
Case Report | DOI: https://doi.org/10.31579/2693-4787/014
1 Medical oncology department, Salah Azaiez Institute, Tunis, Tunisia.
2 Pathology department, Salah Azaiez Institute, Tunis, Tunisia.
*Corresponding Author: Yahyaoui Yosra, Medical oncology department, Salah Azaiez Institute,Tunis ,Tunisia
Citation: Y Yosra, Z Yosr, B Ilhem and M Amel. (2020). Primary Primitive Neuroectodermal Tumor of the Parotid: An Unsuspected Diagnosis. Clinical Oncology Research and Reports. 1(2); Doi: 10.31579/2693-4787/014
Copyright: © 2020 Yahyaoui Yosra, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium,provided the original author and source are credited.
Received: 29 September 2020 | Accepted: 12 October 2020 | Published: 19 October 2020
Keywords: primitive neuroectodermal tumor; parotid; surgery; chemotherapy; radiation therapy
Primitive neuroectodermal tumors (PNETs) are extremely rare tumors. These neoplasms can occur at sites outside of the central nervous system. The head and neck location is unsual. We report a case with primitive neuroectodermal tumor (PNET) of the parotid. We analyze through this observation the clinical, histological and therapeutic characteristics of this entity.
Primitive neuroectodermal tumors (PNETs) are malignant tumors of the central nervous system. These malignancies are usually found in children and young adults. The diagnosis of PNETs is based on light microscopy following identification of a small round cell tumor and on the immunohistochemical staining results. They can occur at sites outside of the central nervous system usually within bone, pelvis, the chest wall and rarely in the head and neck [1]. We present here an extremely rare case of PNET of the parotid gland.
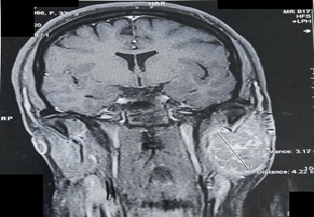
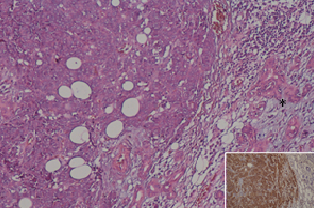
A-33-year-old woman presented with a recurrent rapidly growing mass in the left parotid of 12 months duration associated with facial asymmetry. She had an excision of this mass in another institution since 6 months. The initial histological examination showed a benign mixed tumor of the salivary glands. On physical examination, she had a facial paresis. A left submandibular mass was noted. The tumor size was 6 cm. Upon clinical examination, a painless, non swelling and fixed mass (4x4cm) was found on the left parotid. There was no nodal involvement. Magnetic resonance imaging (MRI) of head-neck showed a soft‑tissue mass of heterogenous density in the left side of the parotid gland (Figure 1). The size of the tumor was measured 31*35*42mm. The lesion appeared heterogeneous hypointense on T1 weighted images and hyperintense on T2 weighted images. The tumor had irregular contours with invasion of pterygoid and masseter muscles. She underwent surgical excision with total parotidectomy, including facial nerve sacrifice. Histological examination showed a polylobulated tumor with peripheral hemorrhagic reshuffle. Tumor cell proliferation infiltrating parotid gland parenchyma with nodular or diffuse architecture was observed. Solid sheets of small- to medium-sized cells with round to oval nuclei, basophilic cytoplasm and mitotic figures were revealed (Figure 2). There were no lymph node metastases.
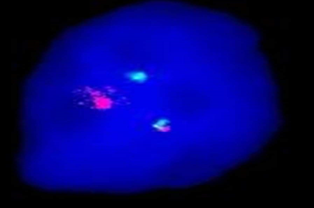
The immunohistochemistry showed positivity for cytokeratin, CD99 and negativity for S-100 protein, CD45, synaptophysin, chromogranin, CD56, vimentin, epithelial membrane antigen(EMA) and CD34. On the basis of these findings, the lesion was confirmed to be a pPNET of the parotid gland. Cytogenetic analysis showed the specific translocation involving the EWSR1 gene on chromosome 22q12. This specific genetic abnormality was demonstrated by FISH (Figure 3). At the time of this writing, our patient is alive. She started start adjuvant radiation therapy and chemotherapy (VDC/IE regimen).She received 9 courses of chemotherapy. She finished the treatment one month ago. The patient has been under close observation since the treatment and there have been no signs of recurrence.
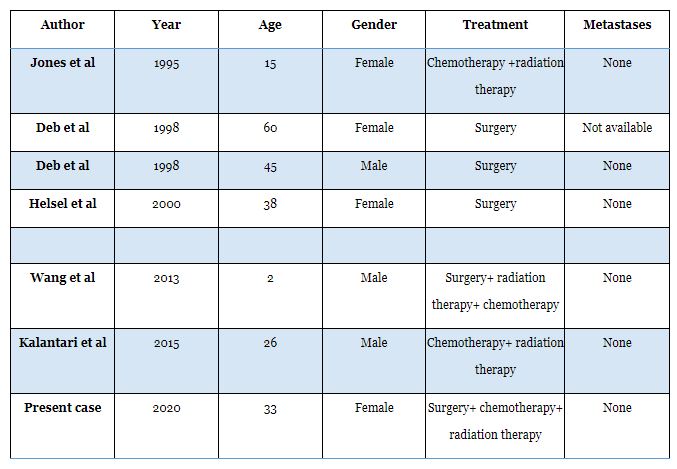
We describe a case of localized primary primitive neuroectodermal tumor (PNET) of the parotid in a 33 year –old man. PNET are rare tumors that belong to the Ewing’s sarcoma family. They represent 1% of all sarcomas [2]. Commonly, PNET is seen in children and young adults. It has a slight predilection for males and occurs in bone and within soft tissues [3]. PNETs are rarely noted in the head and neck region. They can be found anywhere within the body, particularly in the trunk and extremities. Cases of PNET occurring in the genital tract, chest wall and retroperitoneal cavity have been reported [4]. In the head and neck region, PNET is usually found in the jaw, mandible and maxilla [5] . The clinical presentation is often associated with pain, swelling and cranial nerve deficits [6]. The patient in the current case presented with rapidly growing mass in the left parotid associated with facial asymmetry. PNET of the parotid is extremely rare. Only 6 cases have been reported in the literature (table 1). The imaging features of pPNETs are non-specific but are essential for diagnosis and surgical planning. On MRI, the tumor appears isodense or slightly hypodense on CT scan. Cystic or necrotic area with non-calcified masses are usually observed. On MRI, [7]. Histologicallay, the most helpful diagnostic feature is the presence of rosettes, usually of Homer-Wright type[6]. However, it is usually difficult to differenciate PNETs from other small roud-cells cancers. Immunohistochemically is useful for the differential diagnosis. In fact, PNETs consistently stain immunohistochemically for vimentin and CD99. Tumor cells are negative for desmin and cytokeratin. Molecular and cytogenetic studies are essential to confirm the diagnosis. A chromosomal translocation t (11;22)(q24;q12) is found in about 90% of PNETs [6].
The cornerstone of multidisciplinary treatment is surgery followed by radiotherapy with doses
ranging from 45 to 60 Gy and chemotherapy. Our patient had surgery followed by chemotherapy(VDC/IE regimen) and radiation therapy. Surgical excision with negative margins is paramount for local control. But, this surgery can be difficult in the head and neck region in cases of involvement of vital structures. Radiation therapy and chemotherapy can be considered in these cases [8]. The most effective chemotherapeutic regimen for PNETs are Vincristine, Cyclophosphamide, Doxorubicin ,Iphosphamide and Etoposide. Despite the various treatments available, the prognosis of PNETs remains poor.
Close cooperation among surgeons, radiation and medical oncologists is needed for the management of PNET of the head and neck.
Funding: None
Conflict of interests: None
Authors contributions:
Yosra Yahyaoui: Guarantor, Concepts, design, literature search, manuscript preparation
Yosr Zenzri : Concepts, design, literature search, manuscript preparation, statistical analysis
Bettaieb Ilhem : definition of intellectual content, Design
Amel Mezlini: Concepts, Definition of intellectual content
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
