AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2578-8949/059
1 Resident at the Department of Dermatology and Venerology, Faculty of Medicine, Tishreen University, Lattakia, Syria.
2 Professor at the department of Dermatology and Venerology, Faculty of medicine, Tishreen University, Lattakia, Syria.
*Corresponding Author: Nora Harfouch, Resident at the Department of Dermatology and Venerology, Faculty of Medicine, Tishreen University, Lattakia, Syria
Citation: Nora Harfouch (2019), Staphylococcus Aureus Colonization In Atopic Dermatitis Patients, J.Dermatology and Dermatitis.4 (3); DOI:10.31579/2578-8949/059
Copyright: © 2019 Nora Harfouch, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 October 2019 | Accepted: 08 November 2019 | Published: 13 November 2019
Keywords: Atopic dermatitis – Colonization – Staphylococcus aureus – SCORAD- Swabs – Cultures
Background:Atopic dermatitis (AD) is a common chronic inflammatory skin disorder that induces several symptoms including pruritus and dryness, and is often associated with secondary cutaneous infections. AD is considered to be one of the most prevalent and studied skin diseases yet poorly understood, and its pathophysiology remains obscure. Even though other skin diseases (such as psoriasis) share the same pathologic factor -skin barrier defect - with atopic dermatitis, patients diagnosed with those diseases don't suffer infectious exacerbations like atopic patients do.
Aim: Although many international researches have already discussed the relationship between staphylococcus aureus and AD, no studies about this subject in the Arabic region was documented. The aim of our study is to compare staphylococcus aureus colonization rates and densities between atopic dermatitis patients and non-atopic subjects, and to relate the colonization to the severity and duration of the disease.
Materials and methods: This observational analytic study included 200 participants (99 diagnosed with atopic dermatitis and 101 control subjects without atopic dermatitis); nasal and skin swabs (lesional and non-lesional) were collected from patients, while nasal and only normal skin swabs were collected from controls. Positive swabs were assessed to determine the density of colonization.
Results: 57.6% of patients had nasal colonization, 56.6% had lesional colonization and 30.3% had normal skin colonization. Nasal colonization rates and densities were higher in the patients group. We detected a correlation between colonization and severity of eczema, but no correlation between colonization and duration of the disease was detected.
Conclusion: The high rates and densities of staphylococcus aureus colonization in lesional skin of atopic dermatitis patients point out the role of these organisms in the pathophysiology of the disease, put antibiotics on the treatment list of atopic dermatitis and explain infectious features in AD exacerbations.
Atopic dermatitis (AD) is a common chronic, relapsing inflammatory skin condition characterized by pruritus and erythematous patches with typical morphological features and distribution(1). It is often the first manifestation of the ‘atopic march’, which refers to the typical natural history of the atopic disorder. AD is often followed by allergic rhinitis and subsequently asthma, though conditions may overlap(2).
Some of the most valuable AD prevalence data have come from the International Study of Asthma and Allergies in Childhood (ISAAC) (3),Which revealed that the prevalence varies greatly throughout the world.
For the age group 6-7 years, data showed that the prevalence of AD ranged from 0.9% in India to 22.5% in Ecuador, with new data showing high values in Asia and Latin America. For the age group 13-14 years, data showed prevalence values ranging from 0.2% in China to 24.6% in Columbia. A prevalence over 15% was found in 4 of 9 regions studied including Africa, Latin America, Europe and Oceania (4).
Importantly, the latest available data (Phase Three of the ISAAC study)(5) showed that while AD seems to have reached a plateau in the countries with the highest prevalence such as the UK and New Zealand, AD continues to increase in prevalence, specifically in young children (age 6-7 as compared to age 13-14 years) and in low-income countries, such as Latin America or South East Asia which have emerged as regions of a relatively high prevalence in the follow-up data (6).
Atopic dermatitis has a complexed multifactorial etiology. Despite the better understanding that we have today about these factors (Genetics– skin barrier dysfunction– immunologic defects– microbiota imbalance), the exact pathophysiology remains unclear. But in general it is considered that all factors contribute to a vicious circle that lead to the chronicity and relapsing of atopic dermatitis.(7)(8)
Factors related to the pathophysiologic mechanism of AD:
1- genetics: The generation of FLG degradation products, urocanic acid and pyrrolidine carboxylic acid, contributes to SC (Stratum Corneum)hydration and acidic pH of skin. Mutations in filaggrin protein gene impair skin barrier function and increase the risk of AD.(9)
2-immune dysregulation: characterized by the over-expression of type 2 immune cytokines, e.g., IL-4 and IL-13, which play an important role inchemokine production, skin barrier dysfunction, suppression of antimicrobial peptides (AMP), and allergic inflammation(10). Although blockade of type 2–driven inflammation improves AD symptoms, the pathogenesis of AD is not exclusively explained with Th2 immunity(11).
3- Epidermal dysfunction: A damaged epidermal barrier contributes to the mechanism of AD, as it heightens sensitization to allergens. Altered lipid composition - necessary to maintain theintegrity of the epidermal barrier- is observed in lesional and non-lesional AD skin. (12)
IL4-IL13-IL31-IL33 down-regulate the production of epidermal barrier proteins, including FLG, keratins, loricrin, involucrin,and cell adhesion molecules.(13)
4- Microbiome: AD skin has decreased bacterial diversity.(14)
A currently favoured theory in AD pathogenesis is the “outside-in” hypothesis, where an impaired epidermal barrier, allowing penetration of environmental substances into the skin, is described as the starting point in an early march towards atopy (15).
Atopic dermatitis has three distinguished phases symptomatically:
1- AD in infants: It develops during the first two years and characterized by acute eczematous lesions consisting of erythematous, itchy exudative/excoriated papules or plaques with vesicles, affecting mainly the cheeks, neck and scalp.
2- AD in childhood: This phase takes place between 2years old and puberty, and consists of dry lichenoid papules and plaques distributed on the ankles, wrists, hands, feet and flexor areas. Facial involvement is uncommon in this phase.
3- AD in adults: It affects the face, neck, eyelids, nipples and extremities consisting of symmetric dry scaly papules or plaques. The presence of exudation in this phase is a sign of secondary infection.(16)
The skin of AD patients is normally colonized and may be infected with various microorganisms, including bacteria, fungi and viruses. Although there are defects inthe skin barrier, other skin diseases - such as psoriasis - rarely coexist with secondary infections(7).
Species-level investigation of AD has shown a higher predominance of S. aureus in patients withmore-severe disease and an abundance of S. epidermidisin patients with less-severe disease.(17)
As mentioned above, AD patients have corrupted innate immunologic skin defenses against multiple organisms including SA and suppression of antimicrobial peptides (AMP). In addition, an experiment conducted in 2005 revealed that AD patients expressed reduced amounts of several DCD-derived peptides in sweat. When comparing antimicrobial activity of sweat in vivo between healthy individuals and AD patients, it was noted that sweating leads to a reduction of viable bacteria on the skin surface in healthy people, this does not occur in patients with AD(18).
Patients with AD have been found to have reduced TLR function, and impaired production of keratinocyte derived antimicrobial peptides needed to control S. aureus and viral replication(19).The over-expression of TH2 cytokines (IL4-IL13-IL31-IL33) in atopic dermatitis patients down-regulates the production of epidermal barrier proteins, and cell adhesion molecules(13). Each one of these factors may predispose to microbial colonization and chronic skin inflammation.
S. aureus colonizes AD skin and has a pivotal role in the development and exacerbation of AD: it induces T-cell– independent B-cell expansion, up-regulates pro-inflammatory cytokines such as TSLP, IL-4, IL-12, and IL-22; and stimulates mast cell degranulation, which results in Th2 skewing and skin inflammation.(17)
While there is a strong link between acute S. aureus infection of the skin and the increase in AD severity, the role of colonization in the pathogenesis and maintenance of AD remains unclear. (20)
As it is noted that atopic patients has a higher tendency to develop skin and soft tissue infections. This study was conducted to evaluate the colonization rates and densities of staphylococcus aureus in the skin and nasal cavaties of patients with atopic dermatitis and to compare it with non-atopic individuals. Although many researches have already discussed the relationship between staphylococcus aureus and AD, no researches in the Arabic region were documented concerning this dilemma, and we found it important to conduct such a study, as atopic dermatitis is very common in our society, and causes discomfort, embarassment and depression, as it could be refractory to many treatment protocols.
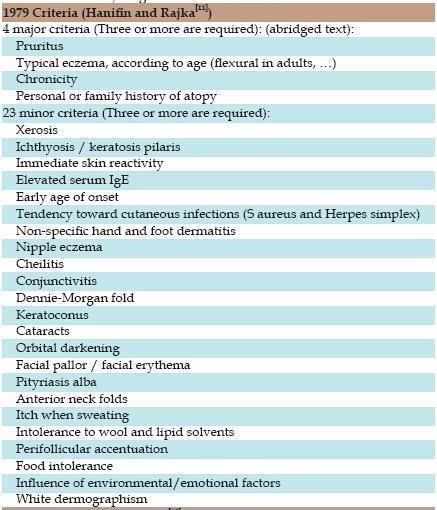
Our study that took place between May 2018 and May 2019, included 200 participantsof all age groups, 99 of which had atopic dermatitis according to the criteria of Hanifin&Rajka*(21),and 101non-atopic individuals who had no personal or familial history of atopy.
1- A history of systemic or topical treatment with antibiotics during the last month.
2- A history of immunosuppressive treatment during the last month.
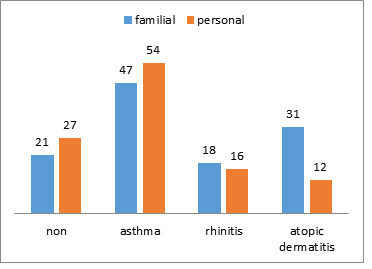
collected data included: {age- sex- phone number- address- atopic dermatitis duration- history of personal atopy manifestations before enrollment in the study /asthma-rhynitis-AD /- familial history of atopic manifestation/asthma-rhynitis-AD/}
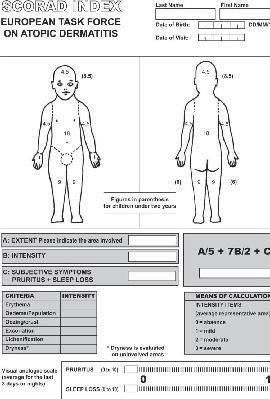
Each patient was clinically assessed to determine the severity of AD using the scale of SCORAD**(22) patients were classified according to SCORAD value into 3 groups as follows:

Six swabs were collected from each AD patient, four of which were from skin and two from nasal cavities. Skin swabs consisted of two lesional eczematous, and two non-lesionalswabs.
Cultures were collected using sterile swabs dipped in normal saline solution; pressed over the skin for 30 seconds on each site, and rotated in 360˚ round motion in each nostril for nasal swabs.
On the other hand, four swabs were collected the same way from each non atopic participant; two skin swabs from the cubital fossae, and the other two from nasal cavities.
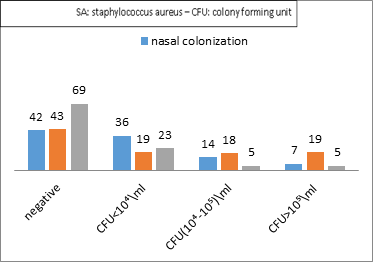
Specimens were delivered to the microbiology lab on the same day for staphylococcus aureus detection. Density of colonization was then determined and classified according to CFU(Colony Forming Units) into:
Mild: CFU<10⁴/ml
Moderate: CFU(10⁴-10⁵)/ml
Severe:CFU>10⁵/ml
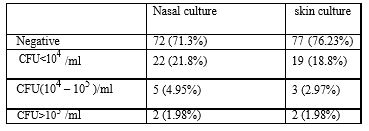
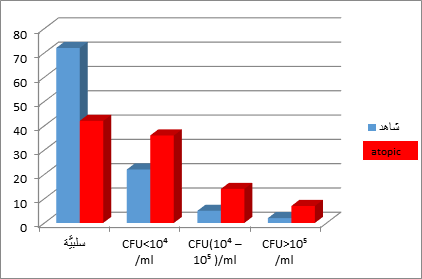
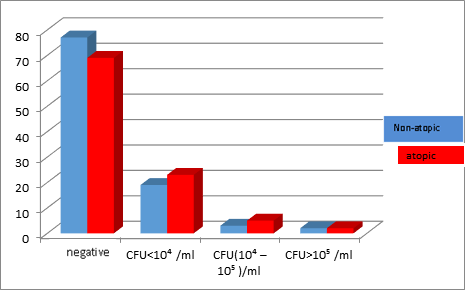
57.6 %of atopic patients had colonization in their nostrils compared to 28.7% in non-atopic individuals. 56.6% of atopic patients had lesional skin colonization and 30.3% had non-lesional skin colonization compared to 23.8% in non-atopic individuals.(T1-T2)
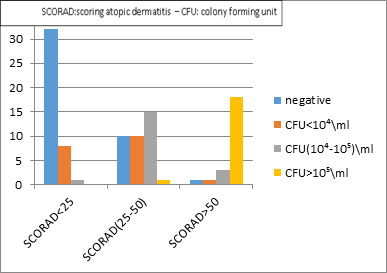
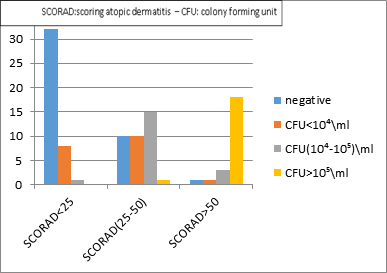
Out of 23 patients with severe AD we recorded 18 with nasal colonization (78.26%), 4 patients (17.4% ) had nasal colonization density >10⁵/ml (D4)
Out of 23 patients with severe AD we recorded 22 patients (95.65% )with lesional skin colonization, 18 patients(78.26%) had lesional skin colonization density >10⁵/ml (D5)
Out of 23 patients with severe AD we recorded 15 patients (65.2% )with non-lesional skin colonization. 2 patients(8.7%) had non- lesional skin colonization density >10⁵/ml (D6)
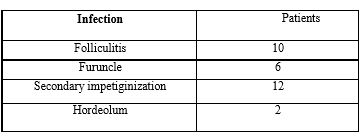
Out of 23 severe atopic dermatitis patients, 18 had concomitant infections, and some of them had more than one infectious manifestation simultaneously. (T3)
Comparing rates and densities of SA cultures in atopic and non-atopic individuals shows higher rates and densities in the atopic group regarding nasal cultures, but approximately compatible values in the skin cultures. (D7-D8)
Treating the data of patients with Spearman–Brown prediction formula revealed: statistically significant correlation between:
1- age and AD severity
2- AD severity and the rate and densities of colonization in each of the three collected sites.(Correlation significance at the level of 0.05) (D4-5-6)
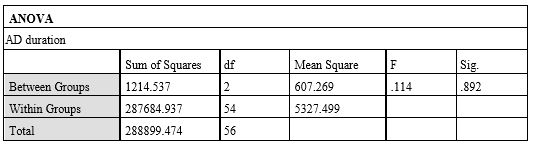
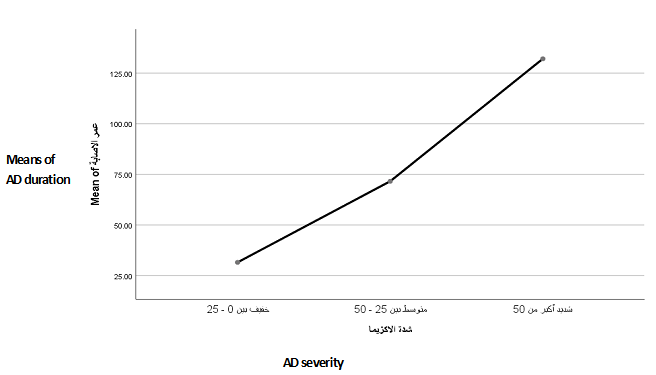
3- AD duration and AD severity, when comparing the means of AD duration between the three groups of severity using the ANOVA test, we found a statistically significant correlation between AD severity and AD duration in the mild and severe categories, which means that mild AD was compatible with short disease duration, while severe AD was compatible with long duration. (T4) - (D9)
4- AD duration and lesional skin colonization, with no correlation between AD duration and colonization in the nose or the normal skin.(Correlation significance at the level of 0.05) (T5)
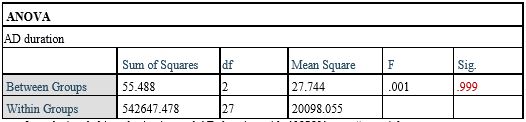
To better understand this relation, we used the ANOVA test in order to determine the effect of AD duration on the densities of cultures after the exclusion of negative culture specimens from each site.(Correlation significance at the level of 0.05), We found no correlation between the variables, which means there is no correlation between duration of AD and the density of colonization of any site. (T6-7-8)
However the correlation found in the first place (detected when using Spearman -Brown prediction formula) between lesional skin cultures and duration of AD can be explained as a relation between AD duration and the rate of lesional skin colonization but not the density. (T5).




Figures:


Pictures of Participants in the Study:



Patients with AD show high rates and densities of lesional skin and nasal colonization with staphylococcus aureus and increased densities correlated to AD severity, which justifies the therapeutic role of topical and systemic antibiotics in treating atopic dermatitis exacerbations especially when sever or accompanied with infections, and explains the importance of both prophylactic nasal antibiotic ointments in dealing with recurrent AD exacerbations as well as systemic antibiotics before invasive medical interventions.
AD patients had significant higher rates and densities of nasal colonization compared to non-atopic individuals, but no significant differences were noted when comparing skin colonization between the same two groups.
Financial barriers held us from repeating cultures to monitor the change in the load of SA during treatment, and determining the isolated SA subtypes and susceptibility to antibiotics.
In the light of our results, we recommend the following:
1- Regular use of skin emollients, and avoidance of irritating the skin in order to enhance the role of the skin barrier as a defender against allergens and bacteria.
2- Systemic antibiotics should be exclusively used to treat infection- complicated AD conditions.
3- Applying prophylactic antibiotics for AD patients before invasive procedures.
4- Prophylactic nasal antibiotic ointments could be beneficial in recurrent refractory cases of AD inorder to reduce the rates of exacerbations.
5-Raising awareness among parents of AD children about the importance of proper treatment of anyinfectionin order to avoid its bad influence on AD severity.
AD :Atopic Dermatitis – SA:Staphylococcus Aureus – SCORAD: Scoring Atopic Dermatitis – CFU: Colony Forming Units – FLG: Filaggrin – SC: Stratum Corneum –AMP: AntiMicrobial Peptide - TSLP:Thymic Stromal Lymphopoietin - TLR:Toll Like Receptor – DCD: Dermcidin.
We would like to acknowledge the participation of DR. Monzer Bobo in the statistical analysis of our results.
Conflicts of interest:
disclose no conflicts of interest with work involved in this article.
Funding:
No funding was received for the work involved in this article.
Ethical Approval:
Not applicable as this article does not involve direct human subject involvement.
No approval was required.
Consent:
Patients' consent was obtained for the publication of this case report.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.
















































