
Review | DOI: https://doi.org/10.31579/cic-2021/001
*Corresponding Author: Debabrata Dash, Department of Cardiology, Aster Hospital, A1 Mankhool, Dubai, UAE.
Citation: Debabrata Dash, Naveed Ahmed, Rohit Mody, Jayachandran Thejus and Sreenivas Reddy (2021). Drug-coated balloon in percutaneous interventions: A relevant tool or an unwarranted hype? Clinical and Interventional Cardiology. 1(1); DOI: 10.31579/cic-2021/001
Copyright: © 2021 Debabrata Dash. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 June 2021 | Accepted: 17 July 2021 | Published: 28 July 2021
Keywords: drug-coated balloon; percutaneous coronary intervention; in-stent restenosis; congenital heart; neuro-interventional pathologies; POBA; coronary revasculatization; DES
Representing an enhancement of the therapeutic repertoire for the interventional cardiologist, the drug-coated balloon (DCB) delivers antiproliferative drugs to local arterial tissue and prevents restenosis, leaving no implant behind. This innovative strategy attenuates the risk of delayed inflammatory response to device component without preventing positive remodeling. Using an appropriate technique, DCBs may play a role in coronary in-stent restenosis, de novo small vessel or bifurcation lesions where the deployment of drug-eluting stent is either not desirable or technically challenging. With extensive research, the device is being constantly refined and its numerous potential applications studied. Not only this device fulfills the specific needs in the coronary vasculature, but also there is great potential for its use in other non-coronary vascular territories and structures including the management of valvular, congenital heart and neuro-interventional pathologies. This review enlightens the rationale for DCB use, its effectiveness in different clinical and lesion setting and the future perspective.
Percutaneous plain old balloon angioplasty (POBA) revolutionized coronary revasculatization [1]. POBA, however, was associated with abrupt closure and restenosis caused by elastic recoil, neointimal hyperplasia and late remodeling. The application of drug-eluting stents (DES) reduced in-stent restenosis (ISR), not only by preventing recoil of the vessel wall and late negative remodeling, but also by significantly inhibiting neointimal hyperplasia formation. However, concerns of stent thrombosis, dependency on prolonged dual antiplatelet therapy (DAPT), and continued restenosis led to a quest for new treatment modalities that would address restenosis rates without DES related drawbacks [2-5]. In recent years, a new technology, the drug-coated balloon (DCB) represents an enhancement of the therapeutic repertoire for the interventional cardiologist. The DCB is designed to have the same antirestenotic effects as a DES with the advantage of additional flexibility and no implant remaining in the vessel. Despite many publications, current knowledge on this device is limited to few well-formed trials and several confounding studies. This review will shed light on the rational, technical aspects, current indications and future perspectives of DCB.
Rationale
A great deal of research has been undertaken to help understand the underlying biological mechanisms of ISR, which has been the most important measure of clinical success since the introduction of stents [6]. ISR is the result of the interaction of a variety of biological processes beginning immediately after stent deployment and is characterized by an excessive neointimal hyperplasia [7]. DESs have been developed to overcome this concern [8]. Despite significant reduction in restenosis, DES restenosis persists in subsets of patients particularly diabetic patients and those with complex lesions. Moreover, efficacy of DES has been challenged by the rare and unpredictable risk of annoying late stent thrombosis [9, 10]. Another pitfall of this device is non-uniform delivery of drug on the arterial wall with highest concentration at the stent struts and the lowest between the struts and the margins. Other limitations include small vessel disease (SVD) treatment because of stent thickness, stent layers left in the artery with arterial vasomotricity abnormalities after multiple layers, and issues pertaining to the duration of DAPT.
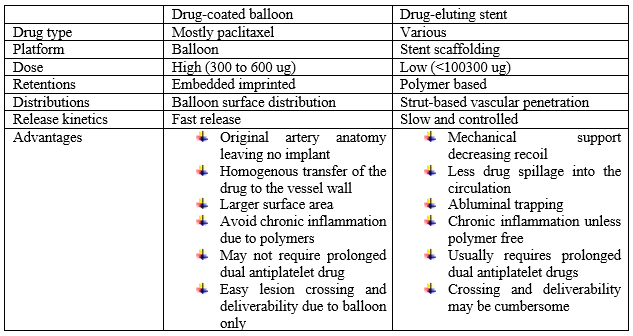
These concerns prompted the quest for improved solutions, such as the local delivery of drugs via nonstent-based platforms, including DCB. The potential advantages of DCB include (a) homogenous drug transfer to the vessel wall enhancing the efficacy of the drug to the artery; (b) rapid release of high concentrations of the drug sustained in the vessel wall no longer than a week with little impact on long-term healing; (c) absence of inflammatory polymer decreasing the trigger for late thrombosis; (d) absence of a stent that would maintain original geometry of arteries, notably in cases of bifurcation or small vessels, thereby decreasing abnormal flow patterns; and (e) limited dependency on DAPT (Table 1) [11].
Nevertheless, use of DCB is without few drawbacks. It has the mechanical limitation of acute recoil seen post POBA. Furthermore, it is not clear whether DCB can evict the late negative remodeling seen with noncoated balloons. The efficacy and safety parameters when using DCB as adjunct therapy to bare metal stents (BMS) or DES must also be determined in case of acute closure caused by occlusive dissection. Other potential disadvantage could be variability of pharmacokinetics and control of dosing [11].
Technical aspects and available devices
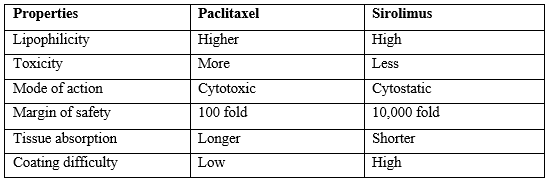
Initially the extensive research was performed to develop local delivery of drugs into the vessel wall, but clinical results are unsatisfying because of absorption variability and quick washout of drugs being studied. The interest in non-stent based local drug delivery system was reignited with the emergence of sirolimus and paclitaxel, both liphophilic drugs absorbed rapidly by the arterial tissue. There are four key elements in DCB: balloon platform; drug; excipient and balloon coating process. Upon inflation, acute drug transfer occurs almost immediately to deliver the drug from the balloon’s surface to the arterial wall, mostly binding to hydrophobic binding sites on the latter, with lesser amount being transported by diffusion and convection [12-15]. Factors influencing transfer efficiency include the inherent physicochemical properties of the drug, manufacturing and coating process, and the presence of excipients. Several properties of the balloon coating may be crucial for effective drug delivery to the target site, including (1) its form on the balloon surface; (2) the homogeneity of distribution along balloon surface; (3) stability during production, handling, and storage; (4) the degree of premature loss while during transition to the target vessel segment; (5) the ability to release during balloon expansion; (6) the transfer efficiency to the vessel wall; and (7) the amount of particulate material released to the distal circulation [15]. The release kinetics of the drug to the vessel wall is critical to the efficacy and safety of the procedure.11Paclitaxel binds to B- tubuline microtubule subunit and exerts locally very potent, dose -dependent inhibitory effects on human arterial smooth muscle cell proliferation, thereby tackling neointimal hyperplasia [16]. The optimal concentration of paclitaxel has been studied in animal models with doses ranging from 1-9 ug/mm2, with an optimal efficacy at 3 ug/mm2 dose, without any further benefit at higher dose [17]. Although most DCBs for human use release paclitaxel, recent DCB development incorporates limus instead due to cytotoxicity of paclitaxel (Table 2) [18].
The methods to load the drug to the balloon include dipping, spraying, nanoparticles, and imprinting the drug on the rough surface of the balloon. With of different excipient and coating, the pharmacological properties of resulting DCBs can be quite different (Table 3).
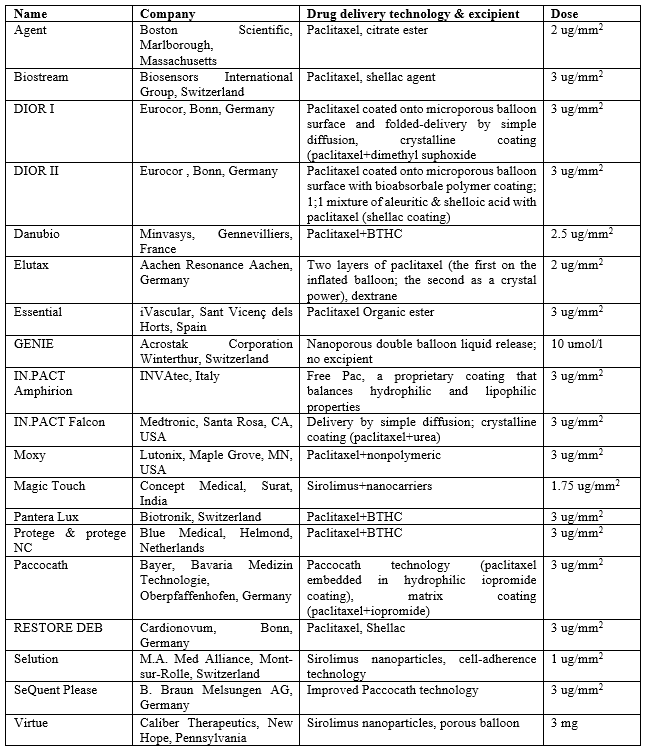
Limus-based drugs are cytostatic, with a higher safety margin than paclitaxel. A meta-analysis done by Dangas et al [19]. Reports lower mortality and superior clinical outcomes with everolimus DES compared with Taxus DES. However, the drawback of using sirolimus in DCB is that the lower lipophilic property of the drug makes tissue absorption and elution more difficult. Newer-generation DCBs have adopted different delivery technologies to address this problem. The Magictouch (Concept Medicals, Surat, India) sirolimus-coated balloon catheter incorporates the Nanolute technology (Concept Medicals), which is a nano-carrier-based drug-delivery technology in which nano-sized encapsulated particles carry the drug. The Selution sirolimus DCB (MedAlliance, Sankt Gallen, Switzerland) incorporates microspheres made from a biodegradable polymer intermixed with sirolimus, which ensures a controlled, sustained release with maintenance of the therapeutic effect in tissue over long periods of time. The Selution DCB also has a unique cell-adherent technology, which protects microreservoirs during balloon insertion, lesion crossing, and expansion. The Virtue sirolimus DCB (Caliber Therapeutics, New Hope, Pennsylvania) has incorporated a microporous angioplasty system with numerous 4-mm laser-drilled pores that delivers sirolimus nanoparticles and allows enhanced tissue penetration with controlled and sustained drug delivery. These DCBs have shown promising result with lower MACE and TLR rates in registry studies [20-22].
Tips and tricks for DCB use
An adequate lesion preparation is critical to successful use of DCB. The general rule of predilatation is to use a conventional or semi‑compliant balloon with a balloon/artery ( B/A) ratio 0.8–1.0 under a moderate pressure between 8 and 14 atm to prevent dissection (Figure 1). Non-compliant high pressure balloons, cutting or scoring balloons, rotational atherectomy and intravascular lithotripsy may be used in case of fibrocalcific lesions. Fractional flow reserve, optical coherence tomography or intravascular ultrasound may be performed in cases of doubtful results. The diameter of the DCB should match with the diameter of the target blood vessel and the reference ratio of B/A is between 0.8 and 1.0 [23-25]. Every attempt should be made to prevent drug loss. Manipulation of balloon must be avoided during flushing and preparation of the catheter. Attention should be paid while crossing the Y-connector, navigating through the guide catheter and proximal part of the artery up to the lesion. The balloon should be brought as rapidly as possible to the target and inflated gently to avoid drug loss in blood stream. Recommended dilatation against the arterial wall lasts for 30–60s. The balloon should be expanded under the nominal pressure of 7-8 atm to reduce the risk of dissection. As residual stenosis caused by elastic recoil often recurs, a stent-like result should not be expected. Residual stenosis <30>

B/A: balloon/artery; CB: cutting balloon; DCB: drug-coated balloon; DES: drug-eluting stent; FFR: fractional flow reserve; HCCL: heavy calcific coronary lesion; IVUS: intravascular ultrasound; ISR: In-stent restenosis; IVI: Intravascular lithotripsy; NC: noncompliant; OCT: optical coherence tomography; RA: Rotational atherectomy; SB: scoring balloon; IVL: intravascular lithotripsy, SC: semicomlaint
Potential Clinical Indications
This segment sheds light on the clinical data of DCB treatment in Coronary Artery Disease (CAD), peripheral artery disease (PAD) and other potential applications.
1. Coronary artery disease
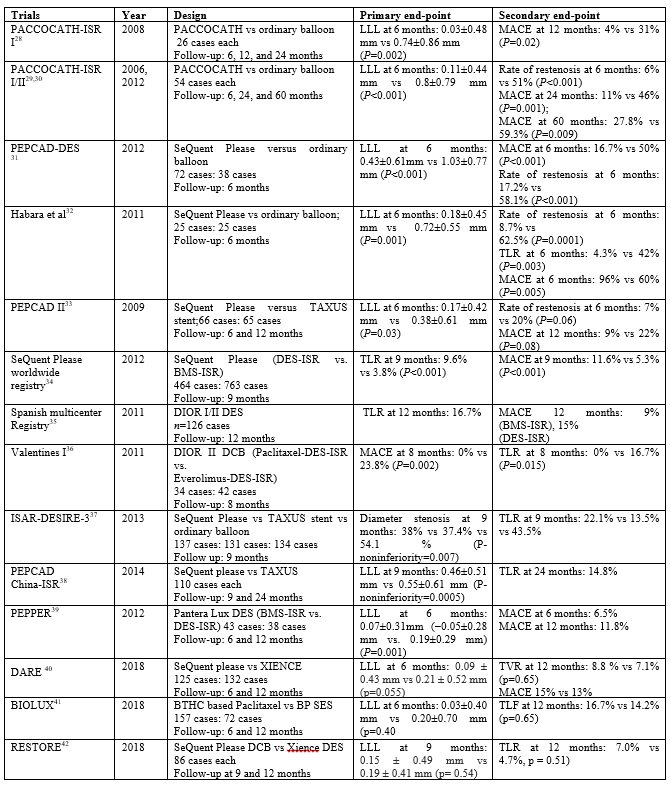
Since PACCOCATH ISR (Paclitaxel-coated balloon catheter for In-Stent Restenosis) was initiated in December 2003, [28] several clinical trials have consistently shown the efficacy and safety of the DCB in treatment of ISR (Table 4), SVD and bifurcation lesions.
1.1 ISR
ISR is the preferred application of DCB. Studies have demonstrated better efficacy and safety of DCB in treatment of ISR when compared with POBA and DES [28-45]. Results of the 2‑year follow‑up of PACCOCATH ISR have demonstrated the safety of the DCB in treatment of coronary ISR and the reduction in the rate of repeated revascularization [29]. Three randomized clinical trials have compared DCBs to DESs in BMS restenosis lesions (PEPCAD II ISR, [33] RIBS V, [46] and Pleva et al [47]), and another three trials have compared DCBs to repeat DES in DES restenosis (RIBS IV, [48] ISAR-DESIRE 3, [37] and PEPCAD China ISR [38]). In the randomized trials comparing DCBs to DES in BMS restenosis, PEPCAD II ISR has shown equivalent outcomes at 1 and 3 years, and the another published trial by Pleva et al has demonstrated lower late lumen loss (LLL) and equivalent clinical outcomes as compared to an everolimus-eluting stent (EES). Only the RIBS V trial has demonstrated better outcomes with a DES. Of the three randomized trials comparing DCBs to DESs in DES restenosis, ISAR-DESIRE 3 has demonstrated that the DCB is as effective as DES in treatment of ISR and has a better safety profile, and PEPCAD China ISR study has shown superior clinical outcomes with DCBs at 2 years. Although RIBS IV has shown better outcomes with repeat DES at one year, it is better to wait for long term safety and efficacy information before considering multiple layers of DESs. The meta-analysis by Siontis et al,[49] reviewed all treatment strategies for coronary ISR lesions and concluded that “two strategies should be considered for treatment of any type of coronary ISR: PCI with EES because of the best angiographic and clinical outcomes, and DCB because of its ability to provide favorable results without adding a new stent layer. The meta-analysis by Elgendy et al, [50] reported that DCB use was associated with lower in-segment minimum lumen diameter and higher in-segment diameter stenosis but lower LLL at a mean follow-up of 8.2 months when compared with DES use. Moreover, a higher rate of TLR was reported with DCB use at a mean follow-up of 27 months. Rates of a variety of other clinical outcomes, including target vessel revascularization (TVR), myocardial infarction (MI), stent thrombosis, all-cause mortality, and major adverse cardiac events (MACE), did not differ between groups. Another meta-analysis reported that repeat stenting with DES was moderately more effective than DCB in ISR reducing the need for TLR at 3 years. The incidence of a composite of all-cause death, MI, or target lesion thrombosis was similar between groups. The rates of individual endpoints, including all-cause mortality did not vary significantly between different groups [51].
Based on the results of aforementioned studies, the European Society of Cardiology/European Association for Cardio‑Thoracic Surgery (ESC/EACTS) Guidelines on myocardial revascularization recommends the DCB for treatment of ISR with an I A level of evidence [52].
1.2 De novo Coronary Lesions
Clinical studies using DCB in de novo CAD have reported mixed results, with a major benefit in SVD. All these studies adopted two main approaches. In combination strategy, DCB angioplasty was performed initially, and then a BMS or DES was deployed, while in the “leave nothing behind strategy,” DCB angioplasty was performed, and a stent was implanted only as a bailout strategy for the suboptimal result after the DCB. A combination of DCB and DES was advocated in patients at high risk for restenosis, such as those with diabetes, but clinical data are limited for this group [53].
1.2.1 Small vessel disease
Small vessel disease (SVD) is likely to have higher rates of restenosis irrespective of the type of intervention. DCB is superior in this subgroup as there is no further reduction of lumen by metallic struts and the drug’s sustained ability to reduce neointimal hyperplasia [57]. BASKET-SMALL [58] is the largest study to date on SVD which compared SeQuent Please DCB (Braun Melsungen AG, Berlin, Germany) with everolimus or Taxus DES (Boston Scientific, Marlborough, Massachusetts). This study concluded that at DCB was noninferior to DES 12 month follow-up (MACE 8% vs. 9%). RESTORE SVD [59] compared the Restore DCB (Cardionovum, Bonn, Germany) with zotarolimus DES and demonstrated that DCB was noninferior to new-generation DES for the primary endpoint for percentage stenosis (11% vs. 7.5%, p value for noninferiority <0 xss=removed xss=removed>
1.2.2 Bifurcation lesions
Treatment for bifurcation lesions pose a great challenge despite continuous improvement in PCI techniques and technologies. Two stent technique is a complex procedure and associated with a higher risk for ISR and thrombosis and may require prolonged DAPT. Despite the lack of data, the use of DCB in the bifurcation lesions in addition to standard provisional stenting could be an innovative and useful strategy when side branch (SB) stenting is not needed, due to lack of additional procedural risk compared to standard treatment and because of the possible positive prognostic implications, especially by reducing the risk of progression of the disease within the SB. The DEBIUT trial examined the outcome of using DCB in the SB and main branch (MB) with BMS/DES in the MB. The use of DCB revealed no angiographic and clinical superiority over BMS, with DES-only strategy achieving the best angiographic results [61]. The BABILON trial concluded with the same results whereby the DCB and BMS approach led to higher rates of TLR and MACE compared to the DES-only group [62]. The results of the PEPCAD V study [63] have demonstrated the feasibility of DCB in treatment of bifurcations lesions, while the PEPCAD‑BIF study [64] has proven the superiority of DCB compared to ordinary balloon. The DEBSIDE trial analysed the role of DCB in the SB after placement of a DES in the MB, demonstrated a very low risk of complications and of TLR at 6 months, with a good angiographic outcome [65]. Similar results were obtained in the SARPEDON study which assessed the efficacy of DCB at the SB ostium after DES implantation in the MB, with good angiographic outcome and low rate of restenosis, although a high rate of MACE (19% at 1 year) [66]. The author suggests that DCB could be an option for the treatment of the SB in provisional stenting technique. Further randomized controlled studies are warranted to decide whether DCB could improve the overall treatment outcome of bifurcation lesions.
1.2.3 Large vessel disease
DCB-only strategy is found to be safe and effective in the treatment of de novo lesions in large (3.0-mm) coronary arteries as well with low risk rates of clinical events and acute vessel closure, which may be due to the lack of foreign material and its inherent thrombogenicity [67,68]. However, further randomized controlled trials (RCTs) comparing DCB with latest generation DES in this scenario is warranted.
1.2.4 Acute coronary syndrome
Although DES in ST elevation myocardial infarction (STEMI) reduces restenosis, it has a risk of uncovered stent struts, and late malapposition, which carries the risk of stent thrombosis. Primary PCI with DCB may represent a valuable alternative strategy by which the purpose of truly leaving nothing behind can be accomplished without compromising results. It provides a homogeneous distribution of the drug and a subsequent reduction in endothelial inflammation while maintaining the integrity of coronary vasomotor response and vessel geometry with proven positive remodeling. Primary PCI with DCB incorporating the Pantera Lux balloon (Biotronik AG, Buelach, Switzerland) was compared with sirolimus or everolimus DES in the REVELATION trial [69]. The DCB showed no significant difference in LLL (0.05 ± 0.13 mm vs. 0.00 ±0.05 mm, p = 0.51) and clinical outcomes (MACE 3% vs. 2%, p = 1.00) at 9-month follow-up. Gobic et al, 70 also showed similar results in STEMI patients at 6-month follow-up in another study. Based on REVELATION trial, the author hypothesizes that DCB PCI may have a place in STEMI, where the lesions are generally short and less calcified and the patients typically younger; a group for whom avoiding DES may be an excellent idea. The DCB-only strategy is noninferior to stent treatment in non–STEMI as well [71].
1.2.5 Diffuse coronary lesion
The hybrid approach of combining DCB with DES has been evaluated in de novo long diffuse coronary artery disease. This approach employs a DES implantation in the proximal lesion, and PCB with DCB in the distal lesion. This overall reduction in stent length might be beneficial for lowering restenosis rates. However, it is important to note that these devices are not intended to treat the same diseased vessel segment. Of note, in this hybrid approach for diffuse disease, the sequential lesions should be treated separately without an overlap between the treated segments because of a higher risk of restenosis. This approach has acceptable, with comparable MACE and TLR rates in the treatment of diffuse coronary artery disease [72].
2. Peripheral artery disease
FP territory is accountable for most of the lifestyle-limiting claudication present in clinical practice. It is the most relevant vascular territory with the greatest demonstrated need for reduced restenosis rates. Not only these vessels are subjected to external compression, but also to interplay of complex forces during hip and knee flexion, including bending, torsion, and axial elongation/shortening. Percutaneous transluminal angioplasty (PTA) has proved to be inferior to stent implantation for moderate length lesions (≤13 cm), [73] but 1-year patency rates even with stents was still only 63%. DES is not found to be effective in reducing restenosis in the FP territory because of the tendency for stents to fracture leading to restenosis, [74] the rigid stent interacting with a vessel constantly in motion, and the lack of the correct “formula” of drug dose and duration when accounting for intimal hyperplasia in this unique vessel. Therefore, DCB technology holds the promise to improved outcomes without a permanent implant.
The THUNDER trial [75] randomized a total of 154 patients with stenosis or occlusion of the superficial femoral or popliteal arteries to an uncoated balloon (control group), a Paccocath balloon (approximately 3 μg/mm2 of paclitaxel), or an uncoated balloon and paclitaxel dissolved in the contrast medium (eg, Ultravist, Bayer Radiology & Interventional; 17.1 mg paclitaxel in 100 mL). At 6-month follow-up, treatment of patients with Paccocath balloons was found to be associated with significant reductions LLL (primary endpoint) compared to patients of the control group or patients treated with paclitaxel dissolved in the contrast medium remained significantly lower in the Paccocath group compared with both other groups registered a lower rate of TLR at 6, 12, and 24 months. 5-years follow-up data revealed sustained long-term efficacy of DCB over PTA, with significantly lower binary restenosis and TLR rates [76]. The Femoral Paclitaxel trial randomized 87 patients to control balloon angioplasty and iopromide-paclitaxel-coated balloon angioplasty in relatively short (≤6 cm) lesions in the FP arteries. The coated balloon exhibited significantly less LLL (primary end point) at 6 months than the control balloon and significantly lower rate of TLR. This difference in TLR was sustained beyond 18 months [77]. The ILLUMENATE studies showed the safety and efficacy of the Stellarex DCB compared to uncoated PTA [78]. DCB is highly recommended in TASC IIA and B de novo and restenotic FP lesions as per an international positioning document [79]. Although meta-analyses have confirmed the superior performance of DCB versus PTA for de novo FP lesions, [80] the long-term durability as well as the efficacy of DCB therapy in patients with ISR of arteries requires further investigation. There is a need of more clear information regarding a relationship between DCB and mortality although all available data except the Katsanos meta-analysis have been supportive of the safety of paclitaxel-coated devices [81].
The performance of DCB for below-the-knee (BTK) disease has been found useful terms of binary restenosis, target vessel occlusion and TLR.
3 Future potential applications
3.1 Valvular heart disease
Degenerative aortic stenosis (AS) is the most frequent manifestation of valvular heart disease in the elderly and it is the foremost indication for surgical aortic valve replacement (SAVR). The recommendation for SAVR is however impacted by the presence of multiple comorbidities, e.g., advanced age, neurological dysfunction, left ventricular dysfunction and, therefore, higher surgical risks [82]. Owing to these reasons, up to one-third of such patients are not referred for this life-saving and symptom-improving SAVR. In recent years, transcatheter aortic valve interventions (TAVI) has been developing into an effective and reproducible therapy for patients who do not have a reasonable surgical option [83]. However, it is apparent that many of these patients will not be candidates for TAVI due to technical and logistics requirements. Balloon aortic valvuloplasty (BAV) is a less invasive percutaneous option for nonsurgical candidates with symptomatic AS that results in temporary symptomatic relief. BAV results in higher rate of early restenosis and dismal long-term survival. Today it is reserved for the stabilisation of haemodynamically unstable patients, particularly as a bridge towards surgical valve replacement or TAVI. BAV is not a lost-cause and remains an attractive option to explore, when TAVI program cannot be embarked on [84]. Restenosis following BAV has been attributed to elastic recoil and scarring reaction with refusion of split commissures, cellular proliferation with formation of granulation tissue, and heterotopic ossification. Therefore, this later dynamic component of the restenosis process may be a target for drug inhibition. One simple approach to deliver drugs inhibiting this dynamic healing process would be to use drug-coated valvuloplasty balloons. Utilizing paclitaxel-eluting balloons in animal pre-clinical studies, Spargias et al were able to demonstrate significant delivery of this drug to the aortic root, aortic valve leaflets, as well as the left ventricular outflow tract after 2-4 inflations [85]. Dr. Spargias performed the first-in-man aortic valvuloplasty with a paclitaxel-eluting balloon on September 26th in Athens, Greece, during the Athens Interventional Cardiovascular Therapeutics (AICT) 2008 [86]. The procedure was performed on compassionate grounds in a patient with severe symptomatic AS who was a poor candidate for SAVR or TAVI (Table 5).

A press release from the company developing this balloon reported a reduction of the transaortic pressure gradient from 56 to 32 mmHg after two inflations of a 20×40 mm balloon. Another study reported that use of a paclitaxel-eluting valvuloplasty balloon in an animal model of AS resulted in attenuated restenosis, secondary to decrease in valve proliferation and calcification [87].
Although the incidence of rheumatic mitral stenosis has declined significantly in developed countries, it is still quite prevalent in many of the developing nations. Percutaneous balloon mitral valvuloplasty (BMV) has been the mainstay of treatment for this condition. Mitral restenosis is mainly due to commissural re-fusion and the progression of subvalvular thickening and/or degeneration. Turgeman et al, [88] reported that patients with mitral restenosis caused by symmetrical commissural re-fusion often responded well to repeat balloon commissurotomy procedures as compared to patients in whom restenosis is mainly subvalvular and the commissures are not bilaterally fused but rather unilaterally or bilaterally split. The author feels that similar to BAV with DCB, it is logical to combine the Inoue balloon, which splits the commissure, with an anti-proliferative drug coating, for enhancing the long-term success of BMV.
3.2 Paediatric intervention
Balloon dilatation has been performed since many years for congenital aortic and pulmonary
shunts and other extra-cardiac conduits). In some cases, stent implants are necessary. Conduit stenoses tend to restenose easily after POBA. Stent implantation offers better durability. The stent-vessel size mismatch continues to remain an issue in a growing child. ISR, stent fracture, limitation in future surgical conduit replacement, significant regurgitation in a valved conduit and coronary artery compression are other potential stent-related problems [89].
DCBs seem to be attractive for these indications. They may offer durable benefits compared to POBA alone and avoid stent related problems. This potential has not escaped the attention of paediatric cardiologists and paclitaxel-eluting balloon treatment of congenital pulmonary vein restenosis [90] and pulmonary artery ISR [91] has been reported (Table 5).
3.3 Neuro intervention
The optimal treatment for patients with symptomatic severe intracranial atherosclerotic disease is not well established. PTA and stenting have been attempted, with controversial results, mainly attributed to perioperative complications and a high incidence of restenosis or in-stent restenosis. One retrospective study suggests that DCB dilatation may be a safe and effective alternative for intracranial de novo atherosclerotic disease [92]. Grubber et al, [93] in a pilot study included ten patients (all men, median age 73 years) where median pre-treatment stenosis grade was 78% with four internal carotid artery, two mid-basilar artery, and four vertebral artery lesions. Median post-treatment stenosis grade was 50%. DCB achieved successful PTA in all cases without technical failure. There were no cases of peri-procedural reocclusion and no deaths at median follow-up of 3 months. Wang et al, [94] reported a case of successful DCB angioplasty in symptomatic vertebral artery stenosis (Table 5) where the patency was maintained at 6 months. Although PTA with a regular balloon is the most reported treatment for carotid ISR, re-ISR seems to limit the durability, leading to recurrent interventions and cost implications. Techniques using DCBs are on the rise and may become the treatment option of first choice, but long term follow-up is needed to evaluate their superior efficacy.
3.4 Other vascular intervention
The ability to perform therapeutic dilatation followed by local spray of a drug to prevent restenosis has generated keen interest in applying the DCB to other parts of the vasculature.
3.4.1 Central vein stenosis
One of the potential applications of DCB is in central vein stenosis angioplasty. Previous experiences with POBA or stent implant showed poor primary patency rates (less than 30%) at one year. Repeat angioplasties provided reasonable assisted primary patency rates and is the norm regardless of whether there was a stent implanted [95]. Chong TT et al, in a retrospective cohort study of all hemodialysis patients who underwent central vein angioplasty, demonstrated a similar target lesion primary patency (TLPP) for DCB and POBA with a trend toward a longer re-intervention-free period for DCB [96].
3.4.2 Stenosis of arteriovenous fistula and grafts
Paclitaxel-coated DCB have potential roles in treating stenoses of hemodialysis access, such as arteriovenous fistula and grafts (AVF/AVG) [Table 5]. Few clinical results using DCB in AVF/AVG venous stenosis and/or restenosis have demonstrated superior primary outcomes with higher Circuit Patency (CP) and TLPP with 100% anatomical success [97,98]. Another study demonstrated that use of a DCB in patent, dysfunctional arm of AVFs resulted in an improved patency trend over control at 9 months and not at other time points over the 2-year study, as well as significantly reduced interventions to maintain TLP and a significant prolongation of time to next intervention at the target lesion [99]. The one-year IN.PACT AV trial results, first presented at LINC 2020 (28–31 January, Leipzig, Germany), [100] reveal that the TLP in the patient group treated with the IN.PACT drug-coated balloon (DCB; Medtronic) was 63.8% compared to 43.6% in the group treated with plain balloon angioplasty (p<0>).
3.4.3 Pudendal artery stenosis
Male sexual function has always been a topic of intense interest for many. It is clear that erectile dysfunction is a close correlate of CAD, sharing many of the same risk factors and has common co-existence. Out of the many etiologies, 80 % of cases are because of vasculogenic origin. Venous leak and arterial Inflow problems (usually pudendal artery stenosis) are the most common etiologies. Many therapeutic options are available for erectile dysfunction (ED) today and the introduction of phoshodiesterase-5(PDE-5) inhibitors have revolutionized its management. However, there remain a significant number of patients who do not respond favourably to these modern treatments. This may be due to the unaddressed problem of vascular insufficiency. In ED patients with concomitant leg and hip claudication, stenosis of the common or internal iliac arteries may be the responsible which may be addressed easily via PTA with good durable results. In other patients, the culprit lesions may be stenoses in the more distal pudendal arteries and its branches.86 Khanna et al, suggests that angioplasty of focal stenosis of internal pudendal artery by DCB or DES appears to be a very promising therapy for male erectile dysfunction (Table 5). It is safe, feasible and leads to sustained improvement of male erectile dysfunction in about 75 % of carefully selected cases. However still many cases are ineligible for this procedure. Larger studies are warranted to be able to accept it as a standard therapy to treat ED. The author believes that DCB application for ED should be seriously explored ahead of stent implantation to avoid the risk of stent crush, thrombosis, penile ischaemia, gangrene and even amputation [101].
The development of DCB is an important milestone in the field of cardiovascular interventions, particularly when a non-stent approach is mandated. There is an ample clinical evidence to demonstrate its safety and efficacy of in the treatment of ISR. Meanwhile, additional evidence supports that DCB is indicated in treatment of SVD and some de novo coronary and peripheral arterial lesions. This technology may be quite promising in targeting neuro, valvular and paediatric interventions and AV fistula treatment. However, larger RCTs, adequately powered with clinical end points, are warranted to further elucidate the role of DCB in these conditions. Although, there is great excitement on its potential applications in various coronary, cardiac and extra-cardiac interventions, DCB is still an evolving technology that is undergoing refinement. This novel technology is here to stay and take an important position in the interventional field to complement the various percutaneous intervention strategies available in the current century.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
