AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Sebastian Reindl, Department for Cardiothoracic Surgery, University Hospital Augsburg, Germany.
Citation: Reindl S., Jawny P.,Girdauskas E., Raab S. (2022). Thoracic trauma with suspected cardiac injury on admission: how often is a cardiothoracic surgeon required, J. Thoracic Disease and Cardiothoracic Surgery, 3(2) DOI: 10.31579/2693-2156/041
Copyright: © 2022 Sebastian Reindl. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 July 2022 | Accepted: 12 July 2022 | Published: 19 August 2022
Keywords: chest wall; blunt thoracic trauma; penetrating thoracic trauma; cardiac injury; ventricular injury; hemopericardium
Introduction: Cardiac involvement in the setting of thoracic trauma is possible with both blunt and penetrating mechanisms. Overall, structural cardiac injury is rare, but when it occurs, it requires immediate diagnosis. We evaluated our process in decision-taking and further surgical procedures if necessary. The aim of this retrospective study is (1) the analysis of cardiac injury patterns and their therapeutic approaches, (2) in how many of these cases a cardiothoracic surgeon is needed in trauma room care and (3) in how many patients cardiothoracic surgery was indicated.
Patients and Methods: We analyzed all blunt and penetrating trauma patients with suspected cardiac injury at the time of admission between 7/2016 and 7/2021. Sonography, cardiac enzymes, and electrocardiography were obtained obligatorily. Computed tomography (CT) was carried out in hemodynamically stable patients. Trauma room protocols were analyzed including available Injury Severy Scores (ISS). Data on cardiac injuries, operations, access routes, outcomes and hospitalization were evaluated.
Results: In total, 43 patients with cardiac injury at the time of admission could be identified. Contusio cordis was detected in 27 patients (63%), in whom conservative therapy was performed. We indicated surgical intervention in 16 patients (37.2%): nine patients (21%) after blunt chest trauma with cardiac or pericardial injuries, mean ISS 37.3 (9.7). These included tricuspid regurgitation after traumatic rupture of chordae tendineae and rupture of the left atrial appendage. Seven patients (16%) underwent surgery for penetrating chest trauma: six for cardiac knife injury, one patient for iatrogenic drainage dislocation in the left ventricle. Mortality was 22% in surgically treated blunt trauma patients, whereas no mortality was observed in penetrating trauma.
Discussion: The most common cardiac injury after blunt thoracic trauma is contusio cordis. In these patients’ surgical treatment is usually not necessary. In contrast, thoracic trauma with structural cardiac injury needs a coordinated and interdisciplinary management in a center with cardiothoracic surgery. In addition to anamnesis and clinical examination, sonography with echocardiography and CT in particular play a decisive role in a rapid diagnosis. In the patients presented in this study, more than every third case required cardiothoracic surgery (16 out of 43 patients, 37.2%). Thus, cardiothoracic expertise should be present for all trauma room patients with suspected cardiac injury.
In trauma room care, the trauma leader – usually a trauma surgeon – decides on necessary specialists for the respective patient and injury patterns. Thoracic trauma plays a key role in the care of severely injured patients (Abbreviated Injury Scale, AIS, injury severity ≥ 2). In the distribution of injuries according to the AIS, thoracic injuries hold a share of 45% in all patients [1]. Blunt (most often traffic accidents or falls from different heights) in comparison to penetrating trauma mechanisms play a major role in terms of numbers (96.3% vs. 3.7%) [2–4]. Currently available figures from the TraumaRegister DGU® (German Trauma Society) put heart injuries at about 1.8% of blunt and about 2.6% of penetrating trauma [5]. The proportion of cardiac contusion is up to 76% in the context of blunt trauma mechanisms, with arrhythmias and disorders of the conduction system as typical findings [6]. Clinically, cardiac trauma manifests asymptomatically to highly acute with signs of infarction due to coronary involvement [7]. Due to the immediate retrosternal location, the right heart is affected more often. In case of highly acute symptoms and hemodynamic instability, ECLS (extracorporeal life support) is also a treatment option [8–10].
The initial diagnostics in the trauma room is of vital importance in cardiac trauma. Sonography (eFAST) and computed tomography (CT-thorax, angio-CT of the thorax or trauma room spiral) are integrated in the ATLS algorithm and allow a fast and reliable diagnosis of cardiac and / or pericardial injuries [11,12]. The establishment of a pleural drainage is of major importance and in many cases already represents the definitive care in preclinical and clinical settings [5,6]. By this, an emergency thoracotomy can be quickly decided for or against. [13,14]. The diagnostic standards also include the measurement of cardiac enzymes, whereby in terms of sensitivity cardiac troponin I or T has largely replaced creatine kinase (CK) or myocardial proportion (CK-MB) [15]. The 12-lead electrocardiography (ECG) can rule out cardiac involvement at an early stage or indicate myocardial damage. Both parameters are suitable for follow-up in the case of cardiac.
Consequently, an interdisciplinary therapeutic approach is of significant importance. If there is a suspicion of cardiac involvement, it is advisable to consult a cardiothoracic surgeon at an early stage. In this context, an interdisciplinary decision on acute life-threatening injuries to be treated primarily is indispensable. Thus, cardiac injuries in the triage of injury patterns are sometimes not to be treated immediately, but in the timely course of polytrauma care. However, there are currently no comprehensive guidelines for cardiac injury patterns.
In order to elucidate how decision-taking for further diagnostics and therapy takes place in a level one trauma center, we selected patients in whom a cardiac injury was either obvious or very probable, e. g. penetrating injury in the cardiac box. In addition, patients were selected after a blunt thoracic trauma for whom cardiac injury had already been mentioned as the admission diagnosis. Therefore, the aim of this study is
Patient selection
For the present study, all patients with blunt or penetrating chest trauma in the period 07/2016 to 07/2021 at the University Hospital Augsburg were retrospectively analyzed. We identified a group of patients with cardiac injury as the leading diagnosis either in the prehospital or in the trauma room setting. Cardiac injuries as a secondary diagnosis and traumatic aortic injuries were not considered.
Trauma Room Management
Procedure and diagnostics for trauma room patients were carried out according to a standardized protocol. First, there was a structured handover from the emergency physician to the trauma leader. He has also determined beforehand which surgical expertise, i. e. a cardiacthoracic surgeon, had to be present. The patient was then taken to the trauma room. Accordingly, a decision is made whether immediate surgical intervention such as emergency thoracotomy was necessary, or whether the patient's cardiovascular system was stable enough for further diagnostics. These included physical examination, sonography of the abdominal and intrathoracic organs according to the eFAST algorithm and blood sampling including troponin I and ECG. Here again the decision is made whether surgical intervention such as pleural drainage or thoracotomy is necessary, or whether a CT scan is performed. With the knowledge of these findings, the decision on the further procedure was then made. Subsequently, it was analyzed which surgical therapy was carried out in which urgency and time interval after hospital admission.
Statistical Analysis
For the patients identified, trauma room protocols were analyzed including available Injury Severy Scores (ISS). Data on cardiac injuries, operations, access routes, outcomes and hospitalization were collected and evaluated. Statistical calculations were performed using IBM SPSS Statistics, release 28 (IBM Inc, Armonk, New York, USA). For qualitative data, absolute and relative frequencies were calculated. Quantitative results are presented by mean (standard deviation) (range). To compare two groups, student’s t-test was used. Because of the rather small sample sizes, exact tests were performed. The result of a statistical test was considered statistically significant if the p value was less than 0.05.
Patient Characteristics
A total of 44 patients with cardiac injuries at the time of admission were identified. One patient with suspicion on hemopericardium, in which a serous pericardial effusion was shown intraoperatively, was excluded. The 43 patients were 28 men (65.1%) and 15 women (34.9%). The mean age at admission was 45.5 (30.0) years. Within our patient collective, blunt thoracic trauma was significantly more common than penetrating: 36 vs. 7 (83.7 vs. 16.3%).
In total, we indicated surgery in 16 patients (37.2%): nine procedures for blunt trauma, seven procedures for penetrating trauma. A significant age difference was not found in patients with indication for surgery: 49.9 (18.9) vs. 44.4 (24.1) years (p = 0.585).
The detailed characteristics of patients with cardiac injuries after blunt and penetrating thoracic trauma are listed in table 1.
Blunt Cardiac Injuries
As the most common cardiac injury cardiac contusion (contusio cordis) could be identified in 27 cases (75.0% of blunt traumas). These patients were treated conservatively regarding the cardiac involvement but were closely monitored on intensive care units. For this purpose, laboratory controls of troponin I as well as echocardiographic follow-up checks were carried out to assess regional wall movement disorders, a persistent or progressive reduction of the ejection fraction as well as pericardial effusion. ECG controls were also used to detect indications of newly occurring ischemia at an early stage. These patients did not require interventional or surgical therapy. The average length of stay was 10.0 (11.3) days. Among this group, an 85-year-old patient (i. e. 3,7% of patients with cardiac contusion) died on the day of her admission due to severe thoracic trauma with higher-grade dislocated rib fractures C1 to C9, undislocated sternal fracture and progressive bradycardia due to cardiac contusion.
We indicated surgical treatment of a cardiac injury in a total of n = 9 patients (25.0 % of blunt trauma) based on the following diagnoses:
The average Injury Severity Score (ISS) calculated in this subgroup was 37.3 (9.7). Surgery took place 5.0 (5.1) days after the accident event. The surgical access was chosen according to the injury pattern present: median sternotomy (n = 1), anterolateral thoracotomy (n = 7), video-assisted thoracoscopy VATS (n = 1).
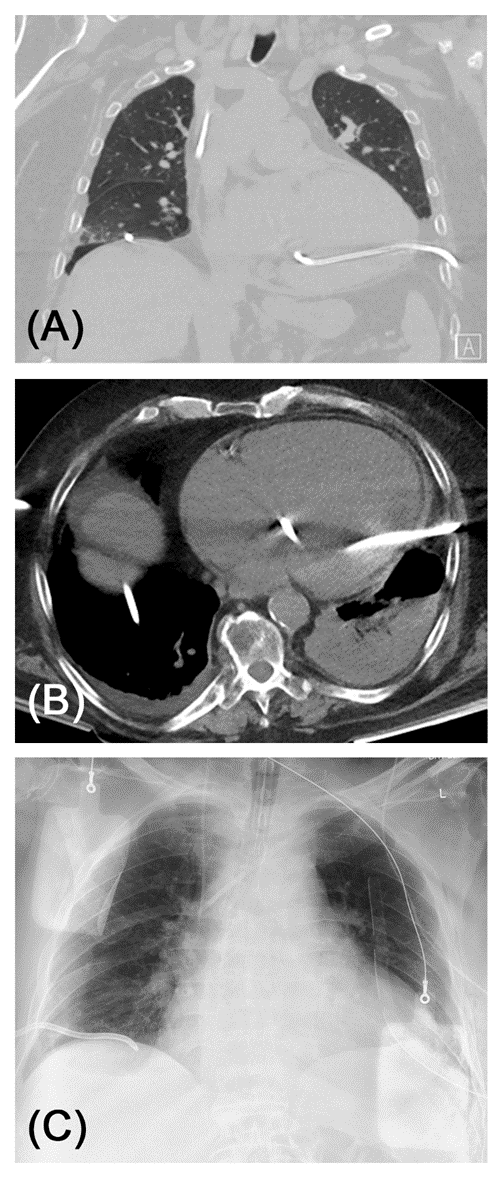
Severe pericardial rupture with luxatio cordis had been confirmed in two patients. Due to the serious injuries, thoracic surgery in both patients could only be performed after 8 and 12 days following the accident (deceleration trauma due to traffic accidents in both patients). Via anterolateral thoracotomy, the rupture was reconstructed by pericardial mesh plasty, and concomitant intra-thoracic injuries were treated (see figure 1).
A. Shown is a pre-operative chest X-ray. Heart and mediastinum are clearly shifted towards the left thoracic wall.
B. Postoperative chest X-ray after pericardial mesh plasty via anterolateral thoracotomy. Heart and mediastinum are centered.
C. Trauma room CT spiral. Ventral rupture of the anterior thoracic wall with affection of the adherent pericardium (arrow). The heart is shifted towards the left side. Massive lung contusion can be seen dorsal.
D. Intraoperative videoscopic photograph after pericardial mesh graft plasty.
Figure 1: Casuistry 1: 61-year-old male patient after car accident. Intubation at accident site. The chest tube was also inserted preclinically.

A. Spiral CT showed left sided rib fractures with dislocated endings affecting the pericardium.
B. Via contrast enhancement active bleeding of a pericardial vessel can be seen. Intraoperatively, arrosion of the A. pericardiophrenica with massive bleeding was diagnosed.
C. Postoperative chest X-ray after ligature of the vessel and osteosynthesis of corresponding dislocated rib fractures. Unstable vertebral injuries were treated within the same operating procedure. The patient remained paraplegic.
Figure 2: Casuistry 2: 45-year-old patient after motorbike accident. Patient presented with fracture-related arrosion of the A. pericardiophrenica and a fulminant intrathoracic hemorrhage. After relief of the hemothorax this could be treated by a vascular ligature with subsequent osteosynthesis of the intrapleural dislocated fracture endings of the ribs.

A. TEE shows a high-grade valve regurgitation, vena contracta 0,757 cm.
B. Postoperative chest X-ray after tricuspid valve repair.
Figure 3: Casuistry 3: 17-year-old male after fall accident. Transesophageal echocardiography revealed a clearly visible rupture of the septal papillary muscle of the tricuspid valve, which prolapsed into the right atrium and led to high-grade valve regurgitation. In addition, there was a traumatic subarachnoid hemorrhage, a subdural hematoma, and a rupture of the pelvic ring. Initially, neuro- and pelvic surgery was provided. After 13 days, the tricuspid valve was reconstructed via a median sternotomy in extracorporeal circulation by transmural refixation of the septal cusp and implantation of a 32 mm annuloplasty ring.
A. Pre-operative CT of the thorax (coronary reconstruction, lung window) clearly shows malpositioning of the tube inside the left ventricle.
B. The tip of the tube reaches the basal portion of the aortic valve apparatus. No aortic regurgitation was found in echocardiography.
C. Postoperative chest X-ray after removal of the tube via anterolateral thoracotomy and direct suture of the left-ventricular perforation. A new pleural drainage was inserted. External defibrillation paddles can be seen.
Figure 4: Casuistry 4: 87-year-old patient with cardiomyopathy and severely impaired left ventricular contractility. As part of cardiac decompensation, bilateral pleural effusions had developed. To relieve progressive dyspnea, a pleural drainage had been applied on both sides, left-sided it had come to a misalignment of the drainage via falsa into the left ventricle. The surgical therapy could be carried out here without a median sternotomy via anterolateral thoracotomy.
Both patients died after 14 and 18 days on intensive care therapy, respectively.
Apart from patients with luxatio cordis, there were no deaths, so that a mortality rate of 22.2 % is recorded in this group of patients. The average
intensive care treatment was 13.0 (5.6) days with a total hospitalization of 18.2 (6.2) days. One patient required long-term ventilation with tracheotomy (11.1%).
Penetrating Cardiac Injuries
Cardiac injury due to penetrating chest trauma was present in a total of n = 7 cases (i. e. 16.3% of all patients): exclusively male, age 44.4 (24.1), six thoracic knife stab injuries, one iatrogenic perforation of the left ventricle by mispositioning of a pleural drainage. No ISS was calculated for these patients. Except for the iatrogenic injury, the foreign bodies were no longer in situ. All patients received surgical care, six patients immediately after admission, one patient two days after the injury; mean 0.2 (0,7) days.
In five patients, an injury to the right ventricle was found intraoperatively. Ventricular suture was performed via anterolateral thoracotomy. Therefore, the pericardial lesion was expanded to a pericardial window and the hemopericardium was relieved. The cardiac injury then was sutured with monofilament, non-absorbable polypropylene threads (thickness 2-0 or 3-0) with a Teflon felt as an abutment. The course of the coronary arteries was strictly observed. Intrapericardial and intrapleural drainages were placed. A left ventricular injury was shown in one patient. In this case, median sternotomy was chosen as surgical access to treat the injury under optimal exposure. A coronary injury was not found in any patient.
There were no deaths in this group of patients. The average intensive care treatment was 5.0 (2.6) days with a total hospitalization of 6.4 (3.5) days. No patient required long-term ventilation or tracheotomy. Patients after suicide attempt remained in intensive care units for monitoring until they were transferred to a psychiatric follow-up.
Clinical Relevance of Cardiac Injuries in Blunt Thoracic Trauma
The focus of this study is on cardiac injuries, which were already mentioned as the main diagnosis during admission. Here we were interested in the extent to which they already require cardiosurgical expertise in the emergency room and how quickly they need to be treated. Most cardiac injuries in chest trauma are associated with compression and deceleration mechanisms. In these patients the most common cardiac injury is cardiac contusion. This is congruent with the data presented in this study: 75.0% of blunt trauma showed this type of cardiac injury. These patients usually do not require any further therapy and can be treated in centers without cardiothoracic surgery expertise [16]. They have a particularly good prognosis. The rarer group of patients with structural heart injuries (25% in our cohort) require completely different care. Because of the vital threat to patients, a chest trauma should always be evaluated to determine whether there is a structural heart injury [8,9].
Cardiologic expertise for arrhythmias and non-perforating coronary injuries is necessary. We did not diagnose these rare complications during our observation period. However, we have certainly observed perforation of the pericardium with and without dislocations. These were treated at a later stage (after 5.0 (5.1) days), since other injuries required more urgent therapy - provided hemodynamic stability was present. Pericardial injuries are the most common entity that led to surgical intervention in our study. Cardiac dislocation occurs rarely but is then associated with high mortality in view of the typically severe polytrauma (ISS 37.3 (9.7) in our cohort). The critical injuries in blunt trauma patients require significant longer intensive care and hospitalization in comparison to penetrating cardiac injuries: ICU stay in blunt trauma 13.0 (5.6) days vs. 5.0 (1.6) in penetrating trauma (p=0.026); hospital stay in blunt trauma 18.2 (6.2) days vs. 6.4 (3.4) in penetrating trauma (p=0.003) (see also table 1).
| blunt trauma | penetrating trauma | p | |
| m:f | 2:1 | 7:0 | |
| Age [years] | 49.9 (18.9) (17-74) | 44.4 (24.2) (19-87)) | 0.585 |
| accident | deceleration 6 fall 2 entrapment 1 | knife stab wound 6 iatrogenic LV perforation 1 | |
| ISS | 37.3 (9.7) | n.a. | n.a. |
| cardiac injury | luxation cordis 2 pericardial injury 4 arrosion of pericardiophrenic 1 tricuspid rupture 1 LAA rupture 1 | RV injury 5 LV injury 1 LV perforation 1 | |
access route thoracotomy median sternotomy VATS | 7 (77%) 1 (11%) 1 (11%) | 5 (71%) 1 (14%) 1 (14%) | |
| operation | pericardial plasty 2 pericardial drain 4 vessel ligature 1 LAA clip 1 tricuspid reconstruction 1 | RV suture 4 RV hemostasis 1 LV suture 2 | |
outcome survived TT deceased | 7 (77%) 1 (11%) 2 (22%) | 7 (100%) 0 (0%) 0 (0%) | |
| ICU stay [days] | 13.0 (5.6) (3-22) | 5,0 (2.6) (1-9) | 0.026 |
| hospital stay [days] | 18.2 (6.2) (12-29) | 6.4 (3.4) (1-11) | 0.003 |
| time to surgery [days] | 5.0 (5.1) (0-13) | 0.3 (0.7) (0-2) | 0.021 |
Tables: legend: f = female, m = male, VATS = video-assisted thoracoscopy, LAA = left atrial appendage, TT = tracheotomy, ICU = intensive care unit
Laceration on the pericardium is usually accompanied by hemorrhagic pericardial effusion, but tamponade does occur rarely in these cases, as relief in the pleural cavity is possible. A reconstruction of the pericardium with relief of the effusion by a pericardial and pleural drainage is the therapy of choice. Care was always taken how to position the patient and operations were carried out with the patient ready for immediate thoracotomy.
Structural injuries to the heart, such as ruptures of the myocardial wall or the valve apparatus, are clinically rare [17–19] whereby a relevant preclinical mortality is pointed out here. A partial amputation of the left atrial appendage could be treated without median sternotomy and use of extracorporeal circulation: a left atrial appendage (LAA) clip was used here, which is usually used for occlusion of the atrial appendage in rhythm surgery [20]. If necessary, the immediate preoperative –"prophylactic" – puncture of the inguinal vessels is also useful to establish a veno-arterial ECLS in acute deterioration of the vital parameters without loss of time. Injuries to the valve apparatus are rare and then require conventional surgical repair.
Clinical Relevance of Cardiac Injuries in Penetrating Thoracic Trauma
In our experience, penetrating cardiac injuries need often be surgically explored or treated. Penetrating injuries that only affect the anterior mediastinum are explicitly excluded here, as they can also be treated conservatively. Most often, our analysis found knife stab wounds, which more often affect the right ventricle due to the anatomical location behind the ventral chest wall. After relieving the pericardial effusion, a direct suture is usually possible via an anterolateral thoracotomy, whereby attention must be paid to the course of the coronary arteries. Iatrogenic perforations of cardiac structures are possible, but very rare.
In the patients shown in this study it was always possible to perform computed tomography to determine the exact location of the injury. This also meant that the access route was not always a median sternotomy, but also a lateral thoracotomy. A thoracoscopy should continue to be viewed critically here, since it was sufficient only once in the case of a laceration of the ventricle. A second time a conversion to thoracotomy was needed due to bleeding. With the involvement of the left ventricle, the median sternotomy provides the best exposure and at the same time allows the rapid commissioning of extracorporeal circulation if it is necessary for the treatment of myocardial injury.
A distinction must be made between trauma room thoracotomy as ultima ratio for critical trauma patients. It is associated with a very poor prognosis in both penetrating and blunt trauma (21,22). In the patients presented here, an emergency thoracotomy in the operating room was required several times, but never a trauma room thoracotomy.
In the patients presented in this study, more than every third case required cardiothoracic surgery (16 out of 43 patients, 37.2%). Thus, cardiothoracic expertise should be present for all trauma room patients with suspected cardiac injury. From this retrospective analysis, we derive the following recommendations for suspected structural cardiac injuries:
Like most publications on this topic, the present study includes retrospective data analysis and must be critically discussed from this point of view. However, randomized controlled trials are difficult to implement for understandable reasons. Retrospective data collection is based on a relevant selection bias in sense of high prehospital mortality of cardiac injuries, in particular due to pericardial ruptures with cardiac dislocation and cardiac or coronary ruptures with consecutively fulminant pericardial tamponade. The presented data thus include pre-selected patients who reach the hospital alive with the aforementioned injury patterns. In literature, mortality from penetrating injuries to the heart is up to 86 % and from vascular injuries of the thorax up to 92 % (15,23). In autopsy studies, the detection of cardiac involvement in fatal thoracic trauma is described up to 96 % [24].
Nevertheless, the patient data analyzed here reflect the spectrum of cardiac injuries associated with blunt and penetrating in a maximum care hospital. If the patient reaches the hospital primarily alive or can be stabilized in the trauma room, a high survival rate can be achieved by the cardiothoracic surgeon. In our case series, mortality for blunt injuries to the heart was 22% of the patients receiving surgical care, while no mortality was recorded for penetrating injuries.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Sebastian Reindl prepared the manuscript and figures. Philipp Jawny performed data collection and did statistical analysis and testing. Stephan Raab corrected the manuscript and checked for scientific relevance and correctness.
None.
None.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
