AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Fatemeh Rahimianfar, Research and Clinical Center for Infertility, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd.Iran.
Citation: Fatemeh Rahimianfar, Mahtab Rahimianfar and Sahar Eshghjoo, (2024), The comparative analysis of Vascular Endothelial Growth Factor-A (VEGF-A) impacts in Ovarian Hyper Stimulation Syndrome and Obesity, J. Obstetrics Gynecology and Reproductive Sciences, 8(4) DOI:10.31579/2578-8965/218
Copyright: © 2024, Fatemeh Rahimianfar. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 May 2024 | Accepted: 17 May 2024 | Published: 03 June 2024
Keywords: OHSS; obesity; VEGF-A; ovarian hyper stimulation syndrome; vascular permeability; adipose tissue; angiogenesis; adipocytes; endothelial cell; IVF; infertility
Ovarian Hyper Stimulation Syndrome (OHSS) is an iatrogenic complication that arises during in-vitro fertilization (IVF) procedures for infertility treatment, representing a growing global concern. This disorder is characterized by several risk factors, clinical features and laboratory manifestations. The underlying pathophysiology involves proinflammatory mediators, with VEGF-A playing a pivotal role. VEGF-A significantly impacts vasculature and contributes to the resulting pathophysiology of OHSS and other related diseases. Interestingly, obesity, another example, demonstrates distinct VEGF-A effects on vasculature, differing from its role in OHSS. In this review article, our aim is to describe pathophysiology of OHSS and obesity as well as providing updated insights into these disorders, highlighting how VEGF-A modulates vasculature through unique intracellular signaling pathways in endothelial cells.
1.Introduction
Currently, a vast number of people suffer from infertility[1]. In the Unites States, around 12.1% of reproductive-age women have this problem [2]. It is defined as an individual’s inability to conceive after one year (or longer) through a natural process. Infertility is classified as primary (lack of history of pregnancy in the past) and secondary infertility (failure to repeat pregnancy after at least one conception) [3]. There are several risk factors for infertility including, genital infections, congenital uterine abnormalities, prolonged oral contraception, hormonal disorders, sociocultural factors, etc. Moreover, due to increasing life style factors attributed, in part, to smoking, sexual transmitted diseases (STDs), obesity, alcohol use, and lake of physical activity, the prevalence rate of infertility has grown [4]. Therefore, assisted reproductive technologies (ARTs) are utilized to help those infertile couples in treatment of this multifactorial disorder [5].
The uses of ARTs have increased during recent years. ARTs are defined as all procedures for commencing conception, which consist of numerous types such as in-vitro fertilization (IVF), intrauterine insemination (IUI), intracytoplasmic sperm injection (ICSI), gamete and embryo cryopreservation, preimplantation genetic screening, preimplantation diagnosis, and/or the use of fertility medication. Among these different kinds of ART, IVF is the most predominant type [6].
IVF procedure is categorized in 4 basic steps. To clarify, high- dose gonadotropins are used for controlled ovarian hyper stimulation (COH) in the first step. Additionally, patients are triggered by using such drugs as human Chorionic Gonadotropin (hCG) after reaching desired count /size of ovarian follicles so as to initiate the ovulatory cascade, yielding the final follicle maturation process. Afterwards, oocytes are retrieved from the ovaries in surgery rooms and are transferred to special laboratories to achieve fertilization. In step three, embryos are cultured in equipped mediums for a few days in order to prime the embryos for transfer (3 days to reach the eight-cell stage or 5 days to reach the developed embryo in blastocyst stage). In the final step, embryos are transferred into the uterus, which is known as Fresh-ET, and/ or frozen for the future transfer [6]. In spite of the fact that IVF is beneficial for most of infertile couples, ovarian hyper stimulation syndrome (OHSS) can occur as one of its complications [2, 6, 7]. In this study, our aim is to overview the pathophysiology of OHSS and its vasculature events and then dive into obesity which has both similarities and differences in some points about vasculature changes.
OHSS is an important iatrogenic condition during IVF procedure, which has the potential to be life-threatening in its severe forms [5-8]. In other words, OHSS often develops as the consequence of gonadotropins (mostly hCG) administration which facilitates oocytes maturation and is released during IVF treatment [1, 2]. There are several risk factors for OHSS (table 1). For better perception, researchers categorized OHSS risk factors into two different groups: primary risk factors and secondary risk factors. Primary risk factors include past history of OHSS, low body mass index (BMI), PCOS (which is also a risk factor for infertility), high antral follicle count (AFC) > 8, age < 30> 35 years old are at high risk of infertility), and high amounts of basal anti-mullerian hormone (AMH) > 3.36 ng/ml (high specifity and sensitivity (81.3%, 90.5%)). The secondary risk factors are associated with ovarian response to COH, and they consist of small follicle counts > 14 with the diameter of around 11mm (8-12 mm) in the triggering day, rapid elevation in serum estradiol concentration > 2500 pg/ml, and large retrieved oocytes count >20 [3, 4, 9-13]. Furthermore, hCG a complex heterodimeric glycoprotein hormone, is regarded as one of the main risk factors for OHSS development [14, 15]. In 2020, one study reported that patients with dyslipidemia are in the higher risk for development of OHSS [11]. Along with different types for categorization of these risk factors, numerous attempts have been carried out to classify OHSS.
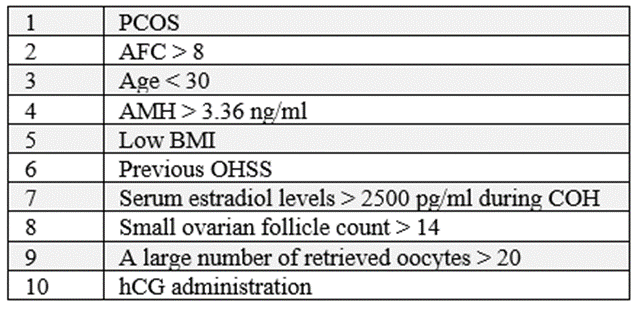
Table 1: The most common risk factors for OHSS.
Two sorts of classifications have been determined for this potentially lethal complication: Firstly, based on timing presentation in which two forms have been described: early and late. Early, OHSS is commonly trigger-related and it happens within 10 days of induced ovulation. The late OHSS is mainly pregnancy-related because of excessive amounts of endogenous hCG from a developing pregnancy, and it appears after ≥ 10 days following oocyte retrieval [8, 12, 14, 16]. Secondly, based on clinical, imaging plus laboratory features, in which OHSS is categorized into 4 stages: mild, moderate, severe, and critical. The milder form is the most prevalent among other stages of OHSS [2]. According to the second classification type, OHSS appears with various features related to severity.
There are an extensive range of clinical presentation for OHSS from mild to critical although these stages are not purely separated from each other. OHSS manifestations appear because of bilateral cystic enlargement of exceedingly luteinized ovaries [13]. Mild ovarian enlargement (ovarian diameter: 5-12 cm) makes the mild form of OHSS. Initial clinical presentations of mild OHSS (Figure 1) are commonly associated with abdominal distention, which include mild abdominal pain, poor appetite, nausea, vomiting, mild diarrhea, and bloating [1, 2, 8, 12, 13] even though The symptoms of this stage might be imperceptible.
N/V; Nausea/ Vomiting. According to the figure, mild form of OHSS can be symptomatic or even without any symptoms in clinical presentation and laboratory findings. In these cases, mild OHSS will be distinguished by ovarian enlargement via ultra-sonography.
Figure 1: The most important clinical presentations and laboratory features of Mild OHSS.
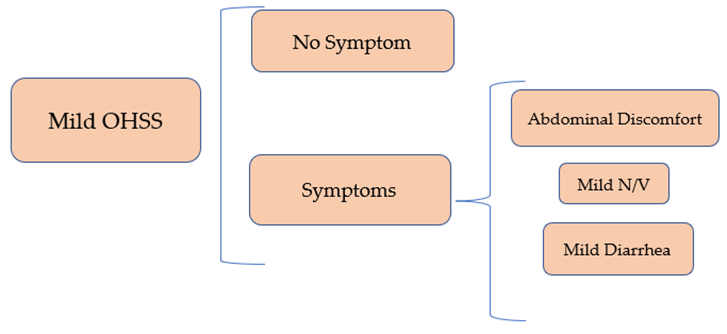
In moderate OHSS (Figure 2), detectable ascites on ultrasound is added to the diagnostic criteria, and an apparent clinically ascites (grade 2) plus other more severe manifestations are revealed in the severe form. Indeed, clinical presentations in the severe forms (Figure 3) include severe abdominal discomfort, severe shortness of breath (SOB), rapid weight gain around > 1 kg in a day, severe nausea and vomiting, venous thrombosis, oliguria, pleural effusion (signs: tachypnea, crackle upon auscultation), intra-abdominal hypertension (IAH) which is defined as intra-abdominal pressure (IAP) > 12 mmHg, hemodynamic changes and so on. Also, the critical form manifestations (Figure 4) include arterial thrombosis, anuria, thromboembolism, pericardial effusion, acute respiratory distress syndrome (ARDS), massive hydrothorax, sepsis, shock, and maybe even death [8, 13, 14, 17]. Laboratory findings are different related to the severity of the disease. For instance, in the mild stage, there is no significant laboratory changes most of the times. In the moderate form of OHSS, laboratory findings are such as white blood cells (WBC) > 15000/ ml, hematocrit (HCT) > 41%, and hypoproteinemia (17). In the severe stage, the laboratory changes get more serious, including HCT> 55%, WBC > 25000/ ml, Na < 135> 5 meq/ml, serum creatinine (Cr) > 1.6 mg/dl, increasing liver enzymes, and clearance of Cr < 50>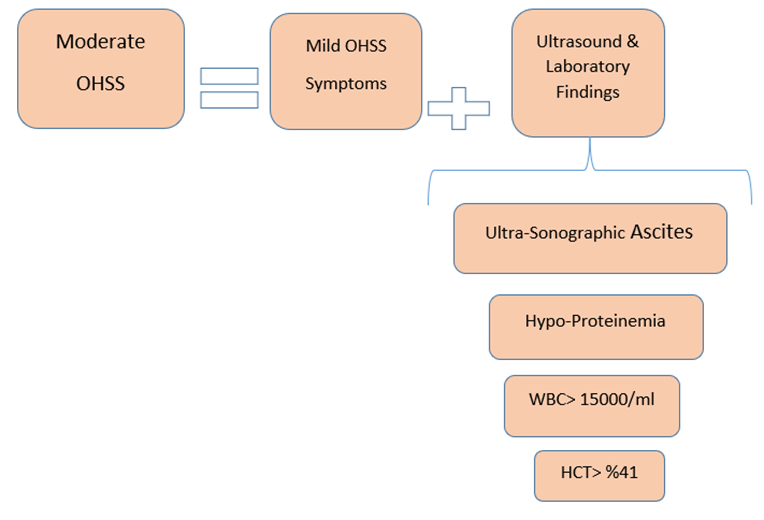
HCT; hematocrit, WBC; white blood cell. In moderate form of OHSS, in addition to mild clinical symptoms, there is ovarian ascites which will be diagnosed by Ultrasound. Moreover, in this stage, patients reveal laboratory changes.
Figure 2: The most important clinical presentations and laboratory features of Moderate OHSS.
In details, to explain more about the manifestations of OHSS, we should state that typically, as the severity increases, the signs and symptoms get more serious and even lethal. For instance, clinical ascites, intra-abdominal hypertension (IAH), hemoconcentration, infection, and severe hemodynamic changes which are highly dangerous for patients [2].
IAH, one of the severe manifestations, is defined as intra-abdominal pressure (IAP) > 12 mmHg. As a matter of fact, IAP is determined by the abdominal walls elasticity and the content of the abdominal cavity. IAP increase occurs due to accumulation of fluids or lesions which occupy the abdominal space. There are numerous methods for IAP measurement, in which trans-vesicular pressure measurement through a bladder catheter is one of the most prevalent and certain methods. Anyway, Normal IAP range is less than 5 mmHg. Also, in chronic obesity, IAP has been reported around 10-15 mmHg. Detrimental ranges of IAP start from more than 12 mmHg, which have been mentioned previously in IAH definition. IAH is separated into two different groups based on timing of IAP increasing: first of all, acute IAH which occurs mostly in patients who have undergone surgeries. In this type, IAP adds up over a few hours. Secondly, subacute IAH which happens along with medical disorders like pancreatitis. In this type, IAP rises over a few days. Additionally, four grades have been determined for IAH: 1) IAP 12-15 mmHg, 2) IAP 16-20 mmHg, 3) IAP 21-25 mmHg, and 4) IAP > 25 mmHg. In grade I, there are venous stasis and renal impairment. In grade II and III, physiologic impacts include decreased lung compliance and reduced splanchnic blood flow. Also, oliguria happens during grade II and III. Finally, in grade IV, anuria occurs with a more serious physiological effect known as decreased central perfusion pressure (CPP) (18). As a result, IAH induces oliguria (i.e. urinary output < 20> 5 meq/L, and metabolic acidosis), increased alanine & aspartate aminotransferase values, etc. [2, 8, 11]. According to some studies, there is another term known as abdominal compartment syndrome (ACS) which occurs by IAP elevation plus organ dysfunction.
Together, ACS might occur in severe OHSS and there are four grades for ACS a little similar to IAH groups: 1) IAP 10-15 mmHg, 2) IAP 16-25 mmHg, 3) IAP 25-35 mmHg, and 4) IAP > 35 mmHg. In other words, ACS with IAP > 20 mmHg is accompanied by organs dysfunction. Moreover, there is another classification for ACS as primary or secondary. Primary ACS is due to operation or trauma. However, secondary ACS is because of capillary leakage. Indeed, OHSS is regarded as a form of secondary ACS. In addition, a triad for ACS has been determined: 1) Respiratory effects: when IAP increases, the diaphragm comes up so that patients suffer from dyspnea and sometimes pleural effusion due to negative impacts on lungs. 2) Venous effects: when IAP raises, decreased venous return happens due to inferior vena cave (IVP) compression. 3) Intestinal effects: when IAP increments, it causes visceral compression which is the result of intestinal obstruction and in this part, patients complain about loss of appetite as well as nausea and vomiting which occur gradually. Overall, parts 1 and 3 (respiratory and intestinal effects) are observed in OHSS [18].
WBC; white blood cells, HCT; hematocrit, SOB; shortness of breath, IAH; intra-abdominal hypertension, ACS; abdominal compartment syndrome, N/V; Nausea/Vomiting. According to the figure, the severe form of OHSS is accompanied by obvious clinical ascites as well as other dangerous clinical and laboratory findings.
Figure 3: The most important clinical presentations and laboratory features of Severe OHSS.
In addition, another severe sign of OHSS, hemoconcentration, is described as increased hematocrit (HCT), thrombocytosis, and leukocytosis. Hemoconcentration is a predisposing factor for thrombosis and hyper coagulopathy. Thrombosis mainly occurs in the venous system in which the jugular and subclavian veins are the most frequent venous locations [2, 19].
Moreover, OHSS patients are at higher risk for different kinds of infections in different sites, including urinary tract, lungs, and upper respiratory tract, etc. Furthermore, these patients might experience some other infections consisting of intravenous line phlebitis, gluteal abscess due to progesterone injection, and post-operative wound infections [2, 20]. Causative organisms for these such infections in severe OHSS include Klebsiella pneumonia, Escherichia coli, Pseudomonas aeruginosa, Morganella morganii, Proteus mirabilis, and Proteus vulgaris. [2, 21]
OHSS also might be accompanied by hemodynamic changes from a simple hypotension until different types of shocks such as hypovolemic, obstructive, distributive, and septic shock related to severity of the disease. Hypovolemic shock happens because of third space or gastro intestinal loses, obstructive shock due to pulmonary embolism or cardiac tamponade, distributive shock as the result of inclement inflammation, and septic shock because of infections [2, 11].
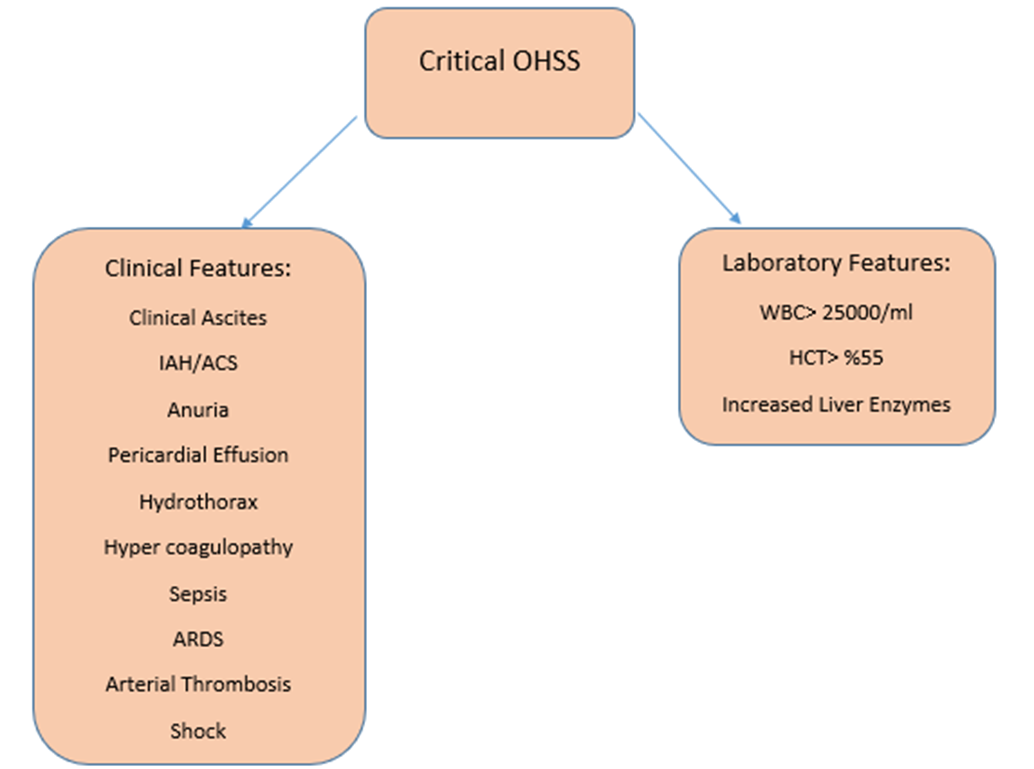
HCT; hematocrit, WBC; white blood cell, ARDS; acute respiratory distress syndrome, IAH; intra-abdominal hypertension, ACS; abdominal compartment syndrome. As you notice in the figure, the critical stage of OHSS possesses much more serious manifestations than other stages which is considered to be further life-threatening.
Figure 4: The most important clinical presentations and laboratory features of Critical OHSS.
To summarize, a number of most important clinical and laboratory findings in OHSS have been shown in figure 1. These manifestations of OHSS specially in the severe forms, predominantly are caused by fluid shifting into the third space of the body (mostly in peritoneal compartment, less frequently in pleural and pericardial space) [2, 19]
1.1.1 Third spacing phenomenon
Third spacing in OHSS is the result of increased vascular permeability. There are two main proposed models for increased vascular permeability: first, formation of vesiculo-vacuolar organelles (VVOs) which are a kind of trans-endothelial channels generated from vesicles or vacuoles. The next model which is deserved to be taken into account is transient dissolving of endothelial junctions [22]. For more explanation, endothelial cells are the bulk of the innermost layer of vessels; they are actually simple squamous cells. Three sorts of endothelial cell junctions have been discovered: gap, tight, and adherence junctions. Each of these different cell junctions possess their own constituents. For instance, in gap junctions, connexins are
participated as the junction generators. Nevertheless, in tight junctions, some other molecules are involved such as claudins, nectin, occluding, and so on.
The constituents of adherence junctions are such as nectin, VE-cadherin, etc. Furthermore, inner side of endothelial cells are covered by glycocalyx which is made up of two layers of fiber matrix and full of proteoglycans. The glycocalyx layer is bound to the membrane of endothelial cells and contributes to the modulating of vascular permeability so that damaged glycocalyx may be also associated with increased permeability of vessels [23]. Plasma possesses three principle macromolecules, including globulins, fibrinogen, and albumin. They are in charge of different tasks like maintaining the pressure balance between blood and interstitial space. In addition, inflammatory cells adhere to endothelial cells so as to pass through endothelial junctions or via the thin endothelial cells directly [22]. Somehow the same probably occurs in OHSS.
In OHSS, the increased capillary permeability is fundamentally the main pathophysiologic feature of massive luteinization of enlarged-ovarian granulosa cells due to high dose hCG (exogenous or endogenous). In addition, some proinflammatory and vasoactive factors have directly or indirectly been involved in this process, resulting in shifting of intravascular fluid into extravascular compartment which is known as third space. The vasoactive factors include interleukin (IL)-1β, transforming growth factor (TGF)-α, TGF-β, endothelin-1, insulin-like growth factor 1 (IGF-1), epidermal growth factor (EGF), von Willebrand factor (VWF), prostaglandin, basic problast growth factor (BPGF), inhibin, prolactin, estrogen, histamine, serotonin, renin-angiotensin-aldosterone system, and most importantly, vascular endothelial growth factor (VEGF) [1, 13, 24-28]. Among the factors mentioned above, a few of them are not strongly evidenced to approved as key mediators for increasing vascular permeability in OHSS, despite of being supposed as possible factors for enhancing vascular permeability in the past [17]. Therefore, we explain more about common recent proved mediators affecting vascular permeability, of which VEGF is the most principle.
1.1.1.1 VEGF
VEGFs also called vascular permeability factors (VPFs), are signal proteins accompanied by angiogenesis as well as vasculogenesis properties. Indeed, they are the member of the platelet-derived growth factor family of cysteine-knot growth factors. There are 7 types of VEGF, including VEGF-A (i.e. VEGF), VEGF-B, VEGF-C, VEGF-D, the placental growth factor (PlGF), the viral genome-derived VEGF-E, and VEGF-F which is encoded in the venom of some snakes [29-33]. Moreover, there are 3 types of VEGF receptor (VEGFR). To clarify, VEGFR-1 is the receptor for VEGF- A, B, PlGF. VEGFR-2 is the receptor for types A, E, C, and D and VEGFR-3 is the receptor for VEGF-C and D. In humans, VEGFRs are encoded by the FLT genes such as FLT-1 which encodes VEGFR-1, and FLT-4 which encodes VEGFR-3. VEGF- C/D are essential for the regulation of lymph-angiogenesis plus angiogenesis at an early embryogenesis less importantly [32-35]. VEGF-B is involved in embryonic angiogenesis (specifically, myocardial tissue) [36]. In addition, PlGF plays a main role in pathological angiogenesis (like retinopathy especially those with diabetes retinopathy) and inflammation [37]. Among different kinds of VEGF, type A was discovered initially and is the most responsible type of VEGF playing an important role in this disorder.
1.1.1.1.1. VEGF-A; increasing vascular permeability
VEGF-A actually gets involved in capillary permeability and pro-angiogenic activity. Indeed, it is made by those cells underwent stress conditions, such as endothelial cells. It is expressed during female reproductive cycle remodeling as well as atherosclerosis and cancer [29, 34]. During OHSS, VEGF-A after getting released into the blood circulation, binds to its specific receptor on the cell surface to exert its effects on the body (figure 5). For more specific explanation, endothelial cells connect to each other tightly by some protein complexes which are known as adherens junctional proteins (AJ proteins). There are several kinds of AJ proteins like β-catenin, VE-cadherin, α-catenin, and p 120-catenin. These proteins maintain vascular integrity so as to make a vascular barrier. The barrier is able to breakdown due to some reasons such as endocytosis, phosphorylation, S-nitrosylation, and/or cleavage of these proteins. The vascular barrier integrity is dynamically modulated by VEGFR signaling. As a matter of fact, VEGF enhances VE-cadherin and β-catenin tyrosine (Y)-phosphorylation, followed by capillary leak. Also, it is recently evident that a kind of kinase known as Src-family protein-tyrosine kinase (PTK), is activated by VEGF and plays an important role in promoting AJ phosphorylation. Src-family PTK is also able to get actuated by integrin receptors which cross-talk with VEGF in vascular permeability controlling. To clarify, VE-cadherin phosphorylation at Y658, Y731 or β-catenin phosphorylation at Y654, both by Src mediation, induce complicated AJ stability regulation. Moreover, β-catenin phosphorylation at Y142 disrupts α-catenin binding. In spite of the fact that in-vitro phosphorylation of β-catenin at Y142 by PTK6 has been demonstrated, the modulating of this kind of AJ protein phosphorylation remains unknown in-vivo. There is another type of PTK, called focal adhesion kinase (FAK) which is actuated by both integrins and VEGF. When FAK binds to paxilin, followed by its localization to cell adhesions, and a FAK/αvβ5 integrin signaling structure formation, actin-myosin tension is generated and cell motility increases [32, 38-40]. Consequently, VEGF-A binds to VEGFR and activates the receptor so that cell signaling induces phosphorylation of AJ proteins resulting in vascular barrier breakdown and increased vascular permeability.
As mentioned above, VEGF-A holds two important impacts on vasculature. First, the increase in vascular permeability, which was explained in the previous paragraphs by the description of OHSS as an example. The next role that should be taken into account is that VEGF-A also plays a principal role in physiological and pathological angiogenesis which occurs in obesity as an instance [32, 33, 41].
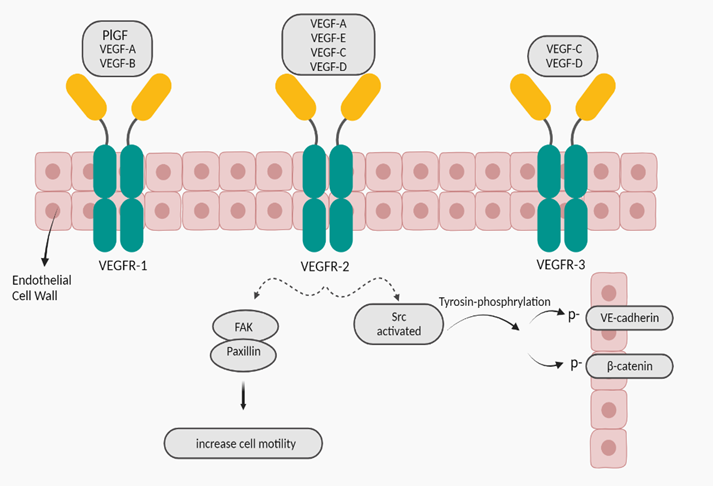
PlGF; placental growth factor, FAK; focal adhesion kinase
Figure 5: VEGFRs and cell signaling; after binding VEGF-A to VEGFR-2, a special cell signaling sets out to degrade AJ proteins between endothelial cells so that yields increased vascular permeability (32, 38-40, 42).
1.2. Obesity
Obesity incidence is aggregating over the last few decades, leading to be one of the main health problems worldwide [43, 44]. According to WHO, approximately 20% of adult population around the world, will suffer from obesity by 2025 [44, 45]. To clarify the concept of obesity, we should state that the imbalance between energy intake and energy consumption underlies obesity and overweight. [46-50]. The next thing which is deserved to be pay attention is that changes in diet quality might also cause obesity [51]. Obesity is in fact a complex chronic disorder, which is specified as three sorts; generalized obesity (BMI ≥ 30 kg/m2), extreme obesity (BMI > 40 kg/m2), and central obesity in which the abdomen fat gets accumulated excessively [48, 52, 53]. There are a number of factors such as epigenetic changes, increasing the risk of obesity. Epigenetics is in fact a phenomenon in which some variables like nutrition and lifestyle lead to make some alterations in gene expression in terms of histone modification, non-coding RNA, and DNA methylation, without any changes in DNA sequence [54, 55]. It should be described into more details that the anti-aging gene Sirtuin 1 has been shown to be involved in ovarian function and OHSS. Then, this is critical to epigenetic alterations in obesity, and under hypoxia Sirtuin 1 regulates VEGF via HIF alpha. The use of Sirtuin 1 activators versus inhibitors may be critical to VEGF regulation and vasculature in OHSS and related diseases such as obesity. Diet, environment, stress and lifestyle factors literally alter Sirtuin 1 which affects the pathophysiology of OHSS and obesity [56-64]. Other predisposing factors include genetic factors, inadequate physical activity, socioeconomic status, excess caloric consumption, sleep deprivation, medical conditions like hypothyroidism and insolinoma, psychosocial stress and mental disorders [47, 48, 65, 66]. Furthermore, it would be such an interesting point that researchers categorized the genetic type into three groups: first, monogenic obesity which is caused by a mutation of a single gene that is involved in the leptin-melanocortin pathway that regulates energy homeostasis. In this type, the major characteristically feature is hyperplasia: secondly, polygenic obesity which results from the occurrence of multiple gene variants concurrently; third, syndromic obesity which is accompanying other signs of developmental diseases such as, Bardet-Biedel, MOMO, Cohen, and Prader will syndrome [53, 65, 67-69]. For management of genetic obesity, a combination treatment is required, including administering medicine, rectifying patients’ lifestyles, plus bariatric surgeries [53]. Scholars demonstrated that obesity particularly causes several adverse health consequences for human body. As a matter of fact, obesity promotes some undesirable outcomes attributed, in part, to type two diabetes mellitus, hypertension, sleep apnea, endometriosis, liver cirrhosis, dyslipidemia, PCOS, infertility, metabolic syndrome, arthritis, cardiovascular diseases, etc. [65-67, 70]. Evidence demonstrates that obesity is able to elevate the risk of some pregnancy-related complications, such as pregnancy loss, gestational hypertension, gestational diabetes, miscarriage, maternal death, and so on [71, 72]. Moreover, obesity, as a systemic inflammatory condition, adversely increases the risk of some types of cancers which are related to vascular dysfunctioning, including liver and gastrointestinal cancers [43, 48, 49, 55, 67]. As get informed, Obesity has been revealed as a metabolic state in which excess in storage of triglycerides in adipose tissues occurs gradually [50, 72].
1.2.1. Adipose tissue
Adipose tissue is distinguished as an endocrine organ [46, 49, 67]. It comprises of mixtures various adipocytes which are covered by stromal vascular cells, as well as fibroblasts and macrophages. These vasculature yields a condensed network of blood capillaries around the adipocytes [46, 67, 73]. Additionally, scholars recognized that there are different kinds of adipocytes in their functions despite of similar morphology. For instance, thermogenic adipocytes which conserve core body temperature. This kind of adipocyte exists around central organs. Some other examples include perivascular, mesenteric, and subcutaneous adipocytes. the latter instance is regarded as the largest depot and is capable of getting expanded as a reaction to excess food intake [73]. If we take a more totally look at adipose tissues, we realize that they comprise two types in human body; white adipose tissue (WAT), and brown adipose tissue (BAT). Researchers found out some different features between these two kinds. WAT is assigned for energy storage in the form of triglycerides. Moreover, WAT works as an endocrine organ, secreting some hormones such as gerlin and leptin, which are called adipokines. Nevertheless, BAT is specialized for thermogenesis in addition to energy expenditure due to mitochondria function which exist in this sort of adipocytes at high concentrated levels plus high density vasculature [41, 67, 74-76]. Overall, adipose tissue has the capability to get expanded by some triggering situations which include fasting and excess food intake. During the former condition, the body attains benefits from the adipose tissue expansion due to providing the ability to store fuels for using. The latter situation actually brings some drawbacks for the body so that causes obesity plus in turn its comorbidities [73]. The adipose tissue expansion can occur through two distinct mechanisms which consist of hypertrophic expansion (increase in size of adipocytes) and hyperplastic expansion (formation of new adipose cells) [67, 72, 75, 77]. Both of these mechanisms are able to happen in adults, specifically hypertrophy which sets out to get generated by excess caloric intake [73, 75]. During hypertrophy in adipose tissues, angiogenesis occurs because of overexpression of VEGF-A [67, 73].
1.2.1.1. VEGF-A Leads to Angiogenesis
As described above, overfeeding leads to hypertrophy of adipocytes eventually. The increase in size of adipocytes yields several negative impacts on the adipose tissues which include tissue hypoxia (55, 67, 75, 76). Indeed, adipose tissue dysfunctions contribute to adiposopathy for which there are two parts (anatomic & functional). For more explanation, the anatomic changes of adiposopathy are such as adipose tissue expansion and augmented levels of fat deposition in organs of the body. Nevertheless, functional changes include adipose tissue dysfunctions through endocrine and immunology responses, increased amounts of reactive oxygen species, tissue hypoxia, etc. [46, 77]. actually, some researchers state that these results especially adipocyte hypoxia might be because of either the compression effect of large adipocytes on vasculature by creating a niche or impairing capillary function through depressing capability of vessels to eliminate extracellular fatty acids. Furthermore, some other researchers hypothesized that the event of hypoxia in adults’ adipose tissues following adipocytes hypertrophy occurs due to the impacts of excess calories on both vasculature function and adipocytes [46, 73, 78]. Anyway, after generating tissue hypoxia in which the tissue receives inadequate blood flow, in turn the adipose tissue function gets disrupted and here is an alarm for the body, since hypoxia finally can lead to endothelial cells death. Therefore, the endothelial cells begin to overexpression of cytokines and angiogenic factors such as VEGF-A [32, 73, 79]. It should be emphasized that the VEGF-A is able to yield both angiogenesis and anti-angiogenesis on the capillaries [41, 73]. This against effect on endothelial cells comes from conversed effects of receptors on the cells. As a matter of fact, when VEGF-A locates on VEGFR 1, the anti-angiogenic property starts to happen. Nevertheless, when VEGFR 2 gets activated by VEGF-A, it shows angiogenic features [33, 34, 41]. As hypoxia is one of the stimulators of endothelial cells due to capillary rarefaction, the aim of releasing high amounts of VEGF-A would consequences angiogenesis in order to take the adequate blood flow to the tissue [32, 46, 76, 78]. For more explanation, VEGF-A sits on VEGFR 2 on endothelial cell wall. The mentioned receptor gets phosphorylated and is activated to generate intra cellular signaling such as PLC (phosphoinositide phospholipase C)- dependent pathway. This pathway consists of two mechanisms, including NOS-dependent signaling and mitogen-activated protein kinase (MAPK) cascade that both of them Finally, induce gene expression, mitogenesis, cell proliferation, and cell survival, thereby angiogenesis [32, 34, 80]. To clarify, VEGFR-2 activated leads tyrosine phosphorylation of PLCγ1 for which the activity of Src- family kinases are the requirements. phosphorylated PLCγ1 aggregates the level of inositol triphosphate (IP3) plus Ca2+ inside the endothelial cells which in turn leads to increased production of NO. Additionally, phosphorylated PLCγ1 activates MAPK cascades. Both NOS and MAPK cascade result in endothelial cells proliferation (32, 34). Then the basement membrane of the capillaries gets cleaved, allowing proliferated endothelial cells to incur into the adipose tissue stroma and make a lumen by endothelial cells migration. The following results include arranging extended blood capillaries which makes a dense network of vasculature in the adipose tissue [33, 67, 78].
We reviewed the two varied impacts of VEGF-A on blood vessels during two distinct situations; OHSS is one of the important IVF complications; leads to secretion of some mediators like VEGF, cytokines, renin-angiotensin system substances, etc. Among these vasoactive mediators, VEGF is considered as the main factor resulting in vascular permeability increase. In order to achieve this goal, VEGF-A binds to its receptor. Then, VEGFR2 activation generates a cell signaling which includes AJ protein phosphorylation. Since AJ stability underlies tight endothelial cell junction, the vascular barrier breakdown occurs due to phosphorylation of AJ proteins. Therefore, vascular permeability increases and intravascular fluid simply shifts into third space. On the other hand, during obesity something different occurs by VEGF-A; obesity prevalence has been increased during recent years due to environmental, genetic factors and so on. Due to adipose tissue expansion, tissue hypoxia occurs thereby cytokines and angiogenic factors such as VEGF-A release in order to repair capillary rarefaction. During this process, VEGF-A locate on VEGFR2, thereby activates NOS-dependent signaling and MAPK cascade by phosphorylation of PLCγ1. This event results in endothelial proliferation which then migrate and create denser network of capillaries in adipose tissue.
This research received no external funding.
The authors declare no conflict of interest.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
