
Case Report | DOI: https://doi.org/10.31579/2693-4787 /015
1 Medical Oncology Department, Faculty of Medicine of Tunis, Salah Azaiez Institute, El Manar University, Tunis, Tunisia.
2 Pathology Department, Faculty of Medicine of Tunis, Salah Azaiez Institute, El Manar University, Tunis, Tunisia.
*Corresponding Author: Yahyaoui Yosra, Medical Oncology Department, Faculty of Medicine of Tunis, Salah Azaiez Institute, El Manar University, Tunis, Tunisia.
Citation: Yahyaoui Yosra, Ghorbel Achref, Charfi Lamia, Gamoudi Ahmed, Gabsi Azza and Mezlini Amel. Low Grade Abdominal Leiomyosarcoma with Liver Metastasis: A Second Cancer Twenty Years after Treatment for Nasopharyngeal Cancer, J. Clinical Oncology Research and Reports. 1(2). Doi: 10.31579/2693-4787 /015
Copyright: © 2020 Yahyaoui Yosra, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 October 2020 | Accepted: 10 November 2020 | Published: 26 November 2020
Keywords: leiomyosarcoma; soft tissue sarcoma; anthracyclines; case report
Background: leiomyosarcoma is one of the most frequent soft tissues and abdominal-pelvic sarcomas however intra-abdominal leiomyosarcoma with liver metastasis remain a very rare disease.
Case presentation: A 61 year-old man presented in February 2019 a recent history of abdominal pain and weight loss. Imagery showed a 5 cm abdominal mass with multiples liver lesions. Biopsy of the liver lesions concluded to a metastases of a low grade leiomyosarcoma. Surgical resection was deemed not possible due to anatomical restrictions and the patient received 6 cycles of systemic mono-chemotherapy with epirubicin. A CT scan performed after the chemotherapy showed a stable disease using RECIST criteria.
Conclusions: In case of an unresectable liver metastasis palliative chemotherapy can be offered although it is widely recognized that leiomyosarcoma show moderate sensitivity to chemotherapy.
Leiomyosarcoma (LMS) is a type of malignant soft tissue sarcoma of smooth muscle that may occur anywhere in the body. Abdominal LMS is highly aggressive with an overall 5 year survival rate ranging between 20 and 30 % [1].
Wide resection is the standard treatment for LMS. Hepatic metastases from soft tissue sarcomas are rare and the treatment has not been standardized. Anthracycline monotherapy and combination chemotherapy containing doxorubicin are options for treating metastatic soft tissue sarcoma [2]. Here we report a case of a metastatic LMS that developed in a 61-year-old man 20 years after he was treated for a nasopharyngeal carcinoma
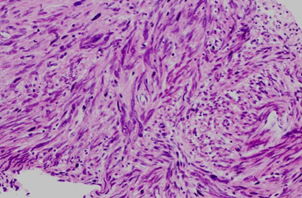
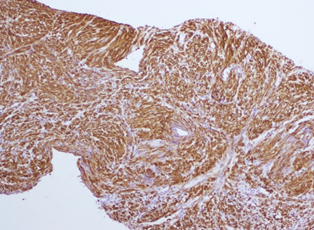
A 61 year-old man, non-smoker, treated in 1999 with chemotherapy and radiotherapy for an undifferentiated nasopharyngeal cancer classified at the time T3N3M0 presented in February 2019 a recent history of abdominal pain and weight loss. He underwent a full body scan that showed a 5 cm abdominal mass located in front of the vascular axis of the left iliac region with multiple liver metastases. Biopsy of the left iliac mass concluded to smooth muscle tumor without clear sign of malignancy as some moderate cytonuclear atypia was seen without necrosis or mitosis (Figure1). Immunohistochemistry was positive for desmine and caldesmone but negative for CD34 and PS100. A fine needle biopsy of a hepatic lesion showed a hepatic parenchyma widely invaded by a mesenchymal proliferation of variable density depending on the territory. The proliferation was made of fusiform cells with an oval nucleus of slightly unequal size with finely granular chromatin, those cells were arranged in crisscrossed beams. Mitosis were rare (1 mitosis/ 10 high power fields (HPF) and no necrosis was seen. Tumor cells stained positive in Immunohistochemistry for caldesmone (Figure2) and negative for CD34, Ckit, Dog1, HMB45 and CK.
The diagnosis of liver metastasis of a low grade abdominal leiomyosarcoma was made. After multidisciplinary assessment, surgical resection was not deemed possible due to anatomical restrictions and the patient received a systemic mono-chemotherapy with epirubicin (75mg/m2). The CT scan performed after six cycles of chemotherapy showed a stable disease using RECIST criteria. At the time of finalization of this report, and 8 months post-treatment, the patient was still alive.
Leiomyosarcoma is one of the most frequent soft tissues and abdominal-pelvic sarcomas [3], however intra-abdominal LMS with liver metastasis remain a very rare disease . Surgical resection should be offered for all patient as long term survival can be achieved after an R0 resection [4].
In case of an unresectable liver metastasis palliative chemotherapy can be offered although it is widely recognized that LMS show moderate sensitivity to chemotherapy [5].
Single-agent anthracyclines and specially doxorubicin is a standard systemic treatment of soft tissue sarcomas, and subsequently for LMS although it showed a lower response rate compared with other sarcoma types [6]. Epirubicin can also be used as it is less cardiotoxic and provides outcomes that are comparable with doxorubicin [3].
Causes and predisposing factors of LMS remains unclear although Epstein-Barr virus (EBV) infection has been associated with LMS in the setting of severe immunosuppression such as the association of EBV with LMS in young people with AIDS shown by McClain et al [7]. Immunodeficient individuals are also prone to develop Epstein-Barr Virus–Associated Smooth Muscle Tumor (EBV-SMT) which represent a heterogeneous group of disorders with a broad pathological spectrum ranging from leiomyoma-like to leiomyosarcoma-like tumors [8] . In such cases, the detection of EBV in the tumor cells remains the mainstay for distinguishing them from conventional leiomyosarcoma [9] .
In our case, although the biopsy of the left iliac mass concluded to smooth muscle tumor without clear sign of malignancy we still think that this mass is probably the primary site of the LMS as it is possible that the small fragment that was taken out may not be relevant to all the tumor.
Our patient had a history of an undifferentiated nasopharyngeal cancer which is also EBV related , however we were not able to do the detection of EBV in tumor cells in order exclude an EBV-SMT , although the fusiform cells proliferation remains in favor of conventional LMS . This medical history underlines the importance of this case as it is interesting by the rarity of a second cancer after treatment for nasopharyngeal cancer in a Tunisian patient (Tunisia being an area of intermediate incidence), outside the field of radiotherapy, usual area of second malignancies. Also the non-response to chemotherapy and the unusual clinical presentation made us question the initial diagnosis of abdominal sarcoma and to discuss a gastrointestinal stromal tumor (GIST). A paper published in 2019 by Guohua Yu et al showed that GIST outside the gastrointestinal tract or with CD117-negative expression may be misdiagnosed as smooth muscle tumor because of the positive expression of H-caldesmon. In this paper H-caldesmon was positive in five cases outside the gastrointestinal tract and in two other cases that were CD117 negative, and all of those cases were diagnosed as GIST and confirmed by genetic sequencing.[10]
Surgical resection remains the first-line treatment of metastatic low grade abdominal LMS. However, anthracycline chemotherapy may be indicated in patients whose abdominal LMS is unresectable. Due to the disease's poor prognosis, ongoing evaluation of current therapy and development of new treatment strategies are required.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
