine at 0.2 ug/kg.min to Pump injection. The blood pressure was 63/43 mmHg. The lactate was 6 mmol/L. The patient’s limbs were wet and cold, and he was unconscious. The patient was intubated and mechanically ventilation, then he was immediately given ECMO assistance.
In venous-arterial ECMO oxygenation (V-A ECMO) mode, the right femoral artery-venous catheterisation was performed, and the following were used: systemic heparin sodium (1 mg/kg), 17Fr femoral arterial catheter (Medtronic) with a depth of 15 cm and 21Fr femoral venous catheter (Medtronic) with a depth of 45 cm. An 8Fr end-end reperfusion catheter was inserted to prevent ischemia of the lower limbs. After the ECMO establishment was completed, we ran the ECMO perfusion system (Medtronic) with a flow rate of 3.5 L/min and MAP of 80 mm Hg. The ECMO was fully established, and the patient underwent interventional therapy.
The patient had acute myocardial infarction 2 years ago, the coronary angiography showed that: about 40%–50% left trunk stenosis, anterior descending branch opening-proximal stenosis, recent acute occlusion and distal flow grade TIMI 0; and about 40%–60% distal branch stenosis, about 50%–70% OM opening-proximal stenosis and distal flow grade TIMI (Figure 2).

Figure 2: 2 years ago, coronary angiography (Figure a: 40%–50% left trunk stenosis, anterior descending opening-proximal stenosis, immediate acute occlusion, distal flow grade TIMI 0; about 40%–60%, 50%–70% OM opening-proximal stenosis, distal flow grade TIMI 3. Figure b: Angiography after coronary artery vessel treatment.)
Descending stenting and IABP implantation were performed, and the patient was successfully discharged 30 days later. In this operation, the coronary angiography showed that: the left main trunk, three vessel lesions and the cyclotron branch were acute occlusion, stent implantation and IABP implantation. The operation process was smooth (see Figure 3).
Figure 3: Coronary angiography after onset in this patient (Figure a: left coronary angiography: left trunk-anterior descending open implanted stent patency, without significant intimal hyperplasia. Middle-distal slender, blood flow grade TIMI 3. The middle section of the spiral branch was acutely blocked, with no forward flow, blood flow grade TIMI 0. Figure b: Angiography after coronary artery vessel treatment.)
After surgery, he was transferred to the intensive care unit for fluid expansion, and the infusion of red blood cells was performed to improve anaemia. The infusion of blood products and other blood products was performed to improve coagulation function, piperacillin tazobactam sodium anti-infection and haemostasis.
After 7 days of ECMO-assisted support and active treatment, the patient showed no significant recovery of cardiac function. After re-examination of NT-proBNP: 33553 (pg/ml), chest X-ray indicated that the texture of both lungs was slightly thickened and blurred, the heart shadow was enlarged. Cardiac insufficiency was considered. Cardiac colour ultrasound suggested the following: weak left ventricular wall activity, left atrial and left ventricular enlargement, mild mitral valve closure, poor left ventricular systolic function and ejection fraction EF of 0.19. Mechanical assistance needed to continue for patient survival. Left ventricular MCE was performed, and the contrast filling defect in the anterior left ventricular wall, anterior interstitial wall and apex myocardium was found in segments 7, 8, 13, 14 and 15 (Section 17) (Figure 4).
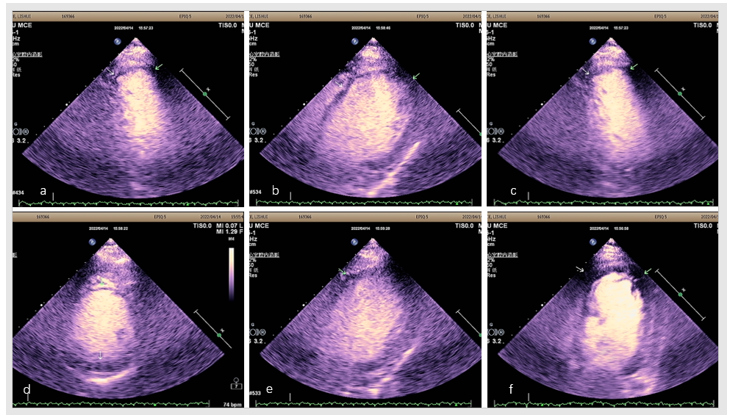
Figure 4: Left ventricular Myocardogram (Figure a. For apical view, contrast filling defect in segments 13 and 14 of the LV wall. graph b. Paraosternal four cavity, contrast filling defect in segment 17 of the LV wall. graph c. For apical view, contrast filling defect in segments 13 and 14 of the LV wall. graph d. Horizontal papillary muscle of the LV with contrast filling defect in segments 8 and 10 of the LV wall. graph e. Paraosternal four cavity, contrast filling defect in segment 8 of the LV wall. graph f. At the apex, contrast filling defects in segments 14, 15, and 17 of the LV wall.)
End-stage heart failure was diagnosed with indications for heart transplantation, and orthotopic allotransplantation was decided after multidisciplinary consultation in the whole hospital. On day 8 of admission, the patient underwent heart transplantation. The procedure was smooth, and the patient returned to the intensive care unit. ECMO, IABP auxiliary support, balaliximab anti-rejection, vancomycin and meropenem anti-infection procedures were continued. Erythrocyte infusion was performed to alleviate anaemia and improve coagulation function, haemostasis and sedation. Extensive myocardial ischemic necrosis and thrombosis were seen (see Figure 5).
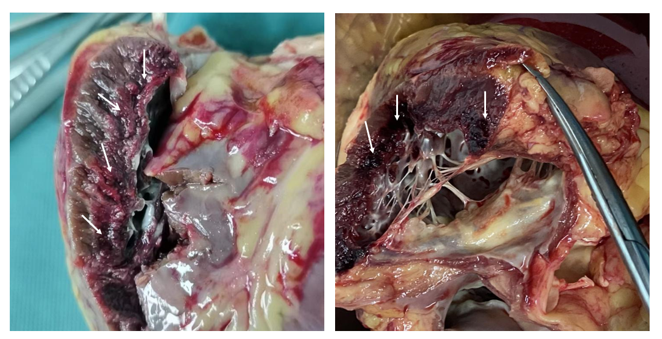
Figure 5 : Left ventricular myocardial specimen (arrow indicated: extensive myocardial ischemia and necrosis and thrombosis.)
Myocardial pathology was determined, and results showed the following: large coagulative necrosis in microscopic myocardial tissue; nuclear fragmentation and disappearance; red-dyed cytoplasm or irregular coarse granular appearance; formation of a contractile zone; interstitial oedema; scattered surrounding neutrophils infiltration; and congested bleeding zone in the infarct area. The left ventricle was predominant, and a small focal infarct area appeared in the right ventricle (see Figure 6).
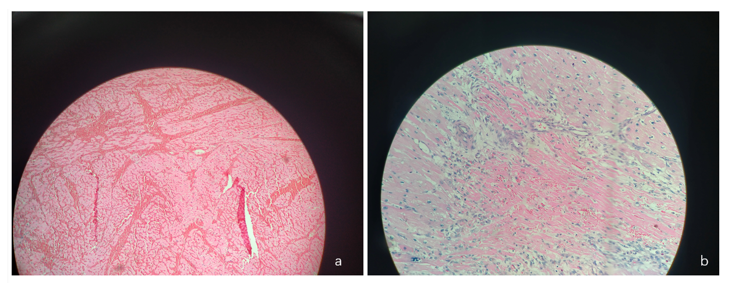
Figure 6: Cardiopathy pathology (Figure a: left ventricular myocardial pathology, Figure b: Right ventricular myocardial pathology. Under the microscope, the myocardial tissue shows large coagulative necrosis, nuclear fragmentation, disappearance and red-dyed cytoplasm or irregular coarse granular, formation of a contractile zone, interstitial oedema, scattered surrounding neutrophils and hyperhaemorrhagic zone in the infarct area. The left ventricle is predominant, and a small focal infarct area is present in the right ventricle.)
On the first postoperative day. The patient had stable respiratory and stable circulation, and the IABP assistance was removed. Review of cardiac colour ultrasound indicated the following: the left ventricular systolic function was normal; ejection fraction EF was 0.62; cardiac function was good; and stable hemodynamic status. ECMO assistance was removed, and the respiratory circulation was stable after withdrawal. On the eighth postoperative day, the patient’s respiratory function was normal. The oxygenation index was normal after shutdown. The tracheal tube was removed, and the breathing was smooth after extubation. On the eleventh day, the patient had stable vital signs and was transferred to the general ward. The patient was successfully discharged after 86 days of hospitalisation.
Discussion
ECMO is an effective auxiliary means for patients with cardiopulmonary failure. In patients with acute myocardial infarction and cardiogenic shock, ECMO support and rapid coronary recanalisation are important ways to rescue the surviving myocardium. The earlier the myocardial reperfusion is, the smaller the infarct area and the better the prognosis will be [4]. After this case experienced the secondary acute myocardial infarction, the cardiac function was seriously damaged. Such damage could lead to partial myocardial ischemia and necrosis after the first acute myocardial infarction. The infarction area could expand after the secondary myocardial infarction, which would ultimately affect the cardiac function. Some studies suggested that the recurrence rate of myocardial infarction, coronary heart disease events and mortality in males are higher than those in females [5]. The patient’s heart function was severely impaired. The patient required mechanical assistance, and heart transplantation was the treatment choice. The evaluation of myocardial survival is a critical step in determining whether a heart transplant needs to be performed. However, the recovery of myocardial function in AMI patients ultimately depends on the perfusion at the level of the myocardial microcirculation. At present, the commonly used detection methods for surviving myocardium are based on the characteristics of surviving cells, including myocardial metabolic imaging, myocardial perfusion imaging, ventricular wall motion observation (cardiac ultrasound, magnetic resonance), myocardial ultrasound angiography, body surface electrocardiogram and others. MCE by containing small bubbles with coronary angiography perfusion to the myocardial tissue, through the principle of the contrast backscattering signal stronger than myocardial perfusion range, is an important method for the clinical evaluation of interventional infarction-related artery myocardial fusion or no reflux. It is the evaluation method used for determining survival after myocardial infarction [3]. Tang et al. proved that when AMI patients have poor myocardial microcirculation perfusion after PCI, their left systolic function is weakened, and the left indoor diameter is enlarged. Early MCE detection helps evaluate long-term left ventricular systolic function changes and left ventricular remodelling [6].The present case had two acute myocardial infarction, with a TIMI flow grade of grade 0 in the anterior descending and spiral branches, as well as severe myocardial ischemia. Even in the patients with coronary recanalisation TIMI flow grade 3, myocardial no reflow phenomenon could occur [7]. Thus, there is a difference between the subepicardial coronary flow and the capillary level myocardial perfusion after PCI treatment. However, the recovery of myocardial function in AMI patients ultimately depends on the perfusion at the level of the myocardial microcirculation [8]. The MCE before transplantation in this case indicated that the patient’s left ventricular myocardial perfusion was severely impaired. A combination of the cardiac systolic function and hemodynamic conditions indicated that the patient had a low probability of cardiac recovery. The pathology of the postoperative myocardium has also demonstrated little cardiac surviving myocardium.
The long hospital stay in this case may be related to the patient's emergency heart transplant. Patients with ECMO assistance have many systemic pipelines and a high risk of infection, especially after experiencing cardiopulmonary bypass again during the process of heart transplantation. The inflammatory reaction caused by the cardiopulmonary bypass damages the body.
In conclusion, patients with secondary acute myocardial infarction are prone to severe heart failure. The myocardial angiography ultrasound imaging can evaluate myocardial perfusion and predict myocardial survival. It can serve as an important reference for emergency heart transplantation. But the existing MCE relies on the human visual assessment, a qualitative assessment is poorly reproducible, and the diagnosis procedure is highly dependent on the experience of the clinician.
List of abbreviations
MI : Myocardial infarction
MCE :Myocardial contrast echocardiography evaluation
TnT-HS Troponin T
CK: Creatine kinase
CK-MB : Creatine kinase isoenzyme:
ECMO : Extracorporeal membrane oxygenation
Veno-artery ECMO:VA ECMO.
Informed consent has been obtained from the patient and the hospital ethics Committee.
Not applicable.
Not applicable
The authors declare that they have no competing interests.
There was no funding for this study.
Xiaozu Liao ,Drafting article
Miaoyun Guo ,Data collection
ShI Zhong , Data collection
Junlin Wen ,Data analysis
Binfei Li ,Design
Informed consent was obtained from the patient in this case
Not applicable.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
