AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Sing-Yung Wu, MD, PhD, 5901 7th Street (Station 151), VA Medical Center, Long Beach, CA 90822-5201, California.
Citation: Sing-Y. Wu., Mark Chambers., Mazhar Khan., Maureen Chinweze., Thao-My Cao., et al., (2023). The Etiology of Abnormal Tsh in Veterans Cared by a Va Medical Center – One High Serum Thyrotropin is Associated with Higher 5-Years Mortality. J. Endocrinology and Disorders. 7(2): DOI:10.31579/2640-1045/133
Copyright: © 2023, Sing-Yung Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 March 2023 | Accepted: 20 April 2023 | Published: 20 May 2023
Keywords: hyperthyroidism; hypothyroidism; TSH; iodinated contrast; elderly veterans; CV/CNS; CT contrast infusion
Objective: By analyzing the etiology of abnormal TSH in randomly selected veteran patients, we set our heart on improving future clinical care/management of the clinical/subclinical hyper- and hypothyroidism in the aging veteran population.
Methods: A total of 1100 patients’ charts in alphabetical order were selected. Excluded cases of insufficient information, 897 patients’ charts were reviewed and analyzed for causes of abnormal TSH. Among them, 602 for the cause of low TSH (below 0.55 uU/mL) and 295 for high TSH (above 4.78 uU/mL) were reviewed retrospectively.
Findings: Among the 1100 patients selected, 680 (61.8%) were 60 y or older (female=44, 6.8%); 420 were under 60 y (female=80, 19.0%); significantly more female patients were found in the younger age group (P<0.001). After excluding patients with insufficient data, the most common cause of suppressed TSH is iodine-induced, CT iodinated contrast and betadine use caused 35.0% in the older group (n=126) compared to 23.6% in the younger group(n=57) (P = 0.027). The significant difference is that older veterans received more contrast CTs (P < 0.05 compared to the younger group). In both age groups with concurrent FT4 study, we found four high FT4 among 90 studies, 4.4% overt hyperthyroidism. The second most common cause of suppressed TSH is due to thyroid hormone (TH) replacement in the older group (119 patients, 33.1%) with age > 60y, significantly more frequent compared to the younger group, P<0.001. There is significantly more overt hyperthyroidism, 27.8/%, than the iodine-load induced suppression of TSH, P<0.001, due to 17 patients on TSH suppression therapy after total thyroidectomy for thyroid cancer. Among the 295 patients with elevated TSH, the most common cause of high TSH was due to hypothyroidism on T4 replacement: a total of 128 (59.3%) in the older group (N=216) is, similar to 47 (59.5%) in the younger group (N=79). In both age groups, there were 139 patients with concomitant FT4 measurement; 17 overt hypothyroidism were found, 12.2%. No significant difference is seen in the two age groups. The next most common causes of elevated TSH are CT contrast infusion, 23 (10.6%) in the older group and 7 (8.9%) in the younger group. We find high TSH is associated with a higher death rate of 101/238 (42.4%) in a 5-year follow-up (from 2016 to 2021), as compared to low TSH of 68/238 (28.6%), in the older age group, p<0.03; both were significantly higher than the age- and sex-matched general US population, 19.7%, P<0.01.
Conclusion: Even though most, ~ 90%, were subclinical, the suppressed and elevated TSH are associated with severe consequences in CV/CNS and immune-suppression complications in aging veterans. Therefore, cautious use (and more frequent check of TSH) of TH replacement and CT contrast in aging veterans is recommended. The alarming increase in 5 years death rate in older patients with elevated TSH deserves further study.
The veteran population is progressively growing older; the percentage of veterans in age > 60 y was 45.7% in 2000 and increased to 54.9% in 2021 [1]. The thyroid function in the elderly is always an intriguing problem [2]. TSH measurement is a more precise estimation of thyroid function than the studies of thyroid hormones [3]. Abnormal TSH is a commonly encountered finding, of which there are many etiologies. An early British study provided data showing that TSH levels did not vary with age among males but increased markedly among females after the age of 45 years [4]. Data from the National Health and Nutritional Survey (NHANES III) confirmed that both TSH levels and the presence of antithyroid antibodies are greater in women, increase with age, and are more common in whites than in blacks [5].
A low TSH is not always the result of suppression by elevated circulating thyroid hormones, particularly in hospitalized patients. Different etiologies/conditions can yield various levels of TSH. Mildly suppressed TSH without abnormally elevated FT4 is seen in subclinical hyperthyroidism. Markedly suppressed TSH with increased FT4 is found in overt clinical hyperthyroidism. The early recognition of clinical and subclinical hyperthyroidism in the aging veteran population is of increasing clinical importance that may result in severe cardiovascular consequences [6, 7].
On the other hand, subclinical hypothyroidism is not pre-dispose to mental or physical impairment. Strangely, a decrease in thyroid function and a shift to higher TSH values with age may contribute to extended longevity [7, 8]. However, aging VA patients have an alarmingly increased mortality rate with elevated TSH, is shown in the present study.
A total of 1100 patients’ charts in alphabetical order were selected. Two hundred-three patients were excluded from the study due to insufficient data, e.g., no VA medication, radiographic study, scanty laboratory tests, or under private physicians' care outside the VA system. Eight hundred ninety-seven patients’ charts were reviewed and analyzed, among them 602 for the cause of low TSH (below 0.55 uU/mL) and 295 for high TSH (above 4.78 uU/mL) retrospectively.
In the low TSH group, 602 patients' charts were reviewed and analyzed for the cause of low TSH (below 0.55 uU/mL) retrospectively. In the high TSH category, 295 charts were reviewed. The Chi Square statistic is used for testing relationships between categorical variables [9]. The significant level set at P value lessthan 0.05.
Student’s unpaired t test was used to assess between-group differences. Analysis of variance was used to test multi-group comparisons [9]. Significance was defined as P lessthan 0.05. Results are reported as the mean ± 1 SE. In addition, semi-log linear regression analysis of the serum thyroid functions was used to assess and compare the correlation between TSH and FT4 [10].
Causes of Reduced TSH:
In the low TSH group, 770 patients' charts in alphabetical order were initially examined, and found 441 (57.2%) were 60 years or older (female=30, 6.8%); 329 were under 60 years (female=65, 19.8%). There are significantly more female veterans in the younger age group, P lessthan 0.001.
After excluding patients with insufficient data, 602 patients’ charts were reviewed and analyzed for the cause of low TSH (below 0.55 uU/mL) retrospectively (Table 1). The most common cause of suppressed TSH is iodine-induced; CT iodinated contrast and skin disinfectant use caused 35.0% in the older group compared to 23.6% in the younger group (P=0.027). The significant difference is due to older veterans receiving more contrast CTs (P lessthan 0.05 compared to the younger group).
The second most common cause of suppressed TSH is due to thyroid hormone (TH) over-replacement in the older group (119 patients, 33.1%) with age > 60 years, significantly more frequent compared to the younger group, P lessthan 0.001(Table 1). The suppressed TSH due to unknown causes is much more frequent in younger patients (plessthan0.001).

Table 1: Age comparisons in causes of low TSH in 602 patients’ charts reviewed in a VA medical center.
Cases of Hyperthyroidism after Receiving Iodinated Contrast Agent:
We report six cases of clinical hyperthyroidism, confirmed by thyroid uptake and scan, after receiving an iodinated contrast agent when performing CT scanning (Table 2; Figures 1 and 2).
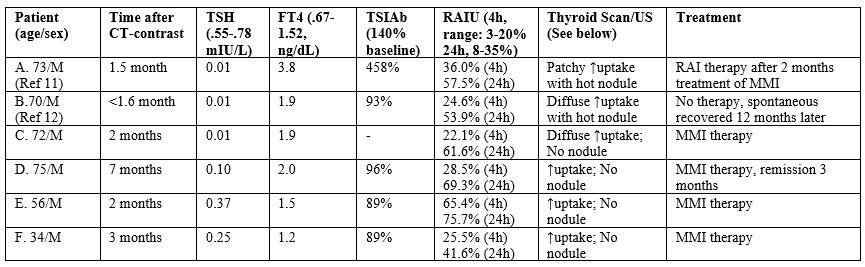
Table 2: Six cases of induced hyperthyroidism after a contrast CT.

Figure 1: Patient A: (Left) I-123 thyroid scan on 6/27/2018 showed diffusely increased uptake bilaterally (57.5% at 24 h, normal range: 8-35%) and a hot thyroid nodule in the right lower lobe. (Right) Thyroid ultrasound examination on 5/17/2018. The image is the sagittal (long) and trans-axial images There is a 1.8 x 1.3 x 2.1 cm predominantly solid nodule in the medial right lower lobe.
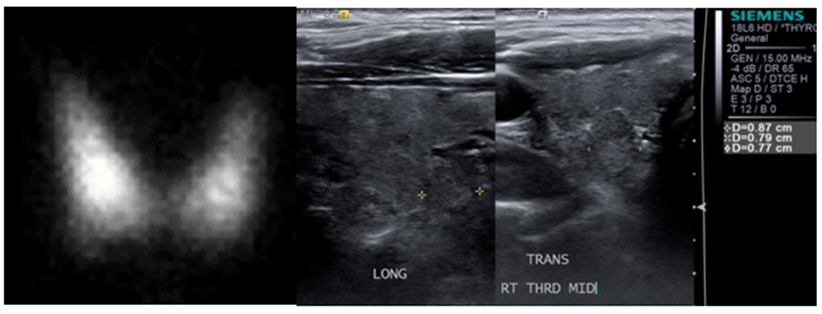
Figure 2: Patient B: (Left) I-123 thyroid scan on 2/26/2015 showed diffusely increased uptake bilaterally (53.9% at 24 h) and a hot thyroid nodule in the right lower lobe. (Right) Thyroid ultrasound examination on 1/13/2017. The image is the sagittal (long) and trans-axial images of the nodule itself with measurements (0.87 x 0.79 x 0.77 cm).
Patient A. 73 y male, has been euthyroid until after a chest CT angiogram on 3/31/18. He presented to the endocrine service with palpitation and weight loss. Suppressed TSH and elevated free T4 was found on May 18 with a positive thyroid -stimulating immunoglobulin, 458% (reference range lessthan 140%). A thyroid ultrasound examination revealed a 1.8x1.3x2.1 cm solid nodule in the medial right lobe (Fig. 1 right panel), where a hot nodule was found on an I-123 thyroid scan with a 24-hour uptake of 57.5% (Fig. 1, left panel). The clinical entity is consistent with the diagnosis of Marine-Lenhard Syndrome induced by an excessive supply of iodine by a CT angiogram [11].
Patient B. A 70-year-old male Vietnam veteran was diagnosed with clinical hyperthyroidism in January 2015, as demonstrated by biochemically suppressed serum TSH and elevated free thyroxine (FT4) concentrations. A history of an iodinated contrast CT performed in April 2013 in a private hospital. Since there was no interim VA medical care, it is presumed that he had some degree of biochemical hyperthyroidism much earlier than that of his presentation following the CT contrast administration. The patient denied palpitations, tremors, and weight loss; there were no thyroid eye disease signs. A thyroid I-123 nuclear uptake and scan in February 2015 showed a single hot nodule in the right lobe with diffusely increased uptake throughout the gland (53.9% at 24 hours; normal 8-35%) (Figure 2, Left). The uptake in the left lobe alone (without any nodule) was 21.6%, markedly elevated. He declined offered treatment with either antithyroid medications or radioactive iodine (RAI) therapy. At a follow-up visit in April 2016, the serum TSH was found to have spontaneously normalized and remained normal in December 2016. An ultrasound examination of the thyroid gland revealed a heterogeneously solid nodule measuring 0.9 cm x 0.8 cm x 0.8 cm in the right lower lobe (Figure 2, right panel) that correlated with the site of the moderately increased uptake on the nuclear scan. Serum thyroid stimulating immunoglobulin (TSI) antibody titers were negative [12]. A repeat thyroid I-123 nuclear uptake and scan showed normal uptake (17.2% at 24 hours) and only a warm nodule in the right lower lobe (Figure not shown).
Causes of Elevated TSH:
In analyzing the cause, among the 330 patients with elevated TSH, in the older age group (>60 years), the total was 238; 13 were female (5.5%), which was significantly less than females in the younger group, 25.0% (p lessthan 0.001). After excluding patients with insufficient data (N=35), the most common cause of elevated TSH was due to hypothyroidism on T4 replacement: a total of 128 (59.3%) in the older group (N=216) is similar to 47 (59.5%) in the younger group (N=79) (Table 3). The next most common causes of elevated TSH are due to iodine load (CT contrast infusion or skin disinfectant), 37 (17.1%) and medications such as amiodarone, lithium, etc., 16 (7.4%) in the older group and 7 (8.9%) and 12 (15.2%) respectively, in the younger group.

Table 3: Age comparisons in causes of high TSH in 295 patients in a VA medical center.
Among 295 patients with elevated TSH, 232 had FT4 measurements simultaneously (Table 4). The mean elevated TSH (17.28 mIU/L) in the younger group (N=60) is significantly higher than, the older age group (10.45 mIU/L, N=172, P lessthan 0.01) even though the mean FT4 values are the same in the two age groups (Fig. 4).

Table 4: Thyroid functions in veterans with elevated TSH.
Most of the Hypo- and Hyperthyroidism Induced by Iodine Load Or in the Replacement Therapy of Hypothyroidism are Sub-Clinical:
In 183 veterans with iodine-load-induced suppressed TSH, we had 90 patients with FT4 study at the same time in 2016 (Table 5). Only four patients with abnormally high FT4 indicate that about 95.6% of this group is subclinical hyperthyroidism. On the other hand, in the hypothyroid on T4 group, there are 27 having abnormally high FT4; thus, 27.8% are overt hyperthyroidism, significantly higher than the iodine-load group, P lessthan 0.001. However, after removing 19 patients with thyroid cancer on T4 suppression therapy, the clinical hyperthyroid cases dropped to 8 cases in 78 (10.2%), no longer statistically significant to the iodine-load-induced hyperthyroidism. In the high TSH group, the subclinical hypothyroidism is similar in Iodine-load (92.9%) vs. the On-T4 therapy (87.2%) group (Table 5).

Table 5: Thyroid Functions in Veterans with abnormal TSH induced by an iodine-load or replacement therapy in hypothyroidism.
Thyroid Dysfuncton Induced by Iodine-load:
The suppressed TSH (mean = 0.32) induced by iodine load was significantly lower for the older age group (n=62) as compared with the younger group (mean = 0.38 mIU/L, n=28), P=0.027 (Table 6).

Table 6: Thyroid Functions in Iodine-load Induced dysfunction.
Of 46 veterans with iodine-load-induced elevated TSH, 14 had both TSH and FT4 measurements and found one abnormally low FT4 indicating most are subclinical hypothyroidism. Even though FT4 showed no apparent changes, the mean value (1.14 ng/dL, n=62) in the older age group is significantly higher in the suppressed TSH group than in the elevated TSH group (0.93 ng/dL, n=12), P = 0.003 (Table 6).
Thyroid Dysfunction found in the T4-therapy Group:
In 602 patients with suppressed TSH, among 157 patients on T4 replacement therapy, 126 had FT4 measurements concurrently. 97 patients were > 60 yrs with significantly higher mean TSH + SE level (0.22 + 0.02 mIU/L, normal 0.55-0.78 mIU/L) than the younger group (0.14 + 0.03 mIU/L, n=29) (Table 7). Twelve thyroid cancer patients on T4 replacement therapy had mean TSH + SE (0.15 + 0.04 mIU/L), which is significantly lower than the mean TSH in the older age group (0.22 + 0.02 mIU/L) (Table 6). Similarly, lower mean TSH is also found in 7 young thyroid cancer survivors on T4 (0.07 mIU/L).
0f patients aged > 80 yrs (N=72, 9 were females), 44 were on TH, reaching 61.1%. Among the 44 patients on T4, 26 had both TSH and FT4 measurements on the same date: mean TSH, 0.20 mIU/L (+ 0.03, SE,) and FT4, 1.42 ng/dL (+ 0.05, SE, normal 0.67-1.52 ng/dL) (Table 7).
Of 175 patients with elevated TSH and were hypothyroid patients on replacement therapy, 125 had FT4 measurements simultaneously. 92 patients were > 60 yrs with significantly lower mean TSH + SE level (12.45 + 1.43 mIU/L) than the younger group (24.92 + 7.14 mIU/L, n=29) even though the mean FT4 values were similar (Table 7).
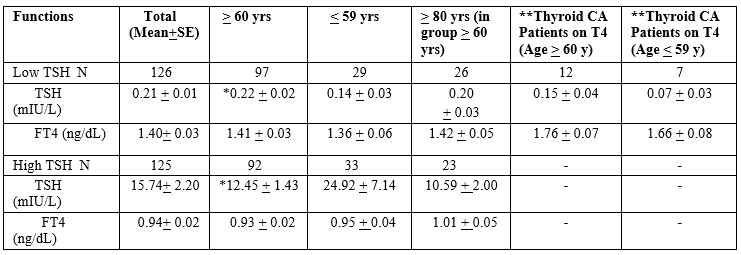
* significantly different from lessthan or equal to 59 yrs. Group.
** Thyroid cancer survivors on T4 therapy to suppress TSH.
Table 7: Thyroid functions in hypothyroid patients on replacement therapy with abnormal TSH (with concurrent FT4 measurement).
TSH and FT4 Were Found to have Low Correlations:
We plotted the linear correlation in 62 paired TSH and FT4 and found the Pearson correlation coefficient, r = -0.222, poor statistical correlation (Plot not shown). Similar r values are found in TSH and FT4 correlations in the younger age group (n=28) or in two age groups with elevated TSH (Figures not shown).
Correlation of TSH and FT4 in 126 veterans with suppressed TSH (Fig. 3, left) and 125 veterans with elevated TSH (Figure. 3, right) on T4 replacement therapy with hypothyroidism suppressed TSH. The Pearson correlation coefficient was R=-0.1804 for the suppressed TSH group and R=-3921 for the elevated TSH group. The FT4 correlates poorly with changing TSH. Similar poor correlations between TSH and FT4 are observed in iodine-load-induced abnormal TSH groups (Figures not shown)

Figure 3: Correlation of TSH and FT4 in 126 veterans with suppressed TSH (left) and 125 veteran with elevated TSH (right) on T4 replacement therapy with hypothyroidism suppressed TSH.
Other Clinical Aspects in Patients with Elevated TSH:
In the older age group with increased TSH, a total of 44 patients had antibody studies (Table 8); 39 were performed in the male group and found 11were positive for anti-thyroid-peroxidase (TPO) antibody (28.2%), and 7 were positive for anti-thyroglobulin (Tg) antibody (17.9%) (Table 8). However, in all five elderly females tested, both antibodies studied were negative. In the younger age group, 14 males had antibody studies; eight were positive for anti-TPO antibody (4 were positive for anti-Tg antibody), while in the eight female, young veterans, three were positive for Anti-TPO antibodies, and two were positive for the anti-Tg antibody. Interestingly a significantly more positive in Anti-TPO Antibody, but not Anti-Tg antibody, in the younger group than in the older group, P = 0.032. The lack of positive TPO-AB in the elderly group may not contribute to more females in the younger group (36.4% vs. 11.4% in the older group) since all five female patients in the older group had negative TPO antibodies (Table 8).
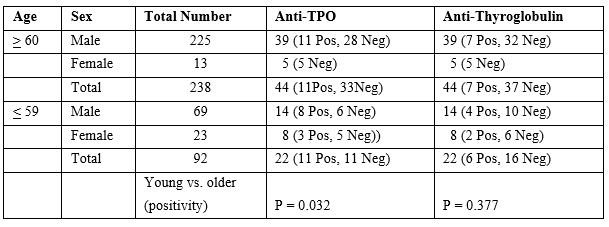
Table 8: Antibody studies in high TSH and older group (>60 years) and compared with younger group (lessthan 59)
Elevated TSH is Associated with a Higher 5-Years Mortality Rate
We find high TSH is associated with a higher death rate of 101/238 (42.4%) in a 5-year follow-up (from 2016 to 2021), in the same numbers of veterans equal or older than 60 yrs of age with low TSH (68/238, 28.6%, p lessthan 0.03) (Table 9). Then we found more veteran in the age groups equal and older than 80 in the high TSH group, 62 vs 44 in the low TSH group, P = 0.11. As compared to age- and sex-matched low TSH, there were 79 deaths in 5 years (33.9%), P=0.162 comparing to the high TSH group (Table 9).
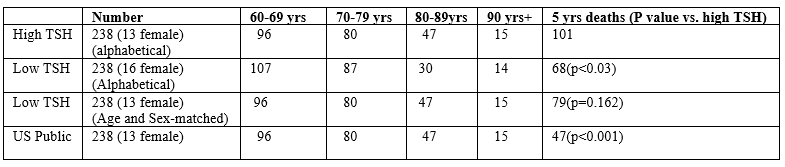
Table 9: Comparison of 5-years mortality rate in low and high TSH group in patients age equal or older than 60 years.
Even though there is no statistical difference between these two aging groups after age and sex-matching, however, the excess 22 deaths in the high TSH group remained to be explained. The 5-year mortality rate is also much higher in the elevated TSH group compared to the age- and sex-matched general US population, 19.7%, P lessthan 0.001 [13].
We also find high TSH is associated with a higher death rate in the younger group of 8/92 (8.7%) in a 5-year follow-up, compared to veterans equal or younger than 60 yrs of age with low TSH (3/106, 2.8%, p lessthan 0.05) (Table 10). When we combine these two age groups, the high TSH will have a significantly higher death rate than the alphabetically selected low TSH group (p lessthan 0.006) or age-/sex-matched (p lessthan 0.05).
The 5-year mortality rate is also higher in the elevated TSH group compared to the age- and sex-matched general US population, 2.2%, P lessthan 0.03 [13]. Due to the number is small, further study is needed.
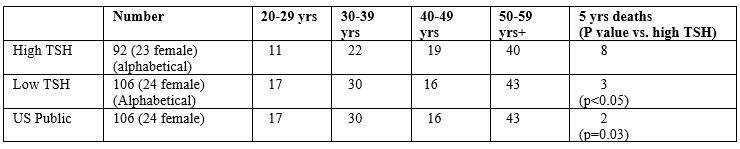
Table 10: Comparison of 5-years mortality rate in low and high TSH group in patients age equal or younger than 59 years.
TSH measurement allows for a more precise estimation of thyroid function than the thyroid hormones studies. However, the diagnosis of overt hyper- or hypothyroidism requires the measurement of FT4 (Figure. 3). In our studies, FT4 is poorly correlated with TSH, which is consistent with prior studies, especially in older patients [14-16].
In veteran patients with suppressed TSH, excluding thyroid cancer patients on T4 therapy, most of these patients are subclinical, ~90% (Table 5); we found a high occurrence of low TSH following an iodine-load(s) in the older age group, which is consistent with older veterans receiving more IV contrast CT studies for cardiovascular (CV) and neoplastic diseases. In the present study, the second most common cause of suppressed TSH is due to thyroid hormone (TH) replacement in the older group (119 patients, 33.1%) with age > 60y; significantly more frequent compared to the younger group, P<0> 80 yrs (N=72, 9 were females), 44 were on TH, reaching 56.1%. Among the 44 patients on T4, 26 had both TSH and FT4 measurements showing significantly suppressed TSH (0.20 mIU/L) and close to lower normal limit in mean FT4 (1.42 ng/dL), indicating a significant proportion of this advanced age group with T4 replacement reached overt hyperthyroid range. A critical review and meta-analysis reported a 20% increased mortality in patients with overt hyperthyroidism, and six studies assessing cardiovascular mortality were included [17, 18].
On the other hand, studies have examined the relationship between Subclinical hyperthyroidism and mortality in large populations. A study included 1,191 subjects aged 60 or older at the initial inclusion and thyroid function testing. This 10-year study observed excess mortality from cardiovascular causes in subjects with TSH lessthan .5 mIU/L. Further subdivision by mortality causes showed both cardiac disease proper and cerebrovascular disease among the causes [17]. While confirming the association with atrial fibrillation, other studies failed to demonstrate increased mortality in older subjects with subclinical cases [19,20]. Other large meta-analyses showed a slightly increased mortality in subjects older than 65 with the diagnosis of hyperthyroidism [21-24].
In patients with elevated TSH, in the older age group (similar to the younger group), the most common cause of elevated TSH was hypothyroidism on T4 replacement (close to 60%, Table 3). The next most common cause of elevated TSH is CT contrast infusion. Iodine-containing contrast infusion causes the acute suppression of TH synthesis (Wolff-Chaikoff effect) and significantly increases TSH concentrations up to 6.4 mIU/L in about 1/5 of patients within five days [17,25,26].
It is essential to recognize that the elderly are at risk of developing iodine-induced or iatrogenic thyroid dysfunctions, which often are transient and reversible. Thus, the morbidity from excessive therapy can be avoided [12]. In 2019, the number and proportion of CT procedures conducted with no contrast media in the United States exceeded those conducted with contrast media, according to IMV Medical Information Division’s 2019 CT Market Outlook Report [27]. IMV estimates that 52% of the 91.4 million CT procedures conducted in the US in 2019 were performed without contrast media, up from 33% of the 76.0 million procedures conducted in 2007. This indicates that the US radiologists have alerted to the adverse effect of CT contrast media. However, from the ACR Manual on Contrast Media [28], the concern of CT contrast media mainly was on contrast-induced nephropathy, not on thyroid dysfunction in the elderly. The present study may call for attention and further study in contrast-induced thyroid dysfunction. In the 2021 Guideline, the European Thyroid Association (ETA) suggested the measurement of baseline serum TSH in high-risk patients for iodine-containing contrast-induced thyroid dysfunction, especially in the elderly and subjects at risk for cardiovascular diseases. If serum TSH is abnormal, thyroid hormones (T3 and/or T4) should be measured [29]. Prior to CT contrast exposure, ETA suggested a thorough case-finding approach based on identifying those persons most likely to have undiagnosed thyroid disease and measuring thyroid function 3–4 weeks after contrast exposure in high-risk patients for possible hyperthyroidism, especially in the elderly and/or those with an underlying unstable cardiovascular disease [30].
Thyroid peroxidase antibodies can be found in up to 30% of unselected subjects aged 70 and older [4]. This is similar to our result in 28.2% of older male veterans (Table 8). In the NHANES study [5], people > 70 years old with TPO antibodies had an incidence of TSH > 4.5 of about 50%, compared to 10% in the “disease-free” group [30], validating the removal of elderly subjects with thyroid autoantibodies from the “healthy control” groups. In the groups aged 70–79 and older than 80, the 97.5th percentile TSH was found higher (than the normal upper range) at 5.9 and 7.5 mIU/mL, respectively. However, in the same population, total thyroxine decreased with age.
A decreased thyroid function and a shift to higher TSH values with age may contribute to extended longevity [7, 8]. However, we have a surprising but alarming finding in our VA patient populations, a higher TSH group in both young and elderly is associated with a higher mortality rate than the same age groups with suppressed TSH (Tables 9 and 10). We postulate that the higher mortality could be due to compromised immunity in hypothyroidism. A central role of thyroid hormones in the modulation of the immune system is confirmed by the influence of T3 and T4 in cytokine maturation and release. This process involves the activation of MAPKs and is mediated by phosphorylation of the Signal Transducer and Activator of Transcription 1α [31]. Furthermore, hypothyroidism correlates with decreased humoral and immune cell responses [32]. Moreover, levels of circulating thyroid hormones positively match up with immunological reactivity in healthy individuals, such as in the physiological maintenance of lymphocyte subpopulations [33]. Recently, it has been shown that T3 increased the number of IL-17-expressing T lymphocytes by activating dendritic cells in vitro [34]. The association of immunity and higher mortality rate with elevated TSH, although mostly subclinical, deserves further study.
Furthermore, many studies showed that adequate thyroid hormone levels are required to achieve optimal outcome from any surgical procedures [35]. Significant differences are found between patients with subclinical and euthyroid patients undergoing a CV surgical procedures regarding complications [36]. A strong association between non-thyroid illnesses with low T3 at admission and increased risk of post operative myocardial dysfunction and death in patients had coronary artery by-pass grafting [37]. Further clinical trials assessing management in older hypothyroid patients are firmly required [38].
Because of the vulnerability to CV/CNS and immunosuppression and severe consequences in clinical/subclinical hyperthyroidism and hypothyroidism, as well as higher mortality rate with elevated TSH in the older group, cautious use (and more frequent check of TSH) of TH replacement and CT contrast in aging veterans is recommended. Further, a more extensive control study in the VA population is needed.
This work was supported in part by the Department of Veterans Affairs and SCIRE [Southern California Institute of Research and Education] to S-y W and the National Institutes of Health (NIH) grants 1RO1 AR073298 and RO178843 to H-b Z.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
