AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Aamir Jalal Al Mosawi, Advisor in Pediatrics and Pediatric Psychiatry, Headquarter of Copernicus Scientists International Panel Baghdad, Iraq.
Citation: Aamir Jalal A M. (2021). The case number 506 of Mostyn Embrey syndrome: Imaging studies and ethics of naming syndromes. Biomedical Research and Clinical Reviews. 4(5); DOI: 10.31579/2692-9406/077
Copyright: ©2021 Aamir Jalal Al Mosawi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 July 2021 | Accepted: 26 August 2021 | Published: 03 September 2021
Keywords: mostyn embrey syndromes; iraq; imaging studies; hysterosalpingography; ultrasound; MRI
Background: Mostyn Embrey syndrome is a rare disorder associated with unilateral renal agenesis and malformations of the female reproductive tract. Delayed diagnosis is associated with serious diagnostic difficulties that may lead to inappropriate management including harmful surgery. The aim of this paper is to present imaging studies of case number 506 of the syndrome which was the first case of this rare syndrome in Iraq, and was originally reported in 2016. Ethics of naming syndromes relevant to this syndrome is discussed.
Patients and methods: An 18-year-old female presented with acute abdominal pain and poor urine output associated with retention of urine; about three years after the onset of menses. The pain was radiating to the back and pelvis. Her menstrual cycles started at the age of fifteen, and were lasting seven days. Cycles were associated with normal flow. The first physician the patient consulted considered the diagnosis of uterine tumor and the need for hysterectomy, but the family of the patient consultedanother physician. Vaginal exam was performed and showed bulging left vaginal wall. The diagnosis of hematocolpos was made. A clotted blood was drained by trans- vaginal approach.
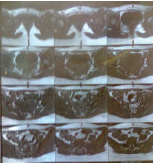
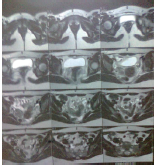
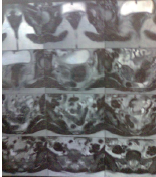
Results: It was difficult to identify the two separate uteri and two separate cervices and to make a diagnosis of didelphys uterus on hysterosalpingography. Abdominal MRI showed left renal agenesis, and two uterine bodies, cervices, and vaginas with normal myometrium and endometrium (uterine didelphys), and normal ovaries.
Conclusions: It is recommended that pediatricians, and pediatric nephrologists need to be aware of this syndrome to avoid unexpected presentations which may lead to delayed diagnosis and sometimes to inappropriate management. The imaging modalities that can be used to diagnose Mostyn Embrey syndrome include ultrasonography, hysterosal pingography and MRI. In this case, hysterosal pingography was not of much help. Ultrasound is affordable, non-invasive, widely available imaging modality that contributes to the accurate diagnosis of Mostyn Embrey syndrome. However, there can be difficulties in visualizing the vaginal septum on ultrasound which best shown on MRI. MRI can facilitate early diagnosis and thus help in the prevention of further complications. Syndromes in medicine are often named after the physician or group of physicians that discovered them or initially provided the full clinical picture or the best description of the syndrome. Unfortunately, Mostyn Embrey syndromes has been attributed unfairly and inappropriately to physicians other that those first described them in almost all previous papers.
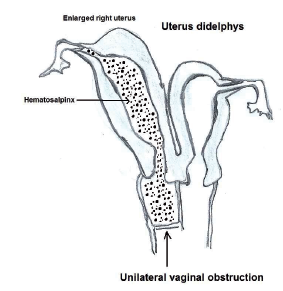
Mostyn Embrey syndrome is a very rare syndrome essentially consisting of the triad of: 1-Duplication abnormalities of the female reproductive tract (uterus, cervix, and vagina). Uterine abnormalities commonly didelphys and bicornuate uterus or unicornuate.
Duplication malformations of uterus and vagina are caused either by absence or incomplete fusion of the paired Müller's ducts. Uterus didelphys which is the most common uterine abnormalities associated with this syndrome. Uterus didelphys is associated with total duplication of the uterus with two independent horns, two cervices, and a double vagina.
The classic Mostyn Embrey syndrome is associated with uterus didelphys. Patients who have uterine abnormalities other than didelphys uterus are generally considered to have a variant of the syndrome.
2-Hemi-vaginal obstruction resulting in unilateral hematocolpos and usually resulting in some degree of hematometra and hemato-salpinxcaused by the back flow of retained menses in the site of the hematocolpos. However, variants of the classic syndrome may be associated with cervical obstruction or atresia.
3-Ipsilateral renal agenesis. Atypical variants can be associated with contra-lateral renal agenesis or other renal anomalies.The uterus, fallopian tubes, cervix and upper two thirds of the vagina develop from the paired müllerian ducts while the lower third of the vagina develops separately from the urogenital sinus.
Duplication of the female reproductive tract results from a lack of fusion of the paired müllerian ducts which appear at the sixth week of embryonic development. The müllerian ducts develop just lateral to the mesonephric (urinary) ducts, which have been hypothesized to act as a guide to the growth of the müllerian ducts. As they move caudally, the müllerian ducts cross over the mesonephric ducts ventrally and fusion of the lowermost portion occurs. The cranial non-fused portions form the paired fallopian tubes; the caudal fused ducts form the uterus, cervix, and the upper three-quarters of the vagina. The distal vagina is formed by invagination of the urogenital sinus whose endoderm then replaces the entire original vaginal epithelium. The association of duplication abnormalities of the uterus with obstructed hemi-vagina and renal agenesis ipsilateral to the side of obstruction was explained by embryologic arrest at the eighth week of gestation which simultaneously affects the müllerian and metanephric ducts. Other renal anomalies may also be associated particularly renal dysplasia, double collecting system and ectopic ureter [1, 2, 3, 4].
The aim of this paper is to present imaging studies of case number 506 of the syndrome which was the first case of this rare syndrome in Iraq, and was originally reported in 2016 [2]. Ethics of naming syndromes relevant to this syndrome is discussed.
Thirty four year old female who was born in 1981 presented initially at the age of 18 years (January, 31, 1999), about three years after the onset of menses with acute abdominal pain and poor urine output associated with retention of urine. The pain was radiating to the back and pelvis.
The first gynecologist the patient consulted considered the diagnosis of uterine tumor and the need for hysterectomy, but the family of the patient consulted another gynecologist. Later, vaginal exam was performed and showed bulging left vaginal wall. The diagnosis of hematocolpos was made. A clotted blood was drained by trans-vaginal approach.
It was difficult to identify the two separate uteri and two separate cervices and to make a diagnosis of didelphys uterus on hysterosalpingography (Figure-1).
As early as 1977, Brezina emphasized the possibility of not diagnosing Mostyn Embrey syndrome for many years after menarche even by hysterosalpingography. Abdominal MRI showed double uterus and left renal agenesis. MRI (Figure-2) performed at the 25th of September, 2005 showed two uterine bodies, cervices, and vaginas with normal myometrium and endometrium (uterine didelphys), and normal ovaries.
Her menstrual cycles started at the age of fifteen, and were lasting seven days. Cycles were associated with normal flow. However, she was frequently experiencing dysmenorrhea. During school she was less tolerant to sport activities and was frequently developing palpitation, shortness of breath and hypotensive episodes. Echocardiography showed mild mitral prolapse. However, her performance in school was good and she graduated from the college of dentistry at the age of 23 years during the year 2004.
She had also myopia (-3) and also dental abnormalities including spacing of teeth, and absence of the upper third molars, and malposition of the lower third molars. She developed dry socket infections of the lower third molars and their positions were corrected thereafter. During the years 2009 and 2010 she was complaining frequently from generalized aches and join pain. Radiographs taken during the 17th of October showed minimal degenerative changes at the knees and cervical spine radiographs showed spondylotic changes at multiple disc space.






The cervical rib couldn’t be seen and bone density was normal. She got married shortly after graduation from college. She became pregnant twice during the ten years following marriage.
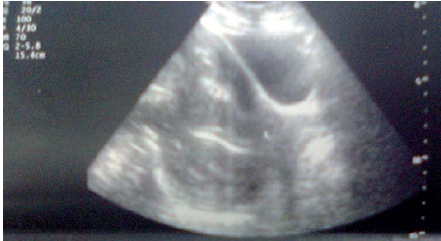
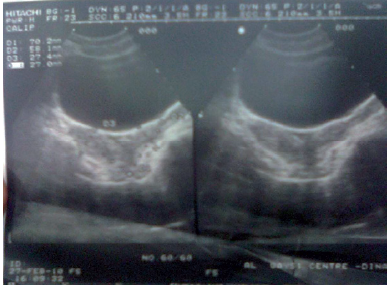
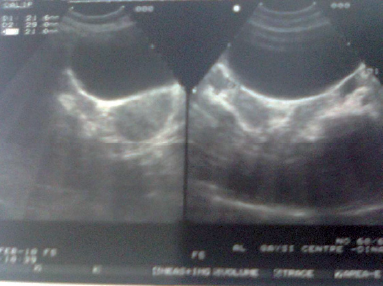
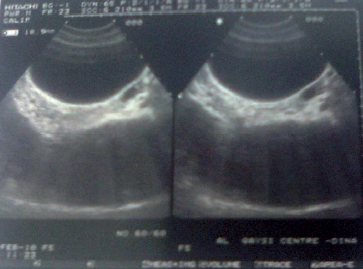
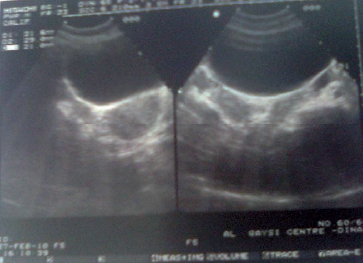
The first pregnancy occurred after about one year, but she experienced abortion. Figure-3 shows the ultrasound during pregnancy at the 16th of December 2004 before the abortion at about 20 weeks gestation. The ultrasound showed single viable fetus that was actively moving. She was evaluated twice with ultrasound early during the year 2010 (Figure-4, 5) more than two years before the second pregnancy.
Figure-5 shows ultrasound taken at the 27th of February, 2010. It showed didelphic uterus: The size of the right corn 70 X 27.4 mm with endometrial thickness of 7 mm. The size of the left corn 58.1 X 27 mm with endometrial thickness of 6.6 mm. Homogenous myometrial texture. The size of the right ovary was 34.9 X 20.5mm. The size of the left was 37.8 X 19.1mm ovary.



She became pregnant again during the year 2012. Ultrasound at the 6th of September 2012 (Figure-6) showed bulky gravid bicornuate uterus with well-defined gestational sac with in the right horn (19 X 13 mm). A tiny fetal pole was seen within the yolk sac.
She experienced elevation of blood pressure during pregnancy (BP 160/100) in association with edema, but without proteinuria. During her second pregnancy she experienced premature contractions and received medications including:
Aspirin 75 mg tablet once daily.
Duphaston 10 mg tablet three times daily.
Cyclogest 200mg suppository one daily.
Duvadilan .10 mg tablet twice daily.
Placental calcification grade 3 was detectable by ultrasound during pregnancy .She was delivered by Caesarian section at 36 weeks. The daughter was considered normal and imaging studies excluded Mostyn Embrey syndrome.
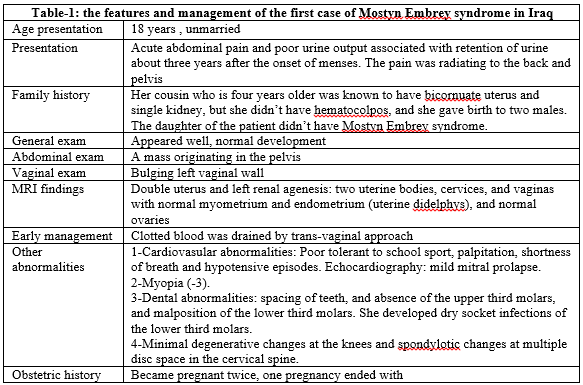
Her parents were unrelated. She has two brothers; one brother has two healthy male children and the other brother has a daughter with cricopharyngeal achalasia. Her mother and two brothers had history of renal stone. Her cousin who is four years older was known to have bicornuate uterus and single kidney, but she didn’t have hematocolpos, and she gave birth to two males. Table-1 summarizes the features and management of the first case of Mostyn Embrey syndrome.


The rare association of complete duplication of the genital tract-uterus didelphys; complicated by unilateral atresia with menstrual retention and a hematocolpo-metrosalpinx was probably first reported in the literature during 1922. Hadden [5] and Purslow [6] were probably the first to report this rare association. Purslow in 1922 reported a 16-year-old girl who had double uterus with right hematocolpos, hematometra and hematosalpinx [6]. Purslow treated patient by removal of the affected uterus and appendages (right hemi-hysterectomy) and vaginal septum incision with vaginal drainage [6]. Wilson reported in 1925 the treatment of a 14 years old girl who had double uterus and vagina with unilateral hematocolpos and hematometra who presented with pelvic mass and treated by total hysterectomy and salpingoophorectomy [7]. Brown and Brews reviewed 50 cases of congenital retention of the menses including a case of a 16 years old girl who had an abdominal mass. Laparotomy and excision of the hymen were performed, but the patient died eight days postoperatively because of peritonitis [8]. Simon HE [Surg Gynec Obstet 1928; 47:356] reviewed 23 cases of hematometra including a patient with an incomplete uterus didelphys." He also quoted Quenu and Le Sourd (1926) as reviewing eight cases of uterus didelphys with hematometra [4]. Masson and Mueller in 1933 reported a patient with uterus duplex bicornis with septate vagina open only on one side associated with right hematocolpos; they performed laparotomy and excision of the vaginal septum [9]. During the same year Carnington and Burlington reported a patient who had incomplete bipartite uterus with left hematocolpos and salpingitis. They treated the patient by partial hysterectomy and salpingoophorectomy [10]. In 1935, Martindale reported a case of uterus didelphys associated with hematocolpos of the right vagina and simulating appendicitis. The patient was treated by excision of the vaginal septum [11].
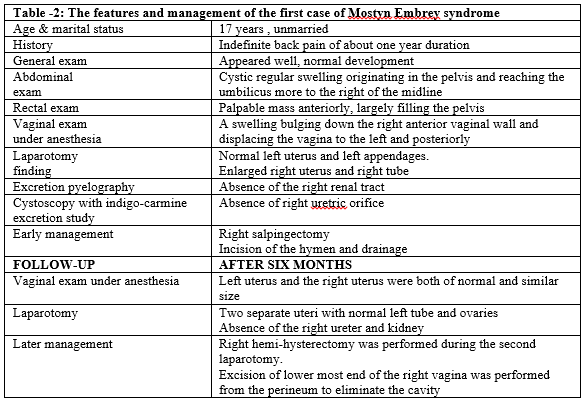
In 1950, Mostyn P. Embrey provided the first excellent description of the occurrence of uterus didelphys, hemi-vaginal obstruction in association with ipsilateral renal agenesis in an unmarried 17-year old girl referred to hospital because of abdominal swelling (Figure-7).Mostyn P. Embrey (B.Sc., M.D. F.R.C.S., and M.R.C.O.G.) was a lecturer in obstetrics at the University of Bristol and Assistant Obstetrician, Bristol Royal Hospital [1, 2, 3, 4].
It was not clear whether the earlier seven cases of the association of uterine duplication abnormalities commonly didelphys or bicornuate uterus with hemi-vaginal obstruction resulting in unilateral hematocolpos or hematocolpo-metrosalpinx reported during the period from 1922 to 1935 were associated with renal agenesis or not [Hadden (1922), Purslow (1922), Wilson (1925), Brown and Brews (1930), Masson and Mueller (1933), Carnington and Burlington (1933), and Martindale (1935)].
The patient described by Embrey was only complaining of indefinite back pain of about one year and she looked to be well and normally developed.
Abdominal examination showed a cystic regular swelling originating in the pelvis and reaching the umbilicus more to the right of the midline. Rectal examination revealed a mass which was palpable anteriorly largely filling the pelvis.
When the patient was examined digitally under anesthesia, the vulva was normal with intact hymen, but the abdominal mass was bulging down the right anterior vaginal wall and displacing the vagina to the left and posteriorly.
Laparotomy revealed a large rounded smooth mass, mostly extra-peritoneal and it was filling most of the pelvic cavity reaching the umbilicus and presenting in the laparotomy wound. The mass was alsocausing distention of the vagina to a large extent. On the top of the massthere was a uterus on each side. The left uterus was of average size andthe left appendages were normal. The right uterus was softer and enlargedto one and half the size of the left uterus and the right tube was 3 timeslarger because of hematosalpinx.
Right salpingectomy was performed and the right ovary was conserved. Incision of the swelling bulging from the vagina was made and about one liter of blood was drained. Right renal agenesis was confirmed by excretion pyelography which showed only the left renal tract. There was no right uretric orifice on cystoscopy with indigo-carmine excretionstudy.
After six months, exam under anesthesia showed that the left uterus and the right uterus were both of normal and similar size. The right vagina opened at the lower end of the left. A second laparotomy showed two separate uteri with normal left tube and ovaries. The absence of the right ureter and kidney was also confirmed. Right hemi-hysterectomy was performed during the second laparotomy. Excision of lower most end of the right vagina was performed from the perineum to eliminate the cavity. Convalescence was uneventful [1, 2, 3, 4]. Table-2 summarizes the features and management of the first case of Mostyn Embrey syndrome.
During the period from 1950 to 1970, sixteen cases were described in English literature including the first case of Mostyn P. Embrey [1]. Most of the cases were classical Mostyn Embrey syndrome: Woolf and Allen (1953) [four cases], Semmens (1956), Gibberd (1957), Hill (1958), Allan and Cowan (1963) [Three cases], Thompson and Lynn (1966) [Two cases], Lewis and Brent (1966) [2, 3, 4].
In 1971, Herlyn and Werner reported the 17th case of Mostyn Embrey syndrome and the first case in German literature. Unfortunately, they missed the earlier sixteen cases reported in English literature and considered their case inappropriately as a new typical syndrome of anomalies [1, 2, 3, 4].
A total of 41 cases of Mostyn Embrey syndrome were reported by the end of the 1970s.Thirty three cases had the classical syndrome with didelphys uterus and eight cases had atypical variant associated with bicornuate uterus in seven and unicornuate uterus in one patient.
Thirty six cases were reported during the 1980s, in addition to the atypical case reported by Burbige and Hensle who had severe renal dysplasia rather than renal agenesis [2, 4].
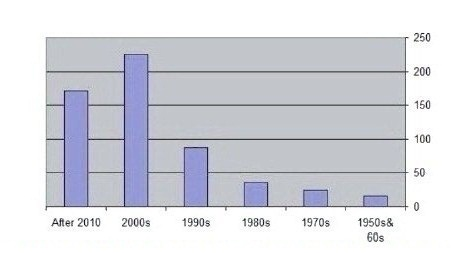
By the end of 1999, Eighty seven cases were reported including the atypical variant associated with hypoplastic cervix reported by Lee et al. The total cases of Mostyn Embrey syndrome reached 164. The 1990s witnessed the report of large series; from USA (15 patients) and from Italy (36 patients). During the 2000s, 225 cases with Mostyn Embrey syndrome were reported (The atypical case of Altchek and colleagues report was notincluded). There were reports from Israel, Finland, Tunisia, Italy, India, and USA. The total cases reported by the end of 2010 were 290 cases. After 2010, 171 cases with Mostyn Embrey syndrome were reported. The atypical cases including Garge et al variants and the patients with incomplete syndrome reported by Dorais et al. we’re not included in this count. The total cases reported after 2010 were 560 cases [2, 4].
Figure 8 shows the number of cases reported during the previous 100 years.
The vast majority of cases of Mostyn Embrey syndrome have been reported in English literature. However, some cases have been reported in other languages including eight in German, five in Bulgarian, three in French, three cases in Spanish, one in Danish, one in Dutch, and one case published in both English and Turkish.
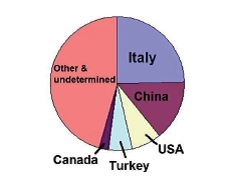
It was difficult and not convenient to determine the geographic region of many reports. However, there were 139 cases from Italy, 80 from china, 41 cases from the USA, 31 cases from Turkey, 13 from Canada, 9 from Japan, 7 from Taiwan, 7 from India, 6 from France, 5 from Bulgaria. 5 from Tunisia, 4 from UK (Many of the cases reported during the 1950s and 1960s are expected to be from UK), 4 from Australia, 4 from Finland, 4 from Israel, 2 from Spain, 2 from Singapore. There were also cases reported from Korea, Denmark, Poland, Portugal, Austria, Thailand, Netherlands, and Oman [2, 4]. Figure-9 shows the geographic distribution of cases of Mostyn Embrey syndrome reported during the previous 100 years.
The first case of Mostyn Embrey syndrome is Iraq was the case number 561, and the second in Ethnic Arab [2].
Atypical variant of the syndrome associated with bicornuate uterus rather than didelphys uterus were reported by Thompson and Lynn (1966) and Burton (1968). Although it was expected that many of the cases reported before 1970 were from the United Kingdom [2, 3, 4].
Non classical forms of Mostyn Embrey syndrome associated with bicornuate uterus rather than didelphys uterus have already been described before Wunderlich (1976) [13] by Thompson and Lynn (1966) , Burton (1968), and Amon and colleagues (1972). Therefore these atypical cases can be called Thompson Lynn variant of Mostyn Embrey syndrome [2, 4].
Another five atypical cases (variant) of the Mostyn Embrey syndrome associated with bicornuate uterus rather than didelphys uterus were reported by Brezina in 1977, Gazárek et al in 1979 [two cases],and Shenker and Brickman in 1979 [two cases]. Therefore, the total cases of Thompson Lynn variant of Mostyn Embrey syndrome were nine by the end of the 1970s [2, 4].
In 1972, Vinstein and Franken reported the first atypical case (variant) of Mostyn Embrey syndrome associated with septate uterus rather didelphys uterus. Hörr in 1979 described for the first time the occurrence of the syndrome in two sisters. Shenker and Brickman were probably the first to report pregnancy in a patient with Mostyn Embrey syndrome in 1979 [2, 4].
The most common clinical manifestation is dysmenorrhea, pelvic pain, vaginal or pelvic mass after menarche. Early diagnosis is important, to preserve fertility, and adhesion due to retrograde menstruation, hematometra, hematosalpinx and endometriosis which lead to distorted pelvic anatomy. These anomalies could be diagnosed with ultrasonography and magnetic resonance imaging. Resection or incision of vaginal septum is adequate treatments to relieve symptoms and reserve fertility in classic Mostyn Embrey syndrome.
Mostyn Embrey syndrome should be considered in the differential diagnoses in young females with unilateral renal agenesis presenting with pelvic mass, symptoms of acute abdomen, and acute urinary retention [1, 2, 3, 4].
A syndrome is a collection of medical signs and symptoms that are associated with each other and, often, with a specific disease or disorder. Syndromes in medicine are often named after the physician or group of physicians that discovered them or initially provided the full clinical picture or the best description of the syndrome. However, many of the rare syndromes have been described by physicians in many areas of the world before the era of the internet which has been associated with easy access to clinical reports throughout the world. Unfortunately, some syndromes have been attributed unfairly and inappropriately to physicians other that those first described them [2, 4].
Mostyn P. Embrey was the first to report the association of uterus didelphys, hemi-vaginal obstruction in association with ipsilateral renal agenesis. During the period from 1950 to 1970, sixteen cases were described in English literature including the first case of Mostyn P. Embrey. Most of the cases were classical Mostyn Embrey syndrome: Woolf and Allen [four cases], Semmens, Gibberd, Hill, Allan and Cowan [Three cases], Thompson and Lynn [Two cases] and Lewis and Brent. Atypical cases (variants) of the syndrome associated with bicornuate uterus rather than didelphys uterus were reported by Thompson and Lynn in 1966 and Burton in 1968 respectively. In April 1971, Herlyn and Werner reported the 17th case of the syndrome and the first in German literature. Unfortunately, they missed the earlier cases reported in English literature and considered their case as a new typical syndrome of anomalies Wunderlich M reported the thirty first case of the syndrome in 1976; the case was the third in German literature . It is intriguing and disturbing to discover the following facts about the historic reporting of Mostyn Embrey syndrome: Herlyn and Werner reported the 17th case of the syndrome twenty-one years after the first excellent description of the syndrome by Mostyn P. Embrey. Wunderlich M reported the thirty first case of the syndrome more than twenty-five years after the report of Mostyn P. Embrey [1, 2, 3, 4].
Gazárek et al. reported in 1979 four cases of Mostyn Embrey syndrome. They described them as having “duplication of uterus, para-cervically localized cystic resistance and renal aplasia on the same side”. It is very surprising that Gazárek et al. considered their cases to have two different syndromes; the Herlyn-Werner syndrome in two cases and the Wunderlich syndrome in the other two despite all apparent similarity of the four cases.
The patient of Wunderlich was described as having bicornuate uterus with simple vagina and isolated hematocervix on right without connection of the right uterus to the vagina in association with aplasia of the right kidney and ureter. Non classical forms of Mostyn Embrey syndrome associated with bicornuate uterus rather than didelphys uterus have already been described before Wunderlich by Thompson and Lynn, Burton, Amon and colleagues.
Obviously, the occurrence of bicornuate uterus in two of the four patients of Gazárek et al. and their unawareness of all the previously reported cases led them to their inaccurate description of the well-known syndrome [2, 4].
The classical uterine abnormality in Mostyn Embrey syndrome is didelphys uterus which is sometimes described as duplicated or double uterus. However, other uterine abnormalities especially bicornuate uterus and septate have been associated and such cases can be considered a variant of the classical syndrome. Such variants have been reported by many authors including Rock and Jones, Stassart et al. and Candiani et al., Heinonen Gholoum et al., Smith and Laufer and Vercellini et al. [2, 4].
There is only one reports of the familial occurrence of Mostyn Embrey syndrome in two sisters [2, 4]. In this Iraqi case a cousin of the patient have an incomplete variant of the syndrome. Such familial occurrence of the syndrome has not been reported before.
However, incomplete variants of the syndrome exist including the cases reported Fried et al. Their cases had bicornuate uterus or unicornuate uterus and unilateral renal agenesis but without hemi-vaginal obstruction and hematocolpos [2, 4]. Acute retention of urine as the initial clinical presentation has been rarely reported in this syndrome. This case is the seventh case of Mostyn Embrey syndrome presenting with retention of urine.
Strong suspicion and knowledge of this syndrome are mandatory for an accurate diagnosis. In fact, accurate diagnosis and surgical treatment can be delayed for several months or even years.
The treatment of patients with classical Mostyn syndrome is generally simple vaginal excision of obstructive septum. The imaging modalities that can be used to diagnose Mostyn Embrey syndrome include ultrasonography, hysterosalpingography and MRI. In this case, hysterosalpingography was not of much help. In fact, Brezina when reporting a case in 1977 emphasized the possibility of not diagnosing Mostyn Embrey syndrome for many years after the menarche even by hysterosalpingography.
Ultrasound is affordable, non-invasive, widely available imaging modality that contributes to the accurate diagnosis of Mostyn Embrey syndrome. However, there can be difficulties in visualizing the vaginal septum on ultrasound which best shown on MRI. MRI can facilitate early diagnosis and thus help in the prevention of further complications because MRI can show the müllerian duct anomaly complicated by obstructed hemi-vagina in detail and also the ipsilateral renal agenesis. Hollander and colleagues when reporting a case of the syndrome made a recommendation for pre-adolescent screening [2, 3, 4].
It is recommended that pediatricians, and pediatric nephrologists need to be aware of this syndrome to avoid unexpected presentations which may lead to delayed diagnosis and sometimes to inappropriate management. The imaging modalities that can be used to diagnose Mostyn Embrey syndrome include ultrasonography, hysterosalpingography and MRI. In this case, hysterosalpingography was not of much help. Ultrasound is affordable, non-invasive, widely available imaging modality that contributes to the accurate diagnosis of Mostyn Embrey syndrome. However, there can be difficulties in visualizing the vaginal septum on ultrasound which best shown on MRI. MRI can facilitate early diagnosis and thus help in the prevention of further complications. Syndromes in medicine are often named after the physician or group of physicians that discovered them or initially provided the full clinical picture or the best description of the syndrome. Unfortunately, Mostyn Embrey syndromes has been attributed unfairly and inappropriately to physicians other that those first described them in almost all previous papers.
The figures in this paper were previously included in some of the author’s publication, but he has their copyright.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
