
Research | DOI: https://doi.org/10.31579/CIC-2021/004
*Corresponding Author: SenDasgupta Chaitali, Professor, Departments Cardiac Anaesthesia, Institute of Post Graduate Medical Education and Research, Kolkata.
Citation: Chaudhuri S, SenDasgupta C, Goswami A, Sinha S (2021). Comparison of Effects of Prophylactic Amiodarone versus Lignocaine and Magnesium Sulphate versus Placebo in Prevention of Arrhythmias in Patients Undergoing Valve Replacement Surgery. Clinical and Interventional Cardiology. 1(1); DOI: 10.31579/cic-2021/004
Copyright: © 2021 SenDasgupta Chaitali. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 July 2021 | Accepted: 19 August 2021 | Published: 28 August 2021
Keywords: postoperative arrhythmias; lignocaine; magnesium sulphate; amiodarone; open heart surgery; acute atrial enlargement; cardioplegia; ventricular tachyarrhythmias
Background- Postoperative arrhythmias are a serious but frequent complication of open heart surgery. The incidence of postoperative supraventricular arrhythmias has been reported to be 11-54%, and the incidence of ventricular arrhythmias to be 1.8-13% [1]. Various drugs have been tried prophylactically to prevent postoperative arrhythmias including amiodarone, lignocaine and magnesium sulphate.
This study compares the efficacy of amiodarone, lignocaine and magnesium sulphate to placebo in prevention of postoperative arrhythmias in patients undergoing valve replacement surgery under cardiopulmonary bypass.
Materials and methods- This prospective, double blind, parallel group randomized study was carried out in the Cardiothoracic & Vascular Surgery OT and postoperative ICU of IPGME&R and SSKM Hospital, Kolkata in 60 subjects of either sex, 15-65years of age undergoing elective valve replacement surgery. The patients were allocated in three groups comprising 20 patients in each group. Group 1 received normal saline; Group 2 received 3mg/kg of amiodarone; Group 3 received 1.5mg/kg of lignocaine and 40mg/kg of magnesium sulphate just before the release of aortic cross clamp. The frequency of occurrence of supraventricular or ventricular arrhythmias in the 24 hour postoperative period was determined in all groups. Observed data was compiled and analysed using appropriate statistical methods.
Results- There was no significant difference between the 3 groups in the incidence of supraventricular or ventricular arrhythmias in the 24 hour postoperative period.
Conclusion- Single dose of amiodarone, lignocaine and magnesium sulphate have no advantage over placebo in prevention of postoperative arrhythmias.
Running Title:
Prophylaxis of Postoperative Arrythmia
Postoperative arrhythmias are a serious but frequent complication of open heart surgery. The incidence of postoperative supraventricular arrhythmias has been reported to be 11-54%, and the incidence of ventricular arrhythmias to be 1.8-13% [1].
These significantly increase the morbidity of the patients and adversely affect their prognosis. These arrhythmias are multifactorial in origin and thus, their prevention is a challenge requiring knowledge of the predisposing factors which lead to the development of arrhythmias in the postoperative period.
Atrial fibrillation is the most common arrhythmia encountered postoperatively, the incidence varying with the type of cardiac surgery undertaken and the different ascertainment methods used. It prolongs hospital stay, adds to the cost burden, disturbs the patient’s comfort and increases the risk of stroke.
Risk factors for atrial fibrillation include acute atrial changes occurring at the time of surgery, such as acute atrial enlargement, ischaemia and infarction, hypertension, trauma from cannulation, hypomagnesaemia, inflammation caused by pericarditis, cardiopulmonary bypass and cross-clamp times, pulmonary vein venting and beta blocker withdrawal. Other reported risk factors include pre-existing COPD, cardiomegaly, left atrial enlargement, type of cardioplegia, right coronary artery stenosis and sinus nodal or AV nodal artery disease [2].
Ventricular arrhythmias following cardiac surgery include the more common benign isolated ectopic beats or non-sustained ventricular arrhythmias and the dangerous but fortunately less frequent ventricular tachycardia or ventricular fibrillation [3].
Conditions associated with ventricular arrhythmias after cardiac surgery include haemodynamic instability, electrolyte abnormalities, hypoxia, hypovolaemia, ischaemia and infarction, acute graft closure, reperfusion after cessation of cardiopulmonary bypass, and pro-arrhythmia caused by inotropic and anti-arrhythmic drugs [2].
Numerous preventive as well as therapeutic strategies have been studied and used to combat post cardiac surgery arrhythmias.
Many drugs have been used prophylactically in order to prevent postoperative atrial fibrillation (POAF). Amiodarone, which blocks potassium and calcium channels, and has both alpha and beta blocking properties, has been assessed in multiple trials. It can reduce POAF by 50-70% and evidence suggests that ventricular arrhythmias are also reduced. However, there is concern about possible complications including pro-arrhythmia, sudden respiratory distress or bradycardia requiring pacing. Therefore close monitoring is required [3].
Various approaches have been used to prevent or treat post cardiopulmonary bypass (CPB) reperfusion induced ventricular fibrillation. Lignocaine, an amide local anaesthetic, has been shown to increase the threshold for VF by binding to sodium channels, decreasing the slope of phase 4 depolarization and increasing the threshold potential in Purkinje fibres. The administration of lignocaine two minutes before the release of aortic cross clamp not only decreased the incidence of reperfusion ventricular fibrillation, but also increased the cardiac output. Another approach to prevent VF has been the use of magnesium sulphate. The prophylactic use of magnesium after cardiac surgery was better than placebo in reducing the risk of atrial fibrillation, supraventricular and ventricular arrhythmias. The cardiac protective effects of magnesium are induced by the activation of the Na+ K+ ATPase, which stabilizes the membrane potential, and thereby raises the ventricular fibrillation threshold [3].
The aim of this study is to compare the effect of a single prophylactic dose of amiodarone to a dose of lignocaine and magnesium sulphate to placebo on the overall incidence of arrhythmias in patients undergoing valve replacement surgery following the release of aortic cross clamp.
After getting approval from institutional ethics committee and obtaining written informed consent from each of the patients, this prospective, double blind, parallel group, randomized study was conducted in the CTVS OT and postoperative ICU in IPGME&R/SSKM Hospital, Kolkata in 60 patients of either sex, 15-65years of age undergoing elective valve replacement surgery.
Sixty (60) patients aged between 15 to 65 years of either sex were included in the study .The patients were divided into 3 groups: Group 1, 2 and 3 by a computer generated randomization chart. Patients who refused, had any contraindication or allergy to the study drugs, patients taking any of the study drugs in the previous 4 months or taking any drugs known to have significant interactions with the study drugs (e.g. phenytoin, cyclosporine or cholestyramine) were excluded from the study. Group1 (n= 20) received normal saline; Group 2 (n=20) received 3mg/kg of amiodarone; Group 3 (n=20) received 1.5mg/kg of lignocaine and 40mg/kg of magnesium sulphate just before the release of aortic cross clamp in the venous reservoir of the pump.
Written informed consent was obtained from all the patients prior to including them in the study during the pre-anaesthetic visit. Complete pre-anaesthetic evaluation was performed in each patient including detailed history taking, thorough physical examination, airway examination and routine preoperative investigation.
The preoperative left atrial size was measured using M-mode transthoracic echocardiography in parasternal long axis view. Beta blockers and calcium channel blockers and digoxin, if prescribed for rate control, were continued on the day of surgery. All the patients were premedicated with 0.1mg/kg of midazolam intravenously prior to induction.
In the operation theatre electrocardiography, pulse oximetry and non-invasive blood pressure monitoring were commenced. After establishing intravenous cannula and arterial line, general anesthesia was induced by the following drugs intravenously- 5μg/kg of fentanyl, 5mg/kg of thiopentone, 1.2mg/kg of rocuronium. Trachea was intubated with an endotracheal tube of appropiate size. Anaesthesia was maintained with incremental doses of fentanyl, midazolam, isoflurane and vecuronium. The right internal jugular vein was cannulated with a triple lumen central venous catheter. The pulmonary artery pressure was measured directly before going on pump with the help of the surgeon.
Heparin 4mg/kg was administered intravenously to achieve adequate anticoagulation with activated clotted time ≥ 480 seconds. The valve replacement surgery was performed under CPB with mild hypothermia. The CPB circuit was primed with Ringer’s lactate solution, sodium bicarbonate, mannitol and heparin. Haematocrit was maintained between 21 and 28% during CPB. Myocardial protection was achieved by antegrade cold cardioplegia (at 4⁰C, St. Thomas’ solution based crystalloid) after aortic cross clamping and cardioplegia was repeated every 20 minutes. As per Institutional protocol, nitroglycerine 0.5μg/kg/min and dopamine 5μg/kg/min were started at the onset of rewarming. Serum potassium levels were optimized to 4-4.5 mEq/L to minimize arrhythmias induced by hypo/hyper- kalemia. Group 1 patients received normal saline, group 2 received 3mg/kg of amiodarone and group 3 received 1.5mg/kg of lignocaine and 40 mg/kg of magnesium sulphate just before the release of the aortic cross clamp. The drug was prepared according to a computer generated randomization sheet by an anaesthesiologist not involved in the study for the sake of blinding. All the study drugs or placebo were added to the reservoir.
Initial rhythm after the release of aortic cross clamp was noted. When AF was detected cardioversion was attempted with internal paddles with stepwise increase in energy output. When the heart rate was less than 60/min atrial pacing (epicardial) was initiated. If the patient had VF/VT, it was treated with internal defibrillation with stepwise increase in energy upto 50J. If the patient had atrio-ventricular block, AV sequential pacing was initiated. Adrenaline was added for inotropic support to treat persistent hypotension despite 10μg/kg/min of dopamine infusion. Aorta was decannulated after reversal of residual action of heparin by administration of protamine sulphate intravenously. After surgical closure the patients were transferred to the postoperative ICU and monitored for the occurrence of any arrhythmias for a 24 hour period. Arrhythmias were treated as and when they occurred. The study ended after 24 hours of postoperative period.
Statistical Analysis
The software used for statistical analysis was Statistica version 6 [Tulsa, Oklahoma: StatSoft Inc., 2001]. Sample size was calculated on the anticipated incidence of spontaneous return to normal sinus rhythm following release of aortic cross clamp. Assuming, based on published literature7 that 46% of patients in the placebo group will not demonstrate spontaneous return to normal sinus rhythm it was calculated that 19 subjects would be required per group for a 20% reduction in proportion of patients not returning to sinus rhythm with 80% power and 5% probability of type I error.
The numerical variables which were normally distributed were : age, body weight, pre- and post-operative LA size, pre-operative pulmonary artery pressure, duration of CPB, aortic cross clamp time, total duration of surgery, pO2, pCO2, K+ and all other lab parameters (Hb%, FBS, urea, creatinine) and they were compared between the three groups using one way ANOVA. The numerical variables which were not normally distributed included: ejection fraction, drug doses, defibrillation energy required, duration of pacing, duration of intubation, ICU stay and they were compared between the three groups using Kruskal-Wallis ANOVA. The categorical variables were compared using the Chi- Square test.All statistical analyses were two-tailed and p <0>
The three groups were comparable with respect to all baseline variables including age, body weight, sex, NYHA class, haemoglobin, fasting blood glucose, blood urea and serum creatinine, pre- and post-operative LA size, pre-operative pulmonary artery pressure and ejection fraction. (Table-1)
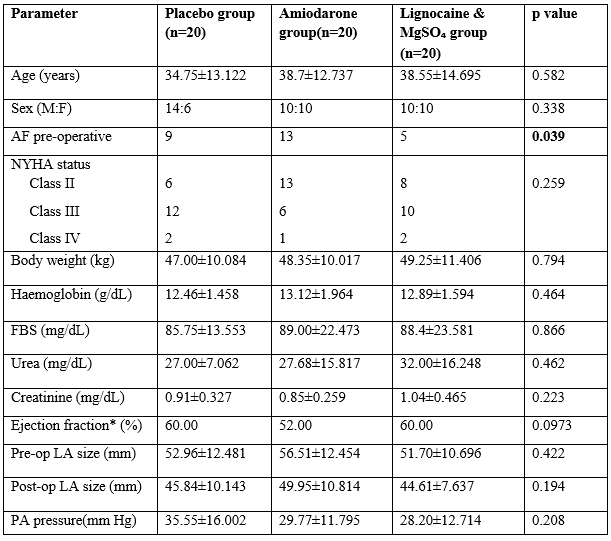
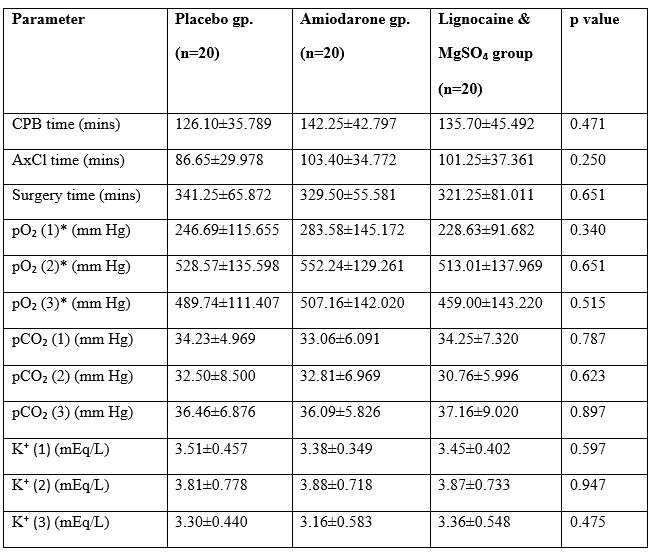
The groups were also comparable with respect to intraoperative factors which might have affected outcome including CPB, aortic cross clamp and surgical durations, pO₂, pCO₂ and K⁺ concentrations just after induction, after weaning from CPB and just after surgery (Table-2).
However, statistically significant differences (p value = 0.039) were noted between the three groups in the presence of pre-operative atrial fibrillation which may have affected the outcome (Table-1).
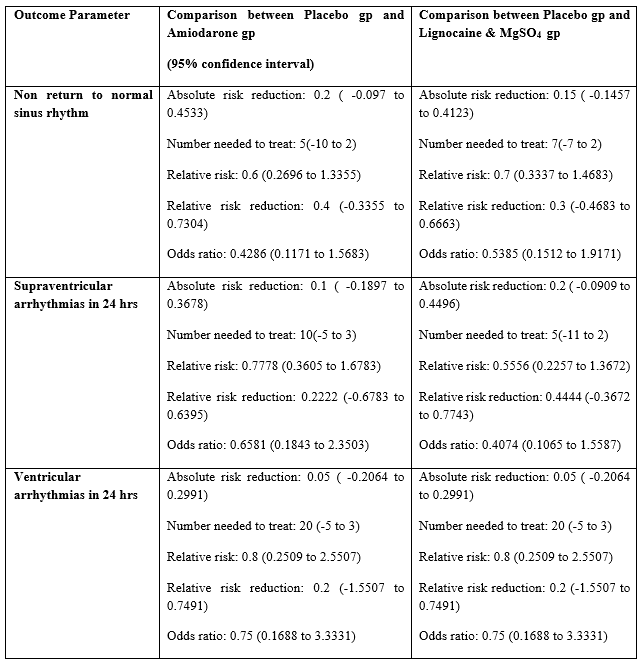
Spontaneous return to normal sinus rhythm after removal of the aortic cross clamp, without the need for pacing or defibrillation was seen in 10[0.5{95% C.I- 0.2993 to 0.7007}] out of 20 patients of the placebo group, 14 patients [0.7{95% C.I- 0.4810 to 0.8545}] of the amiodarone group and 13 patients [0.65{95% C.I- 0.4329 to 0.8188}] of the lignocaine and magnesium sulphate group. However, these differences were not statistically significant (p value = 0.399) (Table-3).
The incidence of supraventricular arrhythmias within 24 hours in the three groups were- 9 patients [0.45{95% C.I- 0.2582 to 0.6579}] of the placebo group, 7 patients [0.35{95% C.I- 0.1812 to 0.5671}] of the amiodarone group, 5 patients [0.25{95% C.I- 0.1119 to 0.4687}] of the lignocaine and magnesium sulphate group. These differences were statistically insignificant (p value =0.415) (Table-3). The incidence of ventricular arrhythmias within 24 hours of surgery was 5 patients [0.25{95% C.I- 0.1119 to 0.4687}] in the placebo group, and 4 patients [0.2{95% C.I- 0.0807 to 0.4160}] each in the amiodarone group and lignocaine and magnesium sulphate group. These differences were also statistically insignificant (p value =0.906) (Table-3).
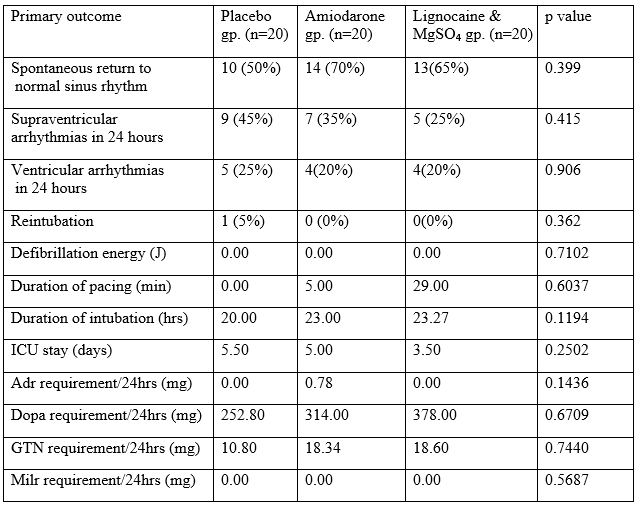
No statistically significant differences were also found between the three groups with respect to defibrillation energy requirement, pacing duration, duration of intubation and ICU stay (Table-3). Reintubation was required in only one patient in the placebo group (Table-4).
Atrial fibrillation is the most common arrhythmia encountered postoperatively following cardiac surgeries under cardiopulmonary bypass. Ventricular tachyarrhythmias after reperfusion following CPB, though fortunately less common are more dangerous. Amiodarone, lignocaine and magnesium sulphate have all been individually shown to be effective in the prevention of postoperative arrhythmias. While amiodarone and magnesium sulphate have been proved to be effective against both supraventricular and ventricular arrhythmias, lignocaine is primarily effective against ventricular arrhythmias [1].
There have been many trials to demonstrate the efficacy of amiodarone in preventing postoperative atrial fibrillation as well as ventricular tachyarrhythmias. Mitchell et al in the PAPABEAR trial compared oral amiodarone (10mg/kg/day) for 6 days prior to surgery to placebo. Amiodarone significantly reduced (p<0>
MT Moeen Vaziri et al, studied 76 patients undergoing CABG, comparing the effect of prophylactic lignocaine to magnesium sulphate and normal saline in preventing ventricular fibrillation. They found that both lignocaine and magnesium sulphate decreased the incidence of ventricular fibrillation, magnesium sulphate more than lignocaine [6].
O. Tiryakioglu et al studied 192 patients undergoing CABG surgery. They compared magnesium sulphate given intravenously 12 hours prior to operation, immediately following the operation, and on postoperative days 1, 2 and 3 to a preoperative infusion of amiodarone (1200 mg) on first postoperative day followed by oral amiodarone (600mg/day), to normal saline inthe control group during the same time periods. This study found that prophylactic amiodarone for total (both ventricular and supraventricular) arrhythmias was significantly more effective than magnesium sulphate (p=0.015). There was no difference between the two drugs in preventing supraventricular arrhythmia (p=0.026) [1].
S.Kar et al studied 56 patients undergoing valve replacement surgery and compared the prophylactic efficacy of a single preoperative dose of amiodarone to placebo. They found that amiodarone significantly decreased the incidence of atrial fibrillation (p=0.035), ventricular fibrillation (p=0.089) and increased the incidence of spontaneous reversion to normal sinus rhythm after cross clamp release (p=0.002) [7].
Ayoub CM et al compared amiodarone to lignocaine and placebo, given 2 minutes before cross clamp release for prevention of ventricular fibrillation in 120 patients undergoing CABG.The study showed no difference between amiodarone and placebo in prevention of ventricular fibrillation after release of aortic cross clamp. In addition, the use of lignocaine was able to reduce the incidence of ventricular fibrillation as compared to both amiodarone and placebo [8].
In a similar study comparing amiodarone, lignocaine and placebo William J. Hauermann et al found that neither amiodarone nor lignocaine reduced the incidence of ventricular fibrillation in patients undergoing a variety of cardiac surgeries. However, amiodarone was shown to reduce the number of shocks required to terminate a ventricular fibrillation [9].
Another study by A A Ghavidel et al comparing amiodarone, lignocaine and placebo on 150 patients showed no significant difference in the incidence of VF after aortic cross clamp release between groups [10].
In our study however, there was no significant difference in the rate of spontaneous reversion to sinus rhythm between the placebo, amiodarone, lignocaine and magnesium sulphate groups. Neither was any difference seen in the incidence of atrial fibrillation or ventricular arrhythmias within 24 hours. Amiodarone and lignocaine and magnesium sulphate also failed to show any significant advantage over placebo in terms of decreasing the defibrillation energy requirement, duration of pacing, intubation and hospital stay in our study. Though similar findings were reported by William J Hauermann et al and A A Ghavidel et al, majority of the studies show amiodarone, lignocaine and magnesium sulphate to be effective against postoperative arrhythmias. However, in our study we have used a single dose of the agents just before the release of cross clamp, whereas most studies have used different regimens of the study drugs. Another fallacy of our study was that despite randomization, a significant difference in the incidence of pre-existing atrial fibrillation crept between the groups which may have affected the outcome.
A single prophylactic dose of amiodarone or lignocaine and magnesium sulphate did not decrease the incidence of atrial fibrillation or ventricular arrhythmias or increase the rate of spontaneous reversion to normal sinus rhythm in patients undergoing valve replacement surgery.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
