AUCTORES
Globalize your Research

case report
*Corresponding Author: Yi Zhang, MD, PhD, Department of Cardiothoracic Vascular Surgery, The Affiliated Hospital of Youjiang Medical University for Nationalities, Baise, China.
Citation: Fengqing Liao, Jialong Huang, BoHao Yang, Yang Hu, XiaFei Li, et al, (2024), Tracheal Reconstruction in a Patient with Tracheal Stenosis Following Acute Pancreatitis Supported by VV ECMO: a Case Report and Literature Review, International Journal of Clinical Case Reports and Reviews, 18(3); DOI:10.31579/2690-4861/438
Copyright: © 2024, Yi Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 April 2024 | Accepted: 25 June 2024 | Published: 08 July 2024
Keywords: tracheal stenosis; acute pancreatitis; ecmo; tracheotomy; airway management
This case report presents a case of tracheal obstruction following severe pancreatitis and describes the condition and airway management of an adult patient from the emergency department to the intensive care unit (ICU), from airway management to pre-operative ECMO implantation to intraoperative ECMO Weaning. Transselective venovenous extracorporeal membrane oxygenation (VV ECMO) effectively mitigates the risks associated with tracheotomy, thereby creating a safe setting for tracheal reconstruction surgery. This case report delves into the mechanisms, characteristics, diagnosis, and treatment of tracheal stenosis. Additionally, a potential association between tracheal stenosis and pancreatitis is explored. Tracheotomy supported by VV ECMO to ensure ventilation, emerges as a viable alternative.
AP is an acute inflammatory condition characterized by the self-digestion of pancreatic tissue, leading to a systemic inflammatory response.1-3 TS is an obstructive upper airway disease that can be life-threatening.4 Severe cases of TS are rare and typically present as respiratory dysfunction.5 Currently, the main cause of TS is believed to be the result of repeated injury and repair of the tracheal mucosa and abnormal wound healing such as granulation tissue proliferation.4,6 ECMO is mainly used to provide continuous extracorporeal respiratory and circulatory support to maintain life in patients with respiratory and/or cardiovascular failure, and is usually used in patients with severe acute respiratory distress syndrome (ARDS).7,8
In this article, we present a case study of a patient who developed severe tracheal stenosis two months after surgery for severe pancreatitis. The patient underwent a successful tracheal reconstruction with ECMO support. It is important to note that tracheal stenosis following pancreatitis is an extremely rare occurrence. Our focus was on exploring the relationship between tracheal stenosis and pancreatitis, discussing the selection of surgical methods, managing the patient’s airway, and highlighting the application of ECMO.
A 31-year-old male was admitted to our hospital's emergency department in May 2023 with dyspnea and confusion. The patient’s family complained of shortness of breath for 7 days after activities, which was significantly aggravated in the past 3 days, accompanied by a cough and difficulty in coughing up phlegm. Upon admission, physical examination revealed the presence of three obvious concave signs, profuse sweating throughout the body, and wheezing rales in both lungs. Additionally, a 10 cm surgical scar and peri-pancreatic drainage tube were observed in the left abdominal region. On arrival, his oxygen saturation in room air, was 90%, and his heart rate (HR) was 121 bpm. The initial blood pressure (BP) readings were 226/113 mmHg. Immediate management of the patient included high-flow non-invasive oxygen therapy and urapidil infusion, which resulted in immediate improvement in breathing, an increase in SpO2 to 100%, and a decrease in blood pressure to 182/99 mmHg.
The patient was admitted to our hospital at the end of January 2023 with acute pancreatitis, complicated by pulmonary infection and respiratory failure. Following pancreatic puncture drainage, anti-infection treatment, blood transfusions, and six days of tracheal intubation, the patient’s condition improved. However, the fever recurred later, and the condition gradually deteriorated. In early March, surgical intervention was performed to remove necrotic pancreatic tissue and drain the peri-pancreatic abscess. On the second postoperative day, the patient developed acute peritonitis, sepsis, and multiple organ failure. Laparoscopic exploration, removal of pancreatic necrotic tissue, abscess incision and drainage, and jejunostomy surgery are all performed in an emergency. After six days of mechanical ventilation via tracheal intubation, the patient was successfully weaned and showed gradual improvement. He was discharged in mid-April but still had a peripancreatic drainage tube in place. The patient was in good health prior to admission.
Immediate chest CT and three-dimensional reconstruction of the trachea revealed significant tracheal stenosis (below the cricoid cartilage), with no apparent abnormalities in the rest of the trachea(Figure2 a). Abdominal CT showed resolution of exudative lesions in the abdominal cavity, decreased ascites, and improvement in mesenteric edema. The patient was transferred to the ICU because of confusion consciousness gradually improved, and oxygen saturation increased following sputum aspiration, high-flow noninvasive mechanical ventilation, and oxygen therapy.
A multidisciplinary team comprising critical care physicians, respiratory physicians, cardiothoracic surgeons, anesthesia teams, and ENT surgeons, consulted at the bedside in the ICU, with special focus on airway management. Given the patient’s short neck, severe stenosis below the cricoid cartilage, and the potential inability of our smallest tracheal tube to pass through the narrowed lumen, our primary concern was the risk of rapid respiratory failure in the event of failed intubation leading to airway bleeding. Tracheotomy, although initially considered, was deemed excessively risky because of its high potential for bleeding and asphyxia. Bronchoscopic balloon dilatation was also considered but was deemed highly likely to fail because of the severity of the stenosis, potentially causing treatment delays. Therefore we needed a new method to ensure adequate ventilation. Hence, we reached out internal ECMO team and proposed an individualized approach after extensive deliberation. This approach involved a predetermined VV ECMO cycle under local anesthesia, followed by transfer to the operating room for the induction of general anesthesia with ECMO support. The patient then underwent the classical procedure of tracheal resection and end-to-end anastomosis, and specimens were collected for pathological evaluation. After the procedure, the patient received further treatment in the ICU. The patient’s family provided informed consent for the proposed plan, acknowledging its associated risks and benefits.
After administering sedation, the patient was positioned supine with the head tilted to the left side and the right lower limb abducted and externally rotated. The right internal jugular vein and right femoral vein were used as catheters. Following local anesthesia with 2% lidocaine, ECMO catheters were placed under ultrasound guidance and heparin saline was injected. The flow rate was gradually adjusted from 0.5 L/min. When the flow rate reached 3.45 L/min, ECMO functioned effectively, achieving a blood oxygen saturation of 100%, and the catheter was secured in place.
An unexpected occurred upon admission to the operating room. Blood oxygen saturation decreased from 100 percent to 78 percent, while vital signs remained stable. Suspecting inadequate blood volume or recirculation as potential causes, 2.0 u of suspended red blood cells without white blood cells and 1,000 ml of sodium lactate Ringer solution were given to replenish the blood volume. Additionally, we adjusted the blood flow rate to 3.6 L/min, resulting in a gradual increase in the blood oxygen saturation to 96 percent. With the patient’s blood oxygen restored, the procedure commenced with the patient in the supine position. Tracheotomy was performed under local anesthesia, followed by intubation and mechanical ventilation to maintain a blood oxygen saturation above 95 percent. Minor intraoperative bleeding was also observed. The patient was weaned from ECMO as soon as possible to prevent ECMO-related complications and alleviate the financial burden on the patient’s family. The ECMO blood flow rate was reduced to 1.5 L/min, then turned off completely, while the patient’s oxygen saturation remained stable at 98 percent. After a total operative time of 1.5 hours, successful weaning from ECMO was achieved. Following satisfactory general anesthesia, a vertical incision of approximately 6 cm in length was made in the neck, up to the thyroid cartilage down to the suprasternal fossa, and the trachea was incised upwards along the endotracheal tube. The thickened tracheal wall was approximately 2 cm in long. The stenotic trachea was resected and the posterior and lateral walls of the trachea were anastomosed with a 3-0PDS suture. Adequate hemostasis was achieved and the incision was thoroughly irrigated before layer-by-layer closure. The lower jaw was fixed with a No.10 suture and the neck was positioned in a forward flexed position. Intraoperative bleeding was minimal and blood oxygen saturation remained above 95 percent throughout the procedure.
Following the surgical procedure, the patient was admitted to the ICU for ongoing treatment while still intubated. The following day, the patient regained full consciousness and was able to breathe spontaneously without any shortness of breath, asthma, or surgical complications(Figure2 b). Subsequent examination using an electronic bronchoscope revealed that the patient’s airway was unobstructed, and no significant narrowing was observed. Following extubation, the patient did not experience any discomfort such as difficulty in breathing.
When the patient's condition stabilized, he was transferred to the general respiratory ward for further treatment and evaluation of his pancreatic disease. Currently, the patient’s pancreatic abscess has been completely drained, and a re-examination has shown significant improvement. The peripancreatic drainage tube was removed based on the recommendations of hepatobiliary surgeons. Subsequent treatment proceeded smoothly. Histopathological examination of the resected specimen showed chronic mucosal inflammation with squamous metaplasia, obvious fibrous connective tissue hyperplasia, and several trabecular bone formations on the lateral side of the cricoid cartilage, however no tumors were found(Figure1).
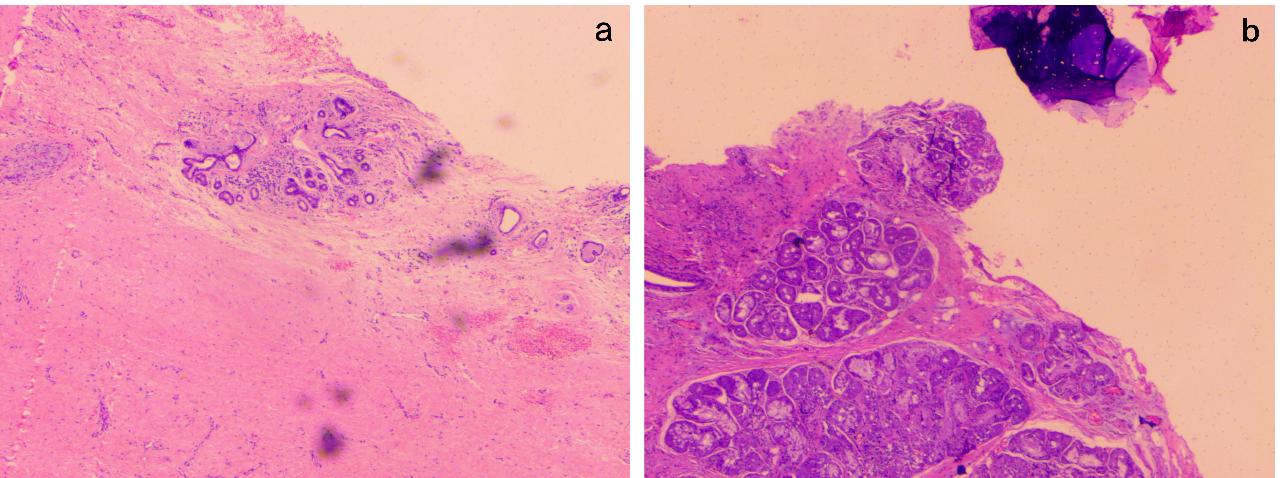
Figure 1. Pathological examination showed chronic mucosal inflammation with squamous metaplasia, obvious fibrous connective tissue hyperplasia, and several trabecular bone formations on the lateral side of the cricoid cartilage, but no tumor was found.
During a follow-up examination conducted 5 months after the surgery, no new narrowing of the airway was detected, and there was a significant improvement in tracheal stenosis compared to the preoperative condition (Figure2 c).
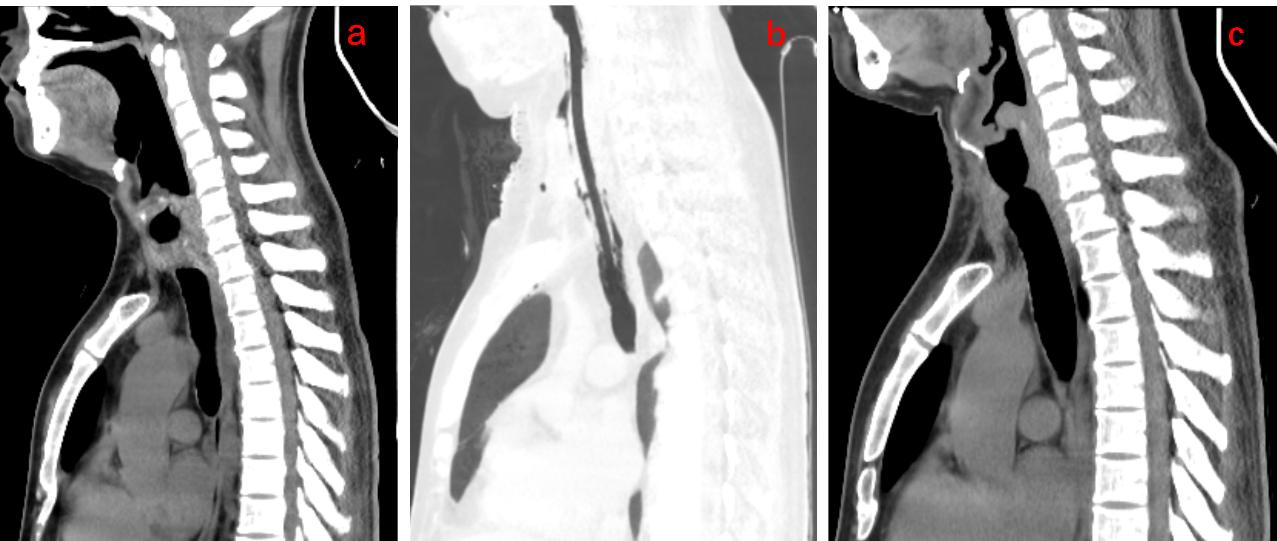
Figure 2. (a)A CT examination on admission revealed significant narrowing of the trachea (below cricoid cartilage level). (b)A post-operative CT examination revealed that the trachea was intubated, the extent of tracheal stenosis was reduced compared to before, and there was new edema and drainage tube shadowing in the soft tissue of the anterior neck. (c)A CT examination 5 months after surgery showed that the trachea (level below the cricoid cartilage) was slightly narrow, which was significantly better than before surgery, and the edema of the anterior cervical soft tissue subsided
Discussion
This case report describes a patient who developed severe tracheal stenosis two months after undergoing tracheal intubation, mechanical ventilation, and surgical treatment for severe acute pancreatitis. The occurrence of severe tracheal stenosis during the subsequent treatment of acute pancreatitis raises questions about the potential connection between the two conditions. AP is an acute inflammatory process characterized by the self-digestion of pancreatic tissue.1-3 The primary systemic complications include systemic inflammatory response syndrome (SIRS), sepsis, multiple organ dysfunction syndrome (MODS), intra-abdominal hypertension (IAH), and abdominal compartment syndrome (ACS). Local complications were mainly related to fluid accumulation in the pancreas peri-pancreas and tissue necrosis. Other complications include gastrointestinal bleeding, abdominal bleeding, biliary obstruction, intestinal obstruction, and intestinal fistula, etc.1,3,9 TS is an obstructive upper airway disease that typically results from repeated damage and repair of the tracheal mucosa and proliferation of granulation tissue.4,6 Various causes can lead to TS, including tracheotomy, tracheal intubation, tracheal trauma or surgery, inhalation injury, infectious causes, and immune-related factors (such as granulomatosis with polyangiitis, systemic lupus erythematosus, relapsing polychondritis, sarcoidosis, and IgG4-related disease). Prolonged mechanical ventilation with endotracheal intubation is the most common cause of TS.4,6,10,11 Major risk factors include diabetes mellitus, prolonged intubation, the use of large types of catheters, recurrent respiratory tract infections, advanced age, gastroesophageal reflux, steroid treatment, etc.11-13 The patient reported in this case had complications involving multiple systems of the body, including the respiratory system. Although he had undergone tracheal intubation, the development of such severe stenosis following intubation was extremely rare. We considered the possibility that pancreatitis could contribute to or worsen the tracheal stenosis. In a literature review, we came across a case report by Yasuo describing a patient with tracheal stenosis due to autoimmune pancreatitis. Bronchial biopsy revealed diffuse infiltration of plasma cells, lymphocytes, and fibrotic eosinophils. Immunostaining revealed infiltration of several IgG4-positive plasma cells, ruling out the possibility of coexisting sarcoidosis and the significant impact of steroid therapy.14 This finding suggests a possible direct relationship between autoimmune pancreatitis and tracheal stenosis. The repair process of tracheal injury is a highly coordinated wound healing process, and comorbidity and critical illness can disrupt its balance and lead to abnormal scar formation. Currently, there is no evidence of direct relationship between acute pancreatitis and tracheal stenosis. However, the systemic inflammatory response triggered by pancreatitis, along with the resulting multi-organ damage including the respiratory system, and the increased blood glucose levels due to impaired islet function, may indirectly contribute to the occurrence and worsening of tracheal stenosis. This case suggests a potential connection between pancreatitis and tracheal stenosis that warrants further confirmation.
The primary symptoms of TS include varying degrees of dyspnea and shortness of breath, accompanied by cough, wheezing, and increased respiratory secretions, which are exacerbated by physical activity.5,15 The patient was admitted to the hospital because of shortness of breath, and a CT examination revealed severe tracheal stenosis. The treatment for TS varies depending on the etiology, location, and severity of the stenosis, with surgery being the main approach. Surgical techniques included airway stenting, balloon dilatation, and tracheal resection. Endoscopic balloon dilation is the main treatment method known for its simplicity, effectiveness, and short procedure duration.16 However, it is typically used in patients with mild stenosis (stage 1 or 2), in early immature lesions or soon after an airway reconstruction procedure to prevent restenosis.17,18 In this particular case, considering the patient’s severe tracheal stenosis, endoscopic balloon dilation was not suitable. Tracheal resection and end-to-end anastomosis (TRE) are the standard treatments for tracheal stenosis, known for their lower restenosis rates compared to endoscopic treatment.17-20 After evaluation, we concluded that TRE was the most appropriate surgical approach.
Hypoxemia and asphyxia are the primary causes of mortality in these patients.15 The key to treatment is ensuring adequate oxygenation, ventilation, and emergency surgical intervention.15,21 Surgical resection of tracheal stenosis cannot be safely performed without adequate ventilation. Conventional airway management techniques, such as nasal oxygenation, mask ventilation, supraglottic airway devices, laryngeal masks, endotracheal intubation, and tracheotomy, are typically suitable for patients with mild airway obstruction.15,22 However, due to the patient’s near-complete tracheal stenosis below the cricoid cartilage, tracheal intubation and tracheotomy carry a significant risk of hemorrhage and asphyxia. Anesthesia induction could result in complete occlusion of the airway, and the application of the appeal method may not guarantee adequate ventilation. In such cases, extracorporeal ECMO may be a suitable option.
ECMO is mainly used to provide continuous extracorporeal respiratory and circulatory support to maintain life in patients with respiratory and/or cardiovascular failure, commonly seen in severe ARDS.7,8 The two main ECMO modes are veno-arterial (VA) ECMO and veno-venous (VV) ECMO. In VA ECMO, venous blood is withdrawn, oxygenated, and returned to the arterial system to provide circulatory and respiratory support, which is a heart-lung replacement mode.8,21,22 Compared to the VA mode, VV ECMO solely offers extracorporeal respiratory support, avoiding the risk of arterial injury and causing fewer hemodynamic disturbances.21,23 The choice of ECMO mainly depends on the urgency and necessity of circulatory support.23 In this case, considering the patient’s intact circulatory function, we opted for VV ECMO. Following the initiation of ECMO, the patient’s oxygen saturation was 100%. However, it dropped upon arrival at the operating room. We suspected recirculation or insufficient blood volume as possible causes, and observed that the oxygen saturation returned to normal after blood transfusion, fluid resuscitation, and flow adjustment. We performed tracheotomy with ECMO support, which resulted in the stabilization of blood oxygen levels following intubation. Considering the potential complications associated with long-term ECMO use (and long-term intubation), such as renal failure requiring continuous hemofiltration, bacterial pneumonia, bleeding, sepsis, hemolysis, liver dysfunction, leg ischemia, and venous thrombosis, we aimed to wean the patient off ECMO as soon as feasible.21 The incidence of complications with ECMO for short periods is relatively low, and early weaning can reduce the likelihood of complications and minimize hospitalization costs.21 The utilization of ECMO in the treatment of tracheal stenosis offers notable advantages. First, it can be employed in cases of severe tracheal stenosis where oxygenation through the trachea is not possible, providing valuable time for strategy formulation and implementing appropriate treatment measures.7,24 Second, it allows for satisfactory oxygenation during tracheotomy, circumventing the risk of bleeding and asphyxia. When conventional ventilation methods are difficult to complete or there are serious risks of uncontrollability, tracheotomy supported by ECMO may represent a reasonable and effective approach.
In summary, we present a case of severe tracheal stenosis following pancreatitis in which acute pancreatitis may indirectly lead to the occurrence and exacerbation of tracheal stenosis. In complex ventilation scenarios, ECMO can guarantee adequate oxygenation, allowing time for appropriate treatment. During the surgery, we performed tracheotomy with ECMO support to ensure proper ventilation. It has been shown that this may be a reasonable approach. In the development of cardiothoracic surgery, surgical risks have been controlled through multidisciplinary collaboration and technological advances, enabling increasingly sophisticated cardiothoracic surgery to be performed safely.25 This case report serves as an example of this evolving trend, which will continue in the future.
We express our gratitude to the patient who kindly provided consent for this case to be presented in this report.
Abbreviation: AP,Acute pancreatitis; TS, Tracheal stenosis; ICU, intensive care unit; ECMO, Extracorporeal membrane oxygenation; VV ECMO, venovenous extracorporeal membrane oxygenation; ARDS, acute respiratory distress syndrome; HR, heart rate; BP, blood pressure; SIRS, systemic inflammatory response syndrome; MODS, multiple organ dysfunction syndrome; IAH, intra-abdominal hypertension; ACS, abdominal compartment syndrome; TRE, Tracheal resection and end-to-end anastomosis ; VA, veno-arterial
Conceptualization:BoHao Yang.
Supervision: Jialong Huang, Yang Hu, Zhichao Ni.
Validation: Fengqing Liao, XiaFei Li, Xi Xia.
Visualization: Yi Zhang.
Writing – original draft: BoHao Yang, Yi Zhang.
Writing – review & editing: Jialong Huang, Fengqing Liao.
Funding Statement:The article didn't receive any forms of financial support.
The Author(s) declare(s) that there is no conflict of interest.
Supporting data can be requested by emailing the corresponding author for reasonable claims.
Ethics approval and consent to participate
Verbal informed consent was obtained from the patient's family for participation.
Verbal informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
