
Research Article | DOI: https://doi.org/10.31579/2637-8914/041
1 Research Scholar, Food Science and Nutrition Department, Banasthali Vidyapith, Rajasthan, India.
*Corresponding Author: Monika Seth, Research Scholar, Food Science and Nutrition Department, Banasthali Vidyapith, Rajasthan, India.
Citation: Monika Seth and Monika Jain (2021) Anthropometric Measurements and Health Status of Obese Omani Women: A Cross-Sectional Study (Age 30-49 Years). J. Nutrition and Food Processing, 4(1); DOI:10.31579/2637-8914/041
Copyright: © 2020 Monika Seth, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 February 2021 | Accepted: 22 February 2021 | Published: 01 March 2021
Keywords: BMI; Non communicable diseases; obese; WHR; women
Obesity has become a major health issue globally due to its increasing prevalence in certain parts of the world. In addition, because of its growing contribution to the burden of global morbidity, obesity has become one of the primary health concerns in many developed and developing countries. The WHO has warned of an escalating obesity epidemic that could put the population at risk of contracting non communicable diseases in many countries. Over the past 2 decades, Oman has been shown to bear a heavy burden of NCDs and numerous studies have documented the distribution of several risk factors coupled with lifestyle behaviors associated with many obesity related diseases giving rise to many more new health challenges in the nation. This article provides an overview of the anthropometric measurements and the health status of obese Omani women.
Objective: The main purpose of this research was to study the association between anthropometric measurements and the health status of the obese Omani women.
Method: The study was carried out during the period Sep 2019 to Jan 2020 and included a sample of total 398 obese Omani women aged 30-49 years from Muscat and Batina Governorates in Oman. Assessment of anthropometric measurements was done by calculating the BMI and WHR of the subjects and the health status was assessed by self-reporting of certain diseases using questionnaire cum interview method.
Result: The anthropometric assessments revealed that 47% were found to be grade I obese, 32% were grade II obese and 21% were morbidly obese with grade III obesity as per the BMI. On classifying the WHR it was found that 70% were in high category, 28% in moderate category and only 2% in low category. The health status of the subjects indicated that 81% of the subjects reported to have some obesity-related morbidity like hypertension, cholesterol, diabetes etc. or the other and only 19% of the subjects were free from any disease.
Conclusion: The obesity indicators i.e. BMI and WHR clearly showed a very high prevalence of obesity in the study sample. The anthropometric measurements are commonly associated with diseases like high cholesterol, hypertension and type 2 diabetes.
Obesity is a complex condition, one with serious social and psychological dimensions, that affects virtually all age and socio-economic groups and threatens to overwhelm both developed and developing countries [1]. Overweight and obesity contribute significantly to global deaths [2] and 2.8 million adults die each year as a result of being overweight or obese [3]. In addition, 44% of the diabetes burden, 23% of the ischemic heart disease burden and between 7 and 41% of certain cancer burdens are attributable to overweight and obesity [4]. Obesity was considered one of the biggest causes of morbidity and mortality both by deaths and life years adjusted for disability for the entire population (DALYs) [5]. The threats to the health of individuals and communities of this public health issue have also been illustrated in the new World Health Organization reports [6].
Most of the Gulf countries have experienced significant changes in their lifestyle habits, particularly dietary intake and over-indulgence in calorie dense, nutritionally deficient foods in recent decades [7]. Several studies have shown a high prevalence of diabetes, obesity and hypertension among Arab communities in the Middle East, including Omanis [8], which are further confirmed by another concerning study indicating a very high incidence i.e. 21% of metabolic syndrome in Omani population [9]. Alarmingly, in the GCC countries (Bahrain, Kuwait, Qatar, Oman, Saudi, UAE), with the highest rates of obesity, hypertension and diabetes in the world, the main cause of fatalities is heart disease and diabetes. In several studies, obesity has been linked very well with its associated conditions such as diabetes mellitus, hypertension, cardiovascular diseases, osteoarthritis and breathing disorders [10].Numerous reports have shown that the prevalence of both diabetes and high cholesterol is rising across the GCC and is a matter of serious concern [11]. For the last two decades, Oman has been identified to experience a tremendous brunt of non-communicable diseases and multiple studies have reported the dissemination of many contributing factors correlated with lifestyle behaviors connected to several diseases linked to obesity, resulting in many more new health challenges in the Sultanate [12, 13]. In Oman, women are at a greater risk of associated health concerns due to their low physical activity (PA) levels and high sedentary behavior (SB). A study of Omani college students showed that male students spent significantly more time exercising weekly( 6.84+_ 1.04 hours) than female students( 3.36+_ 0.70 hours) [14] . Data from the World Health Survey in Oman demonstrated that out of 5.006 new cases of type 2 diabetes, 51.5% were female [15].
As obesity has been recognized as a major risk factor for a variety of serious illnesses, it should be prevented. Since more than 38% of Oman’s female residents tip the obesity scales with mortality rates due to obesity related disease and cancer are high, with limited Studies on women’s health, this study was conducted to understand the association between anthropometric measurements and the health status of obese Omani women.
The recent cross-sectional research included obese women (aged 30-49 years) visiting AlRaffah Hospital and the subjects were registered between August and December 2019. After describing the purpose of the research and obtaining the informed consent form from each subject, the study was carried out. The research sample did not include pregnant women and those with any eating disorders. A total of 398 subjects having BMI more than 30 and aged 30-39 years were considered for the study. BMI (Body Mass Index) = Weight (kg) / height (m^2) was used as an indicator of obesity. The weight was measured using commercial scale “Seca, Germany” with an accuracy of ±100g. Standing height of the participant was measured using a standardized measuring scale. The participant was asked to stand on the horizontal platform without shoes, hold the arms loosely at the sides with the palms facing the thighs. The horizontal bar was lowered until it touched the crown of the participant’s head. The height was recorded to the nearest centimeters and if the reading fell between two values, the lower reading was always recorded. BMI was calculated and the cutoffs provided by the World Health Organization for defining obese (BMI above 30), obesity Grade 1 (30-34.99), obesity Grade II (35-39.99), obesity Grade III (more than 40) were adopted [9]. Waist and hip circumference was measured using a flexible and inelastic tape measure and noted in cm. This ratio is calculated by dividing the waist circumference (cm) by the hip circumference (cm). The WHR above 0.85 in women is considered to be obese and risk of diseases rises steeply when the WHR rises above 0.8. Self-reported questionnaire was administered where the subjects reported regarding their health status (i.e. diabetes, cholesterol, hypertension, osteoarthritis etc.).
Collected data were analyzed using IBM Statistics SPSS 25.0 (IBM Corp. Released 2017). For the descriptive purposes, continuous variables were presented with Mean, Median and Standard deviation. Categorical variables were presented with frequency and percentage. Chi square test was used for comparing the categorical variables. Probability value of < 0.05 was considered statistically significant.
Ethical Considerations: Approval was taken from the Ethical Review Board of Al Raffah hospital, Muscat prior to the start of interview and a brief orientation was given to each subject.
The anthropometric parameters were captured age wise as detailed below in Table 1.

When the subjects were asked about their opinion on their own weight, surprisingly, a majority i.e. 87% (n= 346) of the subjects considered their weight to be only slightly overweight, followed by 10 % (n= 40) who were aware that their weight was grossly excess while 3% (n= 11) also believed to have ideal body weight. Percentage of subjects were relatively higher in class III obese category (35%) who thought that their weight is grossly excess. Although, as revealed, not all the subjects considered themselves to be obese, yet a majority i.e. 57% (n= 225) of them said that they were conscious about their health and diet while 43% (n= 171) of the subjects admitted that they were not at all conscious about their health and diet. 54% (n= 213) of the subjects did nothing to maintain their health, 18 % (n= 73) depended upon exercise as a means to maintain their health, followed by 20% (n= 79) depended upon diet alone while 8% (n= 32) of the subjects followed both diet and exercise routine to maintain their health. Grade I obese subjects were found to take relatively more initiatives to maintain their health and exercise was their main method with 22% (n= 41) opting for it as compared to 14 % (n= 18) and 16 % (n=14) in class II and class III obese women respectively. Overall in class I obese 50% tried some approach to maintain their health while in class II and class III it was 43% and 44% respectively.
When the subjects were asked whether they got fatigued easily, a majority i.e. 77% (n= 308) of them reported to get tired easily and had diminished stamina while the remaining 23% (n= 90) answered in negative. In addition to this, fatigue seemed to have increased with increasing obesity and BMI. 86% (n= 73) of the grade III obese women agreed with this, and 82% (n= 103) grade II and 71% (n= 131) grade I obese subjects positively responded when asked whether they got fatigued easily.
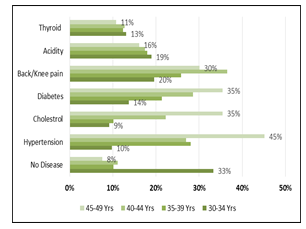
When the subjects were asked whether they were suffering from any of the diseases presently, it was found that only 19% (n= 74) of the participants indicated that they were not having any diseases and the rest 81% of the subjects self-reported to have some disease or the other. Hypertension was a common problem with the subjects i.e. 25% (n=99) of them suffered from it, followed by 23% (n= 91) with diabetes and 18% (n= 70) of them had high cholesterol. Other obesity related issues like back / knee pain were also common among the subjects (26%, n= 104) followed by 18% (n= 71) of them having gastric problems like acidity, heart burn etc. It was further observed that these health problems increased with age and younger generations had fewer health issues as compared to their older counterparts as shown in figure 1.
It was also noted that the comorbidities associated with obesity increased with increasing BMI as revealed in figure 2.

Class III obese subjects were found to suffer more from the obesity related diseases i.e. hypertension, high cholesterol, diabetes, arthritis, gastric problems and others as compared to the class I and II obese women.
Those subjects who answered in negative when asked about any diseases, 85% (n= 63) reported to have suffered from gestational diabetes when asked about having any past history of any major disease which highlights the correlation of obesity and diabetes.
The increasing burden of non-communicable diseases globally has become a rising public health concern. It was estimated by WHO in 2005 that 61 percent of the mortalities and 49% of the global disease burden could be attributable to NCDs and if the current trend continues, chronic diseases will account for 70% of deaths globally and 56% of the disease burden world wide by 2030 [16]. Overweight and obesity has always been registered among most of the populations in developing countries, including the Eastern Mediterranean region. The current study indicates increasing trends of obesity with age in Omani women which are consistent with the findings of several cross sectional surveys documenting a higher prevalence of obesity with increasing age. It was surprising to note that, most of the participants did not even consider themselves obese and reported that they were just little overweight, which was not a major concern for them at all. This misguided conviction, therefore, possibly kept them from taking action to reduce weight or maintain a healthy body. Cultural factors, practices and beliefs can play a significant role in the incidence of obesity in some Gulf countries; men influence Arabic women in determining the attitudes of women towards their own body size and shape in the incidence of obesity. A Qatar study found that 43% of Arab women claimed that men liked plump women [17] .Similar results have been documented in Morocco indicating a cultural preference for a flabby body [18] which was considered suitable and socially acceptable as reported by a majority of obese women. It is likely to serve as a defense mechanism for ignorant and unhealthy eating, thereby reducing their interest and motivation in losing weight [19]. This was very well demonstrated by most of the subjects when asked about the approach (i.e. Exercise, diet control etc.) they followed to promote good health and they stated that they did nothing specific for their health. Further, a majority of the subjects admitted that they had diminished stamina, suggesting a direct link between obesity and energy levels. Over the past couple of decades, Oman has been shown to face a substantial load of NCDs owing to a myriad of risk factors associated with lifestyle and eating habits [20, 21]. A high incidence of diabetes, hypertension and obesity in Arab women has been confirmed by numerous studies [22]. The International Diabetes Federation has reported high prevalence rates of over 20 percent for diabetes in most GCC countries and over 15 percent for prediabetes which are among the highest levels in the world [23].
The findings of the current study indicated that with the exception of just a handful, most of the participants suffered from one or more of the health conditions primarily associated with obesity, such as hypertension, hypercholesterolemia, diabetes, back and knee pain, heartburn, acidity etc. Hypertension has been regarded as one of the most prevalent health concerns globally and is positively associated with obesity; obesity being a significant risk factor for hypertension and other heart diseases [24]. Several researches performed in Tanzania exhibited that elevated BMI was associated with a 10% rise in the chances of hypertension 5, while a study in Nigeria showed an increase of 50%.[25]. A strong correlation between obesity and elevated triglycerides, lower HDL and higher total cholesterol levels at all ages, leading to metabolic syndrome has been highlighted in numerous studies [26]. Being overweight was the single most important factor in diabetes predisposition; risk further increases with increasing waist measurement thus making central obesity an independent risk factor diabetes development [27]. Obesity has been shown to be involved in the development or worsening of osteoarthritis in women and increasing the burden of low back and knee pain with obesity and increasing age. Obesity is also correlated with menstrual cycle disruptions and current estimates indicates that 30-47 % of overweight and obese women have been reported to suffer from these issues. The risk of developing gestational diabetes rises several fold with obesity and 50% of the women with GDM develop diabetes within 5-10 years after delivery as indicated by US studies [28]. According to the International Diabetes Federation, the prevalence of GDM was roughly 14 percent worldwide. Researches carried out to understand the connection between obesity and depression has provided contra suggestive results, with just a few showing an association [29]. More recently, reports from the Third National Health and Diet Analysis Survey showed some significant links between depression and women obesity but there is still not very strong correlation between obesity and mental health. Overweight, though, is a stigma and prejudice against obesity can contribute to many mental health issues, such as anxiety attacks, depression, eating disorders, low self-esteem etc. directly or indirectly impacting the quality of life [30].
Rising prevalence of obesity and the associated morbidities among Omani women can be attributed to an unhealthy lifestyle (i.e. nutrition deficit, high calorie diets and sedentary lifestyle) due to ignorance and unawareness about the benefits of a healthy and balanced diet. Our findings clearly indicate that Nutrition education programs focusing on women’s health and positively impacting their attitude towards healthy eating and exercise are urgently needed not only to fight this battle of bulge but also for the prevention of obesity related diseases i.e. diabetes, hypertension, hypercholesterolemia, osteoarthritis etc.
The authors declare that there are no conflicts of interest regarding the publication of this paper.
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
