AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2834-5142/002
1 Department of Urology, K. S.Hegde Medical Academy, Deralakatte, Mangalore.
2 Department of General Surgery, K.S.Hedge Medical Academy, Deralakatte, Mangalore.
*Corresponding Author: Amulya Cherukumudi, Department of General Surgery, K.S.Hedge Medical Academy, Deralakatte, Mangalore E-mail: amulyac1@yahoo.com
Citation: Suraj Hegde, Amulya Cherukumudi, Rajeev T P, Narendra Pai. (2019) Renal Medullary Fibroma- A Histopathological Surprise in a Patient With an Asymptomatic Abdominal Mass. J Nephrol and Uro Inter. 2(1); DOI: 10.31579/2834-5142/002
Copyright: Amulya Cherukumudi ©2019.This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 August 2019 | Accepted: 20 August 2019 | Published: 29 August 2019
Keywords: renal medullary fibroma, benign, renal mass
Renal medullary fibroma is a fairly common, but unusual benign mass lesion of the kidney. These are often small in size, and rarely produce symptoms; hence they frequently go unnoticed, diagnosed only during autopsy in most cases. Very rarely, they achieve large enough sizes to produce compressive symptoms or a clinically palpable mass. This tumour, however, poses a radiological dilemma, as it cannot be differentiated from malignant lesions of the renal parenchyma. Here we present a unique case of an asymptomatic, incidentally detected left renal mass, which was reported as renal medullary fibroma, a benign disease.
A 42 year old female presented to the gynaecologist for pain abdomen and increased bleeding during menstruation since 6 months. She has no history of pain during menstrual cycles, haematuria, and loss of weight or urinary symptoms. She has, in the past, undergone laparoscopic cholecystectomy 15 years back, which was seemingly uneventful. Patient has no known co-morbidites, and hasn’t undergone any other intervention in the past.
On examination, patient was found to be pale; however, she was not icteric and had no generalized lymphadenopathy. On per abdomen examination, patient had minimal tenderness in the left lumbar region, though there was no palpable mass or hepatosplenomegaly. Per vaginum and per rectal examination was also found to be unremarkable.
For the above mentioned complaints, patient underwent a sonological examination, which showed an incidental finding of a left renal mass, for which she was referred to us. To confirm the findings, CECT abdomen and pelvis was done, which showed a 6.9 x 5.6 x 5.4 cm heterogeneously enhancing mass lesion involving the mid and lower pole of the left kidney (Figure1 and Figure 2).


As there was no evidence of lymphadenopathy or renal vein involvement on the CECT, a radiological diagnosis of renal malignancy was made, with a staging of T1BN0M0.
With the above mentioned findings, patient was worked up for surgery i.e left partial nephrectomy.
Patient was planned for open partial nephrectomy through a subcostal transperitoneal approach. On dissection of the lower pole, dense adhesions were noted to the mesentery of the left descending colon. A mid and lower pole mass lesion was noted in the left kidney, measuring approximately 7 x 6 cm. Due to the clinical suspicion of advanced malignant lesion, we proceeded with a left radical nephrectomy. Post-operative period was uneventful, and patient was discharged on POD 4.
There was, however, a histopathological surprise in waiting with the pathologist as the mass showed features suggestive benign medullary fibroma (Figure 3).

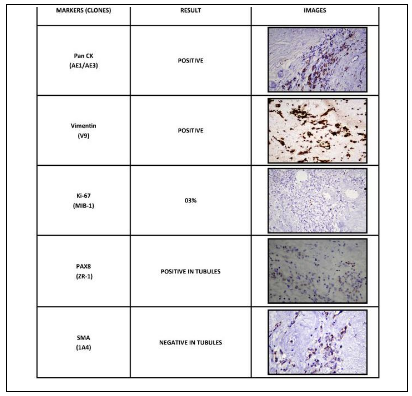
To confirm the diagnosis, immunohistochemistry markers were applied to the specimen, which was confirmatory for benign medullary fibroma (image 4 and 5). The histopathology specimen showed positivity for
It was decided that patient doesn’t require any further chemotherapy or radiotherapy as it was a benign mass. Patient has since been on follow-up, and remains asymptomatic.

Renal medullary fibroma is a common tumour found in the kidney, present in 26% of consecutive autopsy specimens. As they do not achieve large sizes, they are often missed and remain asymptomatic during the life of the patient. It is a radiological challenge as well, as it cannot be accurately differentiated from renal malignancies. Hence, this is usually identified as a histological surprise following partial or radical nephrectomy. They are not encapsulated but well-defined nodules that are usually solitary, but can be multiple and bilateral at times. Prevalence increases with age and the distribution of sex is equal. Over 50% of patients are over the age of 20 years. Few renal medullary fibromas are sufficiently large to become clinically apparent and cause tumor torsion symptoms, such as haematuria due to venous stasis and infarction (1). Pre-operative diagnosis especially via radiological assessment, in the form of calcifications on X-rays, echogenicity on CECT abdomen and pelvis and arteriogram to confirm vascularity, mimics renal cell carcinoma. Evaluation of renal medullary fibroma by magnetic resonance imaging (MRI) may be helpful. On MRI, renal medullary fibroma presumably shows low signal intensity in T1 and T2-weighted images due to its dense collagen content and low cellularity.
There are several differential diagnoses, especially other calcified lesions of the renal parenchyma. These include osteosarcoma of the kidney, Xanthogranulomatous pyelonephritis secondary to Staghorn calculus, renal leiomyoma, haematoma (increased haemosiderin), inflammatory pseudotumour and malignant fibroma of renal parenchyma etc (2, 3).
Usually these patients undergo radical nephrectomy as it is not possible to rule out malignancy with certainty. These entities are completely benign, however, and patients have an excellent prognosis and, if this lesion is radiologically suspected, there may be a role for biopsy. There is still no clear definition of the role of positron emission tomography (PET) scan in renal masses. Benign tumours are usually photopenic on PET scan; malignant tumours have avidity for fluorodeoxyglucose, with few exceptions (4). These clinical scenarios can be evaluated by MRI and PET scans to prevent unnecessary removal of normal renal parenchymal tissue. In these cases, prudent use of the available imaging methods can help us decide to perform nephron-sparing surgery. Radiologists and clinicians need to be aware of the potential for further evaluation of these kinds of lesions.
Conclusion
Renal medullary fibroma is a rare but benign tumour of the kidney that is often mistaken for renal cell carcinoma. If there is a clinical suspicion of this condition, we can avoid radical surgical procedures for the patient.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.
















































