
Case Report | DOI: https://doi.org/10.31579/2768-2757/132
General Surgeon, Department of Surgery, Medical Faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
*Corresponding Author: Ahmad Reza Shahraki., General Surgeon, Department of Surgery, Medical Faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
Citation: Ahmad R. Shahraki, (2024), 3 Years Chronic Simultaneous Separated Triple Large Bowel Volvulus in a Middle Age Female, Very Rare Patient: A Case Report, Journal of Clinical Surgery and Research. 5(5); DOI:10.31579/2768-2757/132
Copyright: © 2024, Ahmad Reza Shahraki. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 June 2024 | Accepted: 28 June 2024 | Published: 08 July 2024
Keywords: volvulus; ct –scan; case report; caecal volvulus; transverse colon volvulus; sigmoid colon volvulus
This case report has been reported in line with the SCARE 2020 criteria. Volvulus of transverse colon is rare when compared to cecal and sigmoid volvulus. Cases involving simultaneous volvulus of the transverse colon and another colonic segment are extremely rare. In adolescent’s sigmoid volvulus is rare and because of this diagnosis is usually missed or delayed. Volvulus is commonly defined as a twisted loop of the intestinal bowel and associated mesentery around a fixed point at its base. Surgery is the main course of treatment for Volvolus, ranging from simple detorsion to right colectomy. Sigmoid volvulus remains an uncommon cause of intestinal obstruction among the adolescent age group. A high index of suspicion is necessary to reach a diagnosis and manage accordingly. Delay in diagnosis can lead to complications such as necrosis and perforation of the twisted colon. Caecal volvulus is a rare cause of bowel obstruction, mainly caused by an exceedingly mobile caecum. Early diagnosis can be difficult due to its unspecific symptoms. Computed tomography plays a major role in a positive diagnosis. The main course of treatment is surgical, and modalities depend on various factors such as patient status and perioperative findings. Nowadays laparoscopic evolution continues to reduce postoperative morbidity. Transverse colon volvulus is an uncommon cause of intestinal obstruction. It is a surgical emergency that can lead to bowel infarction, peritonitis, and death.
Our case was a 52 female just with abdominal distention and we performed CT for her and we find Triple volvulus of large bowel that in history she has signs for 10 days in 3 years before. We operate him and Total colectomy was done and anastomosis of small bowel to rectum and discharge her healthy.
The surgical options in the management of acute large bowel obstruction, as a consequence of transverse colon volvulus, are one- or two-stage procedures. A one-stage procedure includes intraoperative colonic irrigation, resection of non-viable bowel, and primary anastomosis to avoid stoma creation. In a two-stage procedure, two options are available: (1) bowel is resected; the proximal end is brought out as terminal colostomy and distal end as a mucus fistula; 2–3 months’ post-surgery, end-to-end anastomosis is performed and (2) bowel is resected and end-to-end anastomosis is performed; a defunctioning colostomy or a loop ileostomy is fashioned to protect the anastomosis, which is closed 3–4 weeks later. Colonic volvulus usually occurs as a single event that can affect various parts of the colon. The usual sites affected being the sigmoid colon (75%) and the caecum (22%). The phenomenon of multiple sites simultaneously undergoing volvulus is an extremely rare occurrence. The dual location of strangulation makes this situation a major surgical emergency with a high risk of gangrene and septic shock. Colectomy with delayed anastomosis should be preferred in the treatment. Overall, metachronous colonic volvulus must be considered in the differential diagnosis of bowel obstruction, particularly in patients with significant risk factors. Early surgical intervention is essential for better outcome and avoiding complications. A metachronous transverse colonic volvulus is uncommon. Preoperative diagnosis is challenging as there are no defining radiographic features compared to the volvulus of the sigmoid colon with the classical omega sign. Most cases are diagnosed intra-operatively. Bowel resection and anastomosis in a single stage is a safe option. We report this case because in literature we did not find triple and chronic volvulus.
Volvulus is commonly defined as a twisted loop of the intestinal bowel and associated mesentery around a fixed point at its base. Caecal volvulus (CV) is a rare cause of intestinal obstruction, defined by an axial torsion of the caecum, ascending colon, and terminal ileum around the mesenteric vascular pedicles [1]. Preoperative diagnosis can be difficult due to its unspecific symptoms. As a result, CV is a surgical emergency and any delay in management can be associated with complications mainly bowel ischemia eventually leading to perforation and peritonitis [2]. CV is an infrequent cause of colon obstruction [3]. It is the second most frequent location of colonic volvulus and accounts for up to 60% of cases according to several studies [4]. To be diagnosed with CV, two conditions must be met: an abnormal mobile caecum associated with the lack of attachment of the mesenterium, caecum, or right colon to the posterior peritoneum [4, 5, 6] and a fixed point around which the caecum can twist [7].
Surgery is the main course of treatment for CV, ranging from simple detorsion to right colectomy [7]. If gangrene, necrosis, or perforation are identified, resection is mandatory, and the current method of choice is right colectomy with primary anastomosis or ileostomy depending on perioperative factors [8]. Three main procedures are described in the literature following caecum detorsion with no suspicion regarding its viability: isolated detorsion, caecopexy, and caecostomy [9]. Isolated detorsion without caecopexy or cecostomy is associated with a high risk of recurrence; therefore, it should not be used anymore [10]. Caecopexy is obtained by attaching the right colon to the parietal peritoneum with a recurrence rate of up to 40%. Cecostomy is associated with a higher risk of complications, including caecum gangrene, fistula, and leakage. In this case, our patient was young with signs of caecal pre perforation and not prepared for a right colectomy; as a result, we choose to perform a caecostomy. Compared to caecopexy, caecostomy has a higher rate of morbidity and mortality. As a result, caecopexy is recommended for patients with viable intestines not tolerating right colectomy and those
suffering from mobile caecum syndrome [11, 12]. Sigmoid volvulus is a rare cause of intestinal obstruction in children and adolescent population. It's considered a disease of the elderly with a widely varying incidence worldwide. It is more common in areas referred to as “volvulus belt” (Middle East, Africa, the Indian subcontinent, Turkey, and South America) [13]. Sigmoid volvulus is a rare cause of pediatric and adolescent bowel obstruction [14]. Acute sigmoid volvulus is an emergency abdominal condition common in adults but recent reports suggests children and adolescents are susceptible [15]. In adolescents sigmoid volvulus is rare and because of this diagnosis is usually missed or delayed [16]. This case report has been reported in line with the SCARE 2020 criteria [17]. Sigmoid volvulus is a rare cause of mechanical intestinal obstruction in adolescent although in adults it's more prevalent especially in “volvulus belt” where high fiber diet is the norm [18].
Volvulus of transverse colon is rare when compared to cecal and sigmoid volvulus. Cases involving simultaneous volvulus of the transverse colon and another colonic segment are extremely rare [22].
Our case was a 52 years old female with history of recurrent and transient abdomibal distention for 10 days in every months. She referred to Surgery parts and we start examinations and lab data’s. She has 6200/ml WBC, no fever, no nausea and no vomiting. She has good and healthy appearance and in abdominal examination she has distention synchronized in abdomen, no scar of surgery, no colorless and no tenderness. We perform a triple CT for her and we find 2 Simultaneous separated in cecal and transverse colon volvulus that in surgey we find them (figure1), with this information we programing a surgery for her. In Laparatomy we find transverse colon volvulus (figure 2) and we decide to do total colectomy (Figure 3). It shows she has 3 years Chronic Simultaneous separated triple large bowel volvulus (Figure3).

Figure1: cecal and transverse colon volvulus.
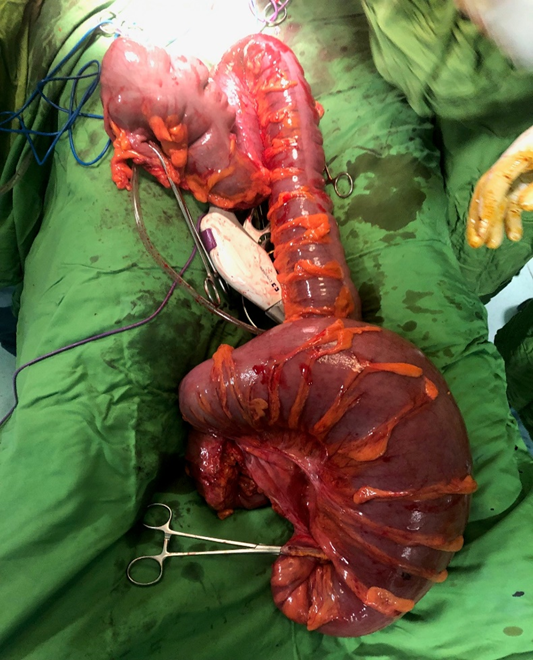
Figure2: Transverse colon volvulus.

Figure 3: Total colectomy.
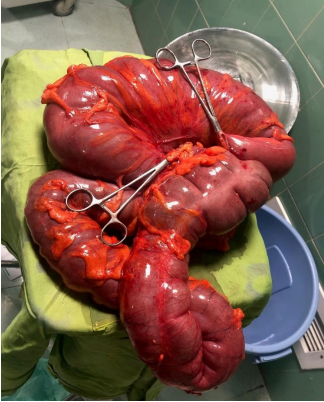
Figure4: Simultaneous separated triple large bowel volvulus.
After Total colectomy we anastomosis small bowel to rectum end to end. We send her to ICU and maintain therapy was done and after 4 days we start oral eating and we observed defication and lab datas. All of them was normal and we discharge her healthy after 6 days from admission.
Sigmoid volvulus remains an uncommon cause of intestinal obstruction among the adolescent age group. A high index of suspicion is necessary to reach a diagnosis and manage accordingly. Delay in diagnosis can lead to complications such as necrosis and perforation of the twisted colon [13]. Caecal volvulus is a rare cause of bowel obstruction, mainly caused by an exceedingly mobile caecum. Early diagnosis can be difficult due to its unspecific symptoms. Computed tomography plays a major role in a positive diagnosis. The main course of treatment is surgical, and modalities depend on various factors such as patient status and perioperative findings. Nowadays laparoscopic evolution continues to reduce postoperative morbidity [2]. In adolescent’s sigmoid volvulus is rare and because of this diagnosis is usually missed or delayed [16]. This case report has been reported in line with the SCARE 2020 criteria [17]. Among children males to female ratio is of 3.5:1 [18, 19]. Clinical presentation of mesenteric torsion is an intestinal obstruction, presenting with an acute abdomen and a major systemic inflammatory response which may compromise hemodynamic status [20]. Transverse colon volvulus is an uncommon cause of intestinal obstruction. It is a surgical emergency that can lead to bowel infarction, peritonitis, and death [21]. The surgical options in the management of acute large bowel obstruction, as a consequence of transverse colon volvulus, are one- or two-stage procedures. A one-stage procedure includes intraoperative colonic irrigation, resection of non-viable bowel, and primary anastomosis to avoid stoma creation.In a two-stage procedure, two options are available: [1] bowel is resected; the proximal end is brought out as terminal colostomy and distal end as a mucus fistula; 2–3 months’ post-surgery, end-to-end anastomosis is performed and [2] bowel is resected and end-to-end anastomosis is performed; a defunctioning colostomy or a loop ileostomy is fashioned to protect the anastomosis, which is closed 3–4 weeks later [21]. Colonic volvulus usually occurs as a single event that can affect various parts of the colon. The usual sites affected being the sigmoid colon (75%) and the caecum (22%). The phenomenon of multiple sites simultaneously undergoing volvulus is an extremely rare occurrence [22]. We report this case because in literature we did not find triple and chronic volvulus.
Caecal volvulus is a rare cause of bowel obstruction, mainly caused by an exceedingly mobile caecum. Early diagnosis can be difficult due to its unspecific symptoms. Computed tomography plays a major role in a positive diagnosis. The main course of treatment is surgical, and modalities depend on various factors such as patient status and perioperative findings. Nowadays laparoscopic evolution continues to reduce postoperative morbidity [2]. In adolescent’s sigmoid volvulus is rare and because of this diagnosis is usually missed or delayed [16]. This case report has been reported in line with the SCARE 2020 criteria [17]. Transverse colon volvulus is an uncommon cause of intestinal obstruction. It is a surgical emergency that can lead to bowel infarction, peritonitis, and death [21]. The surgical options in the management of acute large bowel obstruction, as a consequence of transverse colon volvulus, are one- or two-stage procedures. A one-stage procedure includes intraoperative colonic irrigation, resection of non-viable bowel, and primary anastomosis to avoid stoma creation.In a two-stage procedure, two options are available: [1] bowel is resected; the proximal end is brought out as terminal colostomy and distal end as a mucus fistula; 2–3 months’ post-surgery, end-to-end anastomosis is performed and [2] bowel is resected and end-to-end anastomosis is performed; a defunctioning colostomy or a loop ileostomy is fashioned to protect the anastomosis, which is closed 3–4 weeks later [21]. Colonic volvulus usually occurs as a single event that can affect various parts of the colon. The usual sites affected being the sigmoid colon (75%) and the caecum (22%). The phenomenon of multiple sites simultaneously undergoing volvulus is an extremely rare occurrence [22,23]. Although colonic volvulus is the third most common reason for bowel obstruction, the occurrence of simultaneous sigmoid and transverse colon volvulus is a rare condition that threatens patients’ lives. As there are no definite signs or symptoms or even clinical and imaging findings for simultaneous colonic volvulus, it is essential to consider this disease, do a careful physical examination, and pay attention to laboratory and imaging findings, especially in patients with abdominal pain or distention [24]. In spite of ascending and transverse colon volvulus rarity, we advised including these in the differential diagnosis of patients associated with large bowel obstruction [25]. The phenomenon of multiple sites simultaneously undergoing volvulus is an extremely rare occurrence [26]. The dual location of strangulation makes this situation a major surgical emergency with a high risk of gangrene and septic shock. Colectomy with delayed anastomosis should be preferred in the treatment [27]. Large-bowel obstruction caused by volvulus is potentially life threatening if not managed promptly [28]. Intraoperatively, we found a sigmoid volvulus and a concurrent transverse colon volvulus [29]. Overall, metachronous colonic volvulus must be considered in the differential diagnosis of bowel obstruction, particularly in patients with significant risk factors [30]. Early surgical intervention is essential for better outcome and avoiding complications [31]. A metachronous transverse colonic volvulus is uncommon. Preoperative diagnosis is challenging as there are no defining radiographic features compared to the volvulus of the sigmoid colon with the classical omega sign. Most cases are diagnosed intra-operatively. Bowel resection and anastomosis in a single stage is a safe option [32]. The diagnosis is likely to be made at laparotomy [33].
We report this case because in literature we did not find triple and chroninc volvulus.
Ethical Approval and Consent to participate:
The content of this manuscript is in accordance with the declaration of Helsinki for Ethics. No committee approval was required. Oral and written consent to participate was granted by her husband.
Consent for publication:
“Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.”
Availability of supporting data
It is available.
Competing interests:
The author declares that they have no competing financial interests and nothing to disclose.
Funding: There is no funding.
Authors' contributions:
Ahmad Reza Shahraki is the surgeon of patient and writes this paper.
The author declares that they have no competing financial interests and nothing to disclose.
Acknowledgements
This case is so rare in novel and database that we search and report it. This case report has been reported in line with the SCARE 2020 criteria.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
