AUCTORES
Globalize your Research

Case Reports | DOI: https://doi.org/10.31579/2641-5194/012
1.General Surgeon, ABC Medical Center, Mexico.
2.General and Bariatric Surgeon, ABC Medical Center, Mexico.
3.General Surgery Resident, Durango Hospital, Mexico.
*Corresponding Author: Pablo Magaña Mainero, General Surgeon, ABC Medical Center, Mexico City.E-mail:drpablomaganam@gmail.com
Citation: Pablo Magaña Mainero, Carlos Alberto Gutiérrez Rojas, Andrés Olivares Rónces and Ángel Martínez Munive, Gastric Bypass Reversion with Henley-Longmire Intestinal Loop, Surgical Treatment of Recurrent Marginal Ulcer - A Case Report, J. Gastroenterology Pancreatology and Hepatobilary Disorders, 4(1): DOI: 10.31579/2641-5194/012
Copyright: © 2021 Pablo Magana Mainero. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 March 2020 | Accepted: 25 March 2020 | Published: 03 April 2020
Keywords: marginal ulcer; gastric bypass; reverse bypass; henley-longmire intestinal loop; surgical treatment; abdominal tomography
Bariatric surgery complications are associated with the nature of the procedure, reaching an incidence of 40%. One of them is the marginal ulcer, which is defined as a peptic ulcer produced over the jejunal mucosa, distal from the gastro-jejunal anastomosis. Its reported frequency ranges from 0.6 to 25% in gastric bypass patients.
Associated risk factors are bad tissue perfusion by increased tension of the anastomosis, foreign bodies as stiches or staples, acidic exposure from gastric fistula, non-steroid anti-inflammatory drugs, tobacco and infection by Helicobacter Pylori.
Female patient operated with Roux en “Y” Gastric bypass for obesity, 7 months after the first surgery she required emergency surgery with laparotomy due to postsurgical complications. 3 months after this event she was diagnosed with malnutrition and almost 1 year after the initial GB she presented to the ER with abdominal pain, distension and involuntary muscle resistance. She was admitted to the ER with tachycardia, bilateral hypoventilation and abdominal pain. A CT-scan revealed hollow viscera perforation.
Pouch gastrectomy and anastomosis of the gastric remnant with the Henley-Longmire jejunal loop technique for reverse bypass procedure was performed successfully.
The gastric bypass reversion is essential for long term complications that do not respond to initial treatment, such as the recurrent marginal ulcers, dumping syndrome, hiatal hernias, refractory hypoglycemia’s, nesidioblastosis, and hypocalcemia.
In 2016 alone, almost 40% of adults worldwide, 18 years old or older, were considered overweight [1]. With the increase in obesity rates, it is not surprising that the number of bariatric surgeries performed has increased in the last two decades [4, 5]. The complications of bariatric surgery are related to the nature of the procedure and have been reported with an incidence of up to 40%. For the Gastric Bypass (GB) the most frequent are: marginal ulcer (MU), gastric remnant distention (> 50 mL), anastomosic stenosis, bleeding and gastro-gastric fistula, among others [6]. MU is defined as a peptic ulcer produced in the jejunal mucosa just distal to the gastro-jejunal anastomosis, after a partial gastrectomy for a benign disease or bariatric GB. Its frequency has been reported between 0.6 and 25% in patients with GB [2]. The symptoms associated with the presence of a marginal ulcer are: epigastric pain and heartburn in 56.8% of cases, dysphagia in 36%, nausea and vomiting in 18 to 58% and bleeding from the upper gastrointestinal tract in 5.1% of cases. However, these typical symptoms do not occur in most of cases and even some patients do not refer any symptoms at all [7]. The incidence of perforation in patients with marginal ulcer is reported to 20% in normal population and 1 to 2% in the population with gastric bypass [2]. Surgical treatment for MU takes place in the case of dilatation of the gastric remnant and gastro-gastric fistula, as well as in the complications associated with it, such as retraction and perforation [3]. In patients with recurrence of these complications, GB reversal is performed as a definite treatment [8].
Throughout history, different surgical techniques have been used to restore intestinal transit after a total gastrectomy. The most widespread techniques today are Roux's jejunal Y-handle, as well as Tomoda's loop [9], however, they are not the only reconstructions described.In the year 1952, the Henley-Longmire loop was described by the same authors, this reconstruction y performed by the interposition of a jejunum loop between the esophagus and the duodenum [10, 11, 12], and was even described for the instestinal transit restitution after a partial gastrectomy [11], however, it is a technique rarely used [9]. It is important to mention the gap of knowledge for this particular complication and surgical procedures for definitve management. The lack of RCT´s and guidelines appears as an area of opportunity to further expand our current knowledge.
A 47 year old female patient with history of grade 3 obesity, treated with a “Y” en Roux GB in in February 2016. In October of the same year, MU in the gastro-jejunum anastomosis with secondary anastomotic stenosis, it required revision of the GB, an antecolic conversion and remodeling of the gastro-jejunum anastomosis with distalization of 40 cm of the jejunum-jejunum anastomosis at the expense of the alimentary loop was done. 24 hours after the procedure, she presented with anastomotic leak symptoms of the jejunum-jejunum (J-J) anastomosis, requiring a new emergency Laparotomy in which a reconstruction of the J-J anastomosis was performed, afterwards she recovered succesfully and was discharged.
In January 2017 she was diagnosed with protein-caloric malnutrition, which was managed with multivitamin nutritional support and polymeric diet. In July 29th 2017, she presented acute abdominal pain and was reffered to an unspecified ER unit, where an endoscopy was performed, showing perianastomotic gastric ulcers. After the study, she presented with increased abdominal pain, distention and involuntary muscular resistance associated with hypotension. Upon admission to our hospital; mild dehydration, paleness, tachycardia, bilateral pulmonary hypoventilation, painful abdomen on superficial palpation, with involuntary muscular resistance, positive rebound sing and decreased peristalsis were documented. An endoscopic study was performed and findings showed large ulcerated areas at the level of the gastric pouch (figure 1).


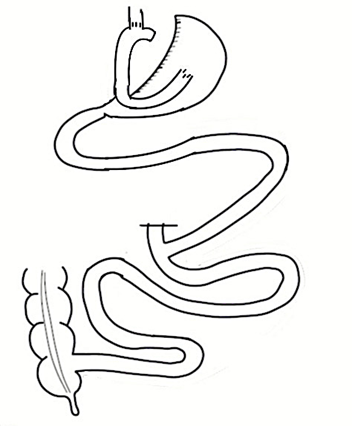
A CT-Scan revealed images suggestive of hollow viscera perforation (figure 2). She then was transferred to the OR for and Emergency Laparotomy, in which we found massive pneumoperitoneum, generalized peritonitis and gastric ulcer perforated at the level of gastric pouch in the anterior wall, a pouch gastrectomy and esophagogastric anastomomis resecction was required as well as Retrocolic Interposition of Henley-Longmire Jejunal Loop (RIHLJL) (esophagus-jejunum anastomosis and jejunum-gastro anastomosis to stomach remnant) for reverse bypass fabrication (Figure 3).
The patient evolved positively on the postoperative period and remained asymtomatic, with significant clinical improvement, beginning oral intake on postoperative day 3 with good tolerance, when she remained under observation and was discharged without complications in the postoperative day 8. Finally, an esophagogram study with hidro-soluble contrast was performed to confirm absence of stenosis or anastomotic leaks (Figure 4).

Nowadays, we can still consider the RIHLJL as an option for restoring intestinal transit in very particular situations. We found no reported cases of jejunal replacement in the literature for GB reversal as in our case, however, back in the 1950's when the article was published, it describes the case of a patient in whom an interposition of a jejunal loop was performed with restitution of the intestinal transit after a total gastrectomy [10,12]. Subsequently, some authors have published their experience of jejunal replacement after total gastrectomy [9].
In this case, when resecting the gastric pouch due to the great damage caused by the perforation of the recurrent MU, in addition to a firmly adhered gastric remnant, it was considered to perform a variant of the previously described technique to achieve the restoration of intestinal transit, performing an esophagus-jejunum anastomosis and a jejunum-gastric anastomosis to the remaining stomach, in order to make a reversal of the GB. The interposed loop was obtained from the Roux limb to avoid performing another anastomosis in the small bowel.
The incidence of perforation of the MU is 20% in general population and 1 to 2% in the population with GB, surgical treatment is definitive. In cases of recurrent ulcers, the reversal of GB plays an important role and it is performed as a treatment as in our case. The first step of the surgical technique for the reversal of GB is the release of adhesions and dissection of the Gastric pouch to perform transection at the level of the gastro-jejunum anastomosis. Subsequently, the mobilization of the gastric remnant is performed avoiding revascularization. The following is the movilizacion of the Roux limb. The surgical decisions are based on the length of the limb: in the case of a short limb, resection, in a long one, reanastomosis. Other authors preserve a Roux limb of 15 to 20 cm. The last step is the construction of the gastro-gastric anastomosis, this technique varies depending on the experience and preference of the surgeon.
Today, we can still consider the Henley-Longmire Loop as an option for the restoration of intestinal transit in cases such as ours, that when resecting the gastric pouch and finding a firmly attached gastric remnant made it technically impossible to perform the gastro-gastric anastomosis (which would be the first option), followed by a vertical gastrectomy to preserve the restrictive benefits of the initial procedure. We performed a variant of this technique to achieve the restitution of intestinal transit, performing an esophagus-jejunum anastomosis and a jejunum-gastric anastomosis to the remaining stomach, in order to make a reversal of the GB. The interposed loop was obtained from the Roux limb to avoid performing another anastomosis of the small bowel.
The complications of bariatric surgery, particularly in gastric bypass, represent a mayor challenge, even for an experienced surgeon, it is important to take into consideration the surgical options available to face these complications, hence the patient's life will depend on the success of the procedure.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.
















































