
Review | DOI: https://doi.org/10.31579/cic-2021/003
*Corresponding Author: Ranjit Kumar Sharma, Department of Cardiology, Nepal Mediciti Hospital, Lalitpur, Nepal.
Citation: Ranjit K Sharma, Anish Hirachan, Milan Gautam and Prabesh Neupane (2021). Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): What does an interventionist need to know? Clinical and Interventional Cardiology. 1(1); DOI: 10.31579/cic-2021/003
Copyright: © 2021 Ranjit K Sharma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 July 2021 | Accepted: 23 July 2021 | Published: 04 August 2021
Keywords: CAD; high-sensitivity cardiac troponin assays; MINOCA; ST-segment elevation; acute coronary syndrome ; INOCA; AMI; obstructive coronary disease; hypertension; diabetes mellitus
In the 1980s, De Wood et al. reported that approximately 10% of patients with MI were found to have non-obstructive CAD. Currently, the prevalence may be even higher in the era of high-sensitivity cardiac troponin assays; because of the lower specificity to diagnose acute MI. MINOCA occurs in 5–15% of patients presenting with acute ST-segment elevation MI (STEMI) or non-ST segment elevation MI (NSTEMI). Many terms have been coined to describe patients with AMI or acute coronary syndrome (ACS) with normal or near-normal coronary arteries, such as MINOCA, MINCA (MI with normal coronary arteries) and INOCA (ischaemia and no obstructive coronary artery disease).
In the 1980s, De Wood et al. reported that approximately 10% of patients with MI were found to have non-obstructive CAD [1]. Currently, the prevalence may be even higher in the era of high-sensitivity cardiac troponin assays; because of the lower specificity to diagnose acute MI [2]. MINOCA occurs in 5–15% of patients presenting with acute ST-segment elevation MI (STEMI) or non-ST segment elevation MI (NSTEMI) [3]. Many terms have been coined to describe patients with AMI or acute coronary syndrome (ACS) with normal or near-normal coronary arteries, such as MINOCA, MINCA (MI with normal coronary arteries) and INOCA (ischaemia and no obstructive coronary artery disease) [4,5]. The term MINOCA is incorporated into the recently published Fourth Universal Definition of AMI [6]. Compared with obstructive coronary artery disease, factors associated with MINOCA include the female sex, younger age (<55 p=0.68>
A 38-year-old man was referred to emergency department for ongoing chest pain. He had sudden onset of central, crushing chest pain for 7 hours, with severity increasing in the last 2 hours and the symptoms were associated with sweating. The patient had a known case of hypertension and was on medication for the last 2 years. The patient was also a pre-diabetic. His mother had hypertension and diabetes mellitus. There is no history of hypertension, diabetes mellitus or cardiovascular disease in his siblings.
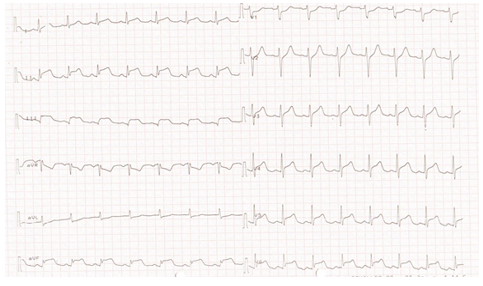
General Examination: O2 saturation-95%, Pulse-110 bpm, Bp-110/90mmHg.Systemic Examination: no abnormality detected. Investigation: CBC, RFT, BSR, and Electrolytes were with in normal limits. ECG: ST elevation in infero-lateral leads. Cardiac Biomarkers: CPK-MB-82u/l and Trop 11.6u/l. Echo screening: hypokinetic inferior LV wall.
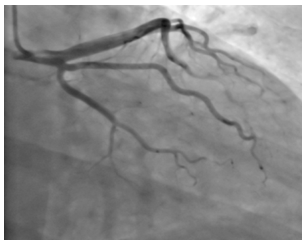
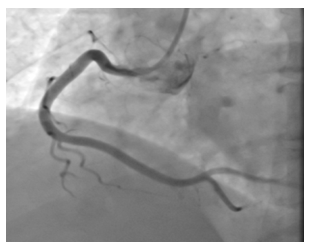
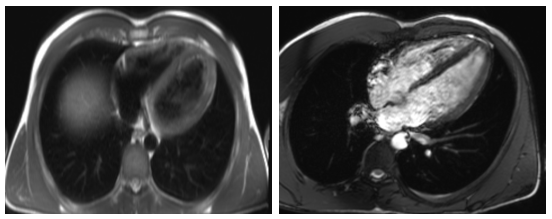
He was diagnosed as acute infero-lateral wall MI and was taken to the cath lab. His coronary angiography studies revealed normal coronary arteries. He was admitted in the CCU and was treated with Aspirin, Clopidogrel, LMWH, Atorvastatin, Beta-Blocker, Anxiolytics, PPI and Stool softener. On the following day, cardiac MRI was performed, which revealed curvilinear, confluent and patchy subendocardial enhancement noted in infero-posterior wall of the left ventricle. Features are compatible with myocardial infraction. He was conservatively managed and was discharged on 5th post MI day.
Definition and Pathophysiology of MINOCA
The diagnosis MINOCA requires (1) the presence of an AMI (according to the Fourth Universal Definition of AMI), (2) non-obstructive coronary arteries on invasive coronary angiography, defined as no coronary stenosis≥50% in any potential infarct-related artery, and (3) no clinically overt specific cause for the acute presentation [6]. In a patient presenting with symptoms of ischaemia, cardiac enzyme elevation and echocardiographic or electrocardiographic features suggestive of acute MI, a working diagnosis is made during angiography in the absence of culprit obstructive coronary artery disease (epicardial coronary artery stenosis ≥50%) or an apparent systemic cause for the presentation [13,14]. Approximately one-third of patients have been reported to present with suspected STEMI within an emergency setting and the remaining majority as NSTEMI patients undergoing subsequent angiography [3]. MINOCA disorders can be classified within the fourth universal definition of MI [6]. They may meet criteria for type 1 MI, where epicardial coronary artery disorders are diagnosed, or type 2 MI due to endothelial dysfunction or oxygen supply and demand mismatch, or myocardial injury [6]. (Figure. 2)
Cardiac causes of MINOCA include:
1. Plaque disruption and plaque erosion
2. Spontaneous coronary artery dissection
3. Coronary artery spasm
4. Coronary micro vascular dysfunction
5, Coronary thrombus or embolism
Non-cardiac causes of MINOCA can result in myocardial injury include (PE), (end-stage) renal failure, sepsis; stroke and other forms of type 2 MI such as anemia and hyperthyroidism. They can also be associated with chest pain, elevated cardiac enzymes and ECG changes. (Figure. 3)
Diagnosis and Evaluation of Patients with MINOCA
When a patient meets the criteria for a working diagnosis of MINOCA (universal acute MI criteria, infarct-related epicardial stenosis ≤50%, absence of overt alternative systemic cause) during angiography, then further invasive and adjunctive investigations should be considered at this point such as Coronary intravascular ultrasound (IVUS) or optical coherence tomography (OCT) [15,16,17]. Left ventriculography may also be of value in the assessment of other causes, such as takotsubo syndrome, and is routinely performed in many percutaneous coronary intervention (PCI) centers [18]. In addition to measurement of left ventricular end-diastolic pressure (LVEDP), ventriculography may also indicate an epicardial territorial distribution of impaired kinesis implicating a single epicardial artery, compared with a microvascular pattern involving an extended territory of one or more arteries. The upper limit of normal for LVEDP is 10 mmHg and LVEDP >18 mmHg is associated with an adverse post-MI prognosis [19]. Following invasive angiography, transthoracic echocardiography should be performed specifically assessing for the presence of regional wall motion abnormalities, embolic sources, pericardial effusion and typical features of takotsubo syndrome [20]. CMR can identify inflammation, oedema and scar and can assess myocardial function by T1 - and T2 -weighted imaging [21]. CMR is an important diagnostic tool and is guideline recommended in all patients with MINOCA [22]. If present on CMR, late gadolinium enhancement localizes the site of myocardial damage, and the pattern of distribution suggests the diagnosis [23]. Subendocardial or transmural enhancement is typically of ischaemic etiology. Subepicardial enhancement may be observed in myocarditis, cardiac sarcoid or cardiomyopathy associated with Duchenne muscular dystrophy. Mid-wall enhancement is associated with dilated cardiomyopathy, hypertrophic cardiomyopathy, Duchenne muscular dystrophy, Becker’s muscular dystrophy, Anderson–Fabry disease, sarcoidosis or myocarditis. Finally, global endocardial enhancement is associated with amyloidosis, systemic sclerosis, hypereosinophilic syndrome or Churg–Strauss syndrome, whereas the absence of late gadolinium enhancement may be in keeping with microvascular dysfunction or a non-cardiac cause of the presentation [24]. CMR should be performed as soon as feasible after identification of MINOCA (within 4 weeks after hospital admission). However, in 8–67% of patients no abnormalities could be found, which leads to a therapeutic dilemma for clinicians [25]. (figure.4)
Therapeutic Strategies for Patients with MINOCA
MINOCA secondary to plaque disruption or with evidence of ischaemic damage on CMR receive dual antiplatelet therapy (12 months followed by lifelong single agent), high-dose statin (including in patients with minimal plaque burden), β-blocker and ACEi or ARB [26, 27]. Mineralocorticoid receptor antagonists (MRA) may have a theoretical role in improving outcomes of MINOCA patients because aldosterone levels immediately after acute MI are associated with all-cause mortality. Aldosterone mediates the downstream effects of RAAS activation, including endothelial dysfunction, inflammation and fibrosis, but, at present, there are no trial data of MRA therapy in MINOCA patients [28].
Outcomes of Patients with MINOCA
With outcomes similar to those of patients with acute MI and obstructive coronary disease up to 1 year (12-month mortality 0.6% versus 2.3%, respectively; p=0.68), MINOCA is not benign [11]. Mortality and the incidence of major adverse cardiac events (MACE) for MINOCA patients are reported as comparable with those of patients with obstructive coronary artery disease, as and significantly worse than for the general population [29]. Within the SWEDEHEART registry, approximately one in four patients experience a MACE within 4 years, including death, recurrent MI, hospitalization with heart failure or ischemic stroke [30]. There are no studies focused on the effects of MINOCA on quality of life, including persistent ischaemic symptoms and psychosocial parameters. MINOCA-BAT will include a sub-study assessing the prevalence of angina pectoris in addition to health-related quality of life, anxiety, depression and psychiatric comorbidities [27].
MI with non-obstructive coronary arteries (MINOCA) is a heterogeneous working diagnosis requiring further investigation during and after invasive angiography. Clinicians should consider the use of intracoronary imaging and coronary physiology testing during angiography to assess for plaque disruption and vasospasticity. Cardiac MRI with gadolinium contrast is recommended in all MINOCA patients. MINOCA is not benign and has comparable outcomes with acute MI due to obstructive coronary artery disease. Treatment of the underlying cause is paramount although, at present, often empirical. There is an unmet clinical need for stratified therapy for patients with MINOCA.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
