AUCTORES
Globalize your Research

Short communication | DOI: https://doi.org/10.31579/2578-8868/131
1 Neurology, Taikang Xianlin Drum Tower Hospital, Nanjing University School of Medicine, Nanjing, China
*Corresponding Author: Shucheng Gang, Department of Neurology, Taikang Xianlin Drum Tower Hospital, NO.188 Lingshan North Road, Qixia District, Nanjing 210046, Jiangsu, China.
Citation: Wang L, Zhang Y, Geng T, Li M, Wang Q, Liu, Xie T, Gang S., (2020) From the onset to large vessel occlusion—what matters?. J. Neuroscience and Neurological Surgery. 6(5); DOI:10.31579/2578-8868/131
Copyright: © 2020 Shucheng Gang, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 21 July 2020 | Accepted: 03 August 2020 | Published: 07 August 2020
Keywords: Intravenous thrombolysis therapy; Mechanical thrombectomy; blood clot
Intravenous thrombolysis (IVT) therapy is being questioned nowadays for eligible patients prepared to receive mechanical thrombectomy. We reviewed some large randomized controlled clinical trials and observational cohorts and discussed the efficacy and necessity of intravenous thrombolysis.
Whether intravenous thrombolysis therapy should be given as pretreatment before mechanical thrombectomy for acute ischemic stroke due to large vessel occlusion (AIS-LVO) has been a hot issue since the last few years even current guidelines advocate [1]. The main controversy is whether the benefits outweigh the risks for patients in terms of intravenous thrombolysis pretreatment. One of the arguments is the low rate of recanalization for LVO [2].
Truthfully, according to a meta-analysis of randomized controlled clinical trials and observational cohorts, 1 out of 10 patients with LVO causing stroke had successful recanalization after intravenous thrombolysis alone [3]. However, further study revealed that early recanalization of LVO with only intravenous thrombolysis was associated with 61.7% independence rate at 90 days and similar successful reperfusion rates (mTICI2b/3) compared to LVO treated with endovascular treatment, with or without previous intravenous thrombolysis. Furthermore, intravenous thrombolysis was not independently associated with symptomatic intracranial hemorrhage, parenchymal hematoma, or subarachnoid hemorrhage [4].
The points are that how long is the time from the onset to initiation of alteplase infusion (OTBT, onset to bolus time) and are there any features on the baseline head computed tomography (CT) that predict early recanalization with greater possibility?
As we know, arterial thrombosis is a process that involves in activating coagulation cascade under different circumstances which also generally determine the speed of thrombosis or the length of thrombus such as hypercoagulable or hypoperfusion states, stenosis of cerebral arteries, vulnerable plaques, drugs being taken, the patients’ functional states, etc [5]. Theoretically, there also exists a time window from the onset (or more accurately the beginning of thrombosis) to complete formation of LVO and ideally the process of thrombosis can be terminated by means of thrombolytic therapy during the time window, which needs to have thrombolytic drugs administered as early as possible.
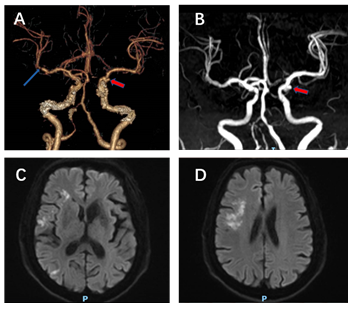
However, the onset to bolus time seemed still “long” from some available published data with average 131 minutes [3]. If given earlier within golden hour (≤60min from symptom onset), for example, in the settings of mobile stroke units, intravenous thrombolysis may have greater potential for successful reperfusion of LVO. Recently, we treated a patient complaining of sudden palsy of left limbs. We gave the patient alteplase with a standard dosage of 0.9mg per kilogram of body weight (10% administered as a bolus first, then 90% infused over a period of 1 hour) immediately after the head CT scan was completed. During the infusion procedure, we completed the computed tomography angiography (CTA), found an abnormal sign located in the right middle cerebral artery (MCA). In the following 3 days, the patient’s symptoms were dramatically improved, and the right middle cerebral artery was nearly normal showed on magnetic resonance angiography (MRA) with multiple sporadic fresh ischemic lesions on diffusion weighted imaging (DWI) series (figure 1).
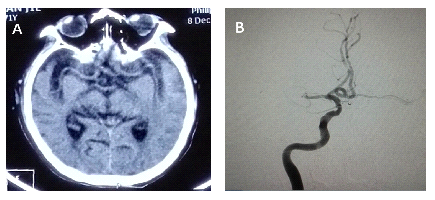
On the other hand, one fact which cannot be neglected in China is that fewer hospitals in which endovascular treatment can’t be performed are willing to treat acute ischemic stroke doubtfully caused by LVO since thrombectomy was recommended in the past few years. Patients have to be transported from primary centers directly to tertiary care centers, consuming valuable time during the transportation. Another patient we treated earlier complaining of progressive weakness of left limbs was transported to our center because of an intracranial hemorrhage history. No apparent abnormalities were showed on the head CT scan completed after the onset with symmetrical normal signs of bilateral middle cerebral arteries. While digital subtraction angiography (DSA) performed 4 hours later after the onset showed complete occlusion of the right middle cerebral artery (figure 2).
The two examples perhaps can give us a hint of LVO forming process in real world which ends up finishing completely with enough time or probably can be discontinued if treated with thrombolytic therapy as early as possible.
Recently the DIRECT-MT investigators published their results which showed that going directly to endovascular treatment was non-inferior to the use of intravenous thrombolysis before or during the procedure with regard to functional outcomes [6]. We noticed that in the group that received alteplase before thrombectomy (combined –therapy group), only a few patients had the alteplase infusion completed before groin puncture while the majority of patients had the infusion completed during the endovascular procedure. As one of the secondary outcomes, with inadequate time that was allowed for alteplase to act before endovascular treatment was initiated, the percentage of patients with successful reperfusion before thrombectomy was still apparently higher in the combination-therapy group than in the thrombectomy-alone group. Given earlier or more time, alteplase will probably play a bigger role in the treatment strategy.
Actually, we observed successful reperfusion from 9 patients suffering from AIS-LVO and receiving alteplase alone with standard dosage as mentioned above from June 2017 to May 2020 in our center. The occluded arteries, which mostly led to multiple sporadic lesions distributed in their supply areas confirmed by DWI series after intravenous thrombolysis, were recanalized well showed on subsequent CTA or MRA. Two major features revealed on head CT scan after the onset were as follows: first, the decrease of Alberta Stroke Program Early CT Score(ASPECTS) was not found, which meant the morphological structures of the affected brain area were still normal; second, there were no high density signs on the affected arteries. More data should be observed and analyzed to evaluate the efficacy of intravenous thrombolysis therapy for patients who had good outcomes with AIS-LVO by receiving intravenous thrombolysis alone.
From above, we favor that time is still a key factor for patients with AIS-LVO and intravenous thrombolysis should be performed with no delay for eligible patients instead of going directly to endovascular procedures [7].
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

















































