AUCTORES
Globalize your Research

Case Report
*Corresponding Author: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, A-1, Ring Road, Rajouri Garden, New Delhi, India.
Citation: Anubha Bajaj. (2020) The Bairn’s Blain-Melanotic Neuroectodermal Tumour of Infancy. International Journal of Clinical Case Reports and Reviews. 3(2); DOI: 10.31579/2690-4861/033
Copyright: © 2020 Anubha Bajaj, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 July 2020 | Accepted: 07 August 2020 | Published: 11 August 2020
Keywords: Keywords
Abstract
Melanotic neuroectodermal tumour of infancy is an exceptional, benign, pigmented, melanin imbued neoplasm of neural crest origin, initially scripted by Krombecher in 1918[1]. The rapidly progressive neoplasm denominates a locally aggressive, biphasic tumefaction composed of miniature, primitive, round, neuroblast-like, blue cells admixed with enlarged, melanin- producing, epitheloid cells.The neoplasm is diversely nomenclated as melanotic progonoma, melanotic hamartoma, melanoameloblastoma, melanotic adamantinoma, congenital melanocarcinoma, retinal anlage tumour or pigmented congenital epulis Incriminated infants can depict elevated levels of urinary vanillylmandelic acid (VMA), thus implying a neural crest origin.
Disease Characteristics
Neural crest genesis of the neoplasm was hypothesized in 1966 on account of elevated urinary vanillylmandelic acid( VMA) secretion, as detected in adjunctive tumours of neural crest origin such as phaechromocytoma and neuroblastoma. Vanillylmandelic acid is restored to normal levels with surgical eradication of the neoplasm. Neural crest engenderment of the neoplasm can be determined by immune histochemical, ultrastructural and cell culture analysis. Also, biphasic cellular population comprised of melanocytic and primitive neuroectodermal cells appear as derivatives of neural crest [2, 3].On account of neural crest origin, gnathic bones are a frequent site of tumour incrimination. Majority (90%) of instances arise within cranio-facial sites and tumefaction is commonly discerned in maxilla (62.2%), skull (15%), mandible (7%), male reproductive system (5%), central nervous system (4%), soft tissues (1%) and female genital tract (<1%). Apart from head and neck, epididymis and testis are commonly incriminated besides exceptional implication of ovaries, soft tissues or bones of extremities [3]. Melanotic neuroectodermal tumour of infancy is typically discerned beneath < one year where majority (>90%) of incriminated subjects are infants. An estimated 50% of instances are beneath < 4.5 months. Median age of tumour discernment is 5 months. Congenital and prenatal cases are exemplified. A slight male predominance is observed.Although benign, melanotic neuroectodermal tumour of infancy can enhance rapidly and emerge as a locally infiltrative, destructive neoplasm with deformities ensuing in adjacent anatomic structures. Tumour reoccurrence is around 60%. Certain neoplasms undergo malignant metamorphoses wherein roughly 5% to 10% of tumefaction incur metastasis. Thus, preliminary tumour detection is mandated in order to minimize challenges and complications associated with treatment while inspiring a favourable outcome and normal developmental milestones [3, 4].
Characteristic genetic or molecular anomalies are absent in melanotic neuroectodermal tumour of infancy. The neoplasm is associated with BRAF-V600E mutation, germline heterogeneous mutation of CDKN2A with RPLP1-C19MC genetic fusion. Multiple tumour reoccurrences delineating a predominant neuroblastic component demonstrates loss of heterozygosity (LOH) with deletion of chromosome 1p and gain of chromosome 7q [3, 4].
Clinical Elucidation
Melanotic neuroectodermal tumour of infancy appears as a painless, expansive, lobulated, well circumscribed, un-encapsulated, firm, bluish- black, partially pigmented neoplasm with a superimposed intact epithelial surface. The tumefaction primarily arises within jaws of new born with frequent bone destruction and displacement of dental follicles. Appropriate discernment is contingent to pertinent clinical, radiographic and histological features although biphasic tumour composition is a crucial diagnostic element [3, 4].
Histological Elucidation
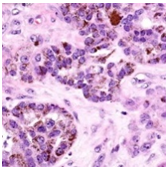
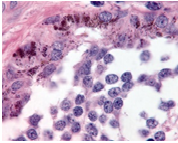
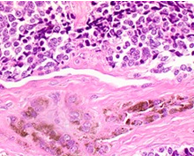
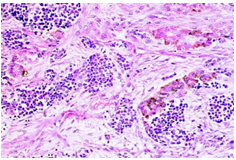
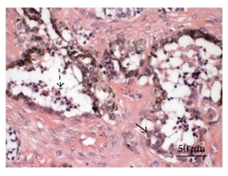
On gross examination, melanotic neuroectodermal tumour of infancy appears as greyish/ blue, firm, lobulated, well circumscribed tumefaction. Typically, tumefaction is superficially infiltrative and compresses abutting anatomic structures, instead of deep-seated tissue invasion. A blue- black hue is common on account of disseminated melanin. Cut surface is greyish to black contingent to quantity of melanin pigment [4, 5].Tumour nodules are comprised of neuroblast-like cells appearing as miniature, spherical, bluish, hyperchromatic cells with scant cytoplasm. Admixed are cords and nests of enlarged, epitheloid cells with abundant, pale cytoplasm, uniform, spheroidal nuclei and vesicular chromatin. The cytoplasm is impacted with melanin pigment although focal pigment granules can be identified. Tumour cells are disseminated within a dense, fibrotic background [4, 5].
Microscopically, melanotic neuroectodermal tumour of infancy is composed of islands of miniature, spherical neoplastic cells embedded amidst a fibro-collagenous stroma. Characteristic histological feature is a biphasic tumour cell population constituted of enlarged, epitheloid, melanogenic or melanin-producing cells and miniature, primitive, neurogenic or neuroblast-like cells. Tumour cells configure sheets, nests, cords, pseudo-glandular arrangements or occasional pseudo-alveolar spaces. The articulations are composed of an admixture of enlarged, melanogenic cells and miniature, neurogenic cells although ascribed cellular populations can appear singularly [5].Generally, melanogenic cells are delineated within the periphery whereas spheroidal neurogenic cells accumulate within centroidal region, configuring cellular nests or tumour aggregates.Melanogenic cells are moderate to enlarged, appear as epitheloid, polygonal or cuboidal, imbued with abundant eosinophilic cytoplasm and melanin granules. Nuclear chromatin is smooth to vesicular with occasional, prominent nucleoli [5, 6].Neurogenic population of tumour cells is comprised of miniature, primitive cells with minimal cytoplasm and elevated nuclear to cytoplasmic ratio. Nuclei are spherical, hyperchromatic and occasionally demonstrate salt and pepper chromatin. Neurofibrillary stroma enveloping neurogenic cells can be discerned in certain tumours. Tumour cells are intermixed with well vascularized, dense, fibro-collagenous stroma. Typically, mitosis and tumour necrosis are exceptional and accompany obviously malignant biological behaviour. Periphery of tumour aggregates localized within bone is infiltrative and nests of tumour cells are situated betwixt bony trabeculae. Tumour evolution with invasion of miniature neurogenic cells can be misinterpreted as a malignant neoplasm [5, 6]. As melanotic neuroectodermal tumour of infancy is composed of miniature, spheroidal, neuroblast- like tumour cells in combination with enlarged, polygonal, melanin- containing cells, it enunciates an amalgamation of neural, melanocytic and epithelial cells. Aforesaid heterogeneous cellular subtypes are incurred due to mesodermal and ectodermal morphological manifestations engendered by neural crest within diverse phases of ontogeny. M2- polarized macrophages contribute towards pathogenesis of neoplasm [6].


Immune Histochemical Elucidation
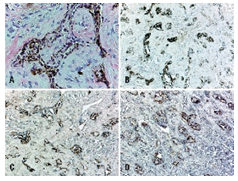
Miniature, round, primitive, neuroblast-like tumour cell component is immune reactive to synaptophysin, neuron specific enolase(NSE), glial fibrillary acidic protein (GFAP) and CD57. Enlarged, epitheloid, melanin-producing tumour cells are immune reactive to anti-cytokeratin monoclonal antibodies (AE1/AE3) and human melanoma black 45 (HMB45) antigen. Dendritic-like cells, immune reactive for HLA-DR, Factor XIIIa, CD68, CD163 can be observed within glia- like tissue, fibrous tissue septa and within tumour stroma. Aforesaid cells can be implicated in modulating tumour growth and/ or remodelling of intervening tumour stroma[6,7].
Immune markers such as human melanoma black 45 (HMB45) antigen, Melan A, cytokeratin along with neuroblastic markers as synaptophysin, neuron specific enolase (NSE) can assist in discerning the neoplasm. Melanin-producing epithelial cells are intensely immune reactive to HMB45 and Melan A [6, 7].Melanogenic and neurogenic cells comprising melanotic neuroectodermal tumour of infancy are immune reactive to vimentin and neuron specific enolase(NSE). Enlarged epitheloid, melanogenic cells are commonly reactive for cytokeratin and markers of melanocytic differentiation as human melanoma black 45 (HMB45) antigen and dopamine β-hydroxylase. Enlarged epitheloid cells are variably immune reactive for synaptophysin. A proportion of melanogenic cells are immune reactive to epithelial membrane antigen (EMA) [6, 7].Miniature neurogenic cells are immune reactive to synaptophysin and non-reactive for cytokeratin. Neuroblast- like cells can occasionally be immune reactive to glial fibrillary acidic protein (GFAP) although immune reactivity to neurofilament and CD99 is exceptional.Melanogenic and neurogenic cells are typically non-reactive to chromogranin and S100 protein with few instances delineating a focal expression.Foci of glial differentiation and varying stages of skeletal muscle can be enunciated in few instances with immune staining for myogenic markers such as desmin, muscle specific actin (MSA) or myogenin. Aforesaid immune reactivity can exemplify a misrepresentation as rhabdomyosarcoma[7,8].
Melanotic neuroectodermal tumour of infancy can express histological and immune phenotypic features akin to adjunctive lesions such as cellular blue nevus, malignant melanoma, neuroblastoma or rhabdomyosarcoma although diffuse reactivity with S100 protein is not exemplified.On ultrastructural examination, melanogenic cells are encompassed by basal lamina and configure desmosomes with adjacent cells whereas neurogenic cells depict dense vesicles [6, 8].
Differential Diagnosis
Melanotic neuroectodermal tumour of infancy arising in head and neck requires segregation from Ewing’s sarcoma, lymphoma, odontogenic tumours, developmental cysts, rhabdomyosarcoma, metastatic neuroblastoma, localized infection and non odontogenic lesions as fibromatosis or fibrous dysplasia [3].Melanotic neuroectodermal tumour of infancy mandates distinction from adjunctive childhood round cell tumours such as neuroblastoma, Ewing’s sarcoma, alveolar rhabdomyosarcoma or lymphoma. Also, melanogenic tumours such as malignant melanoma or clear cell sarcoma of soft tissue necessitate demarcation [3, 4].Distinctive features enunciated by melanotic neuroectodermal of infancy are cogent clinical representation, biphasic population of epitheloid, melanogenic cells admixed with primitive, neurogenic cells along with characteristic immune reactive panel.Evaluation of miniature tissue specimens can be challenging as the neoplasm can be misdiagnosed as a neuroblastoma[3,4].Olfactory neuroblastoma is frequently discerned within fifth to sixth decade. Typically, cribriform plate, nasal concha or septum is incriminated. Tumour cells are miniature, spheroidal, bluish and configure Homer-Wright rosettes, falsely imparting a biphasic cellular morphology although constituent cells are of singular subtype. Tumour cells are immune reactive to neuron specific enolase (NSE) and synaptophysin, akin to primitive neurogenic cells of melanotic neuroectodermal tumour of infancy. Also, neuroblastoma lacks a population of epitheloid melanogenic cells imbued with melanin pigment and is non-reactive to cytokeratin or HMB45[3,4].However, melanotic neuroectodermal tumour of infancy is typically devoid of rosette articulations and diffuse immune reactivity to neuroendocrine markers.An estimated 2% to 10% of Ewing’s sarcoma appear within head and neck. Ewing’s sarcoma is comprised of nests and sheets of miniature, monomorphic, spherical cells. Cellular component can recapitulate neuroblast- like cells of melanotic neuroectodermal tumour of infancy wherein enlarged, pigmented, epitheloid melanogenic cells are absent. Tumour cells depict an intense, diffuse, cytoplasmic immune reactivity to CD99. The neoplasm typically harbours chromosomal rearrangements of EWSR1 gene. Majority of Ewing’s sarcoma depict chromosomal translocation t(11;22)(q24;q12) with EWSR1-FLI chimeric fusion. Although melanotic neuroectodermal tumour of infancy can exceptionally react to CD99, absence of molecular signatures of Ewing’s sarcoma can be beneficially adopted for demarcating the neoplasms [3, 4].Alveolar rhabdomyosarcoma is commonly discerned within extremities although head and neck region is often incriminated. The neoplasm is constituted of nests of poorly differentiated, miniature, hyperchromatic cells subdivided by fibrous tissue septa. Tumour cells of alveolar rhabdomyosarcoma are focally immune reactive to desmin and display a diffuse, intense reactivity to myogenin. Characteristic chromosomal translocation t(12;13) or t(1;13) along with fusion of PAX-FOX01 gene is denominated. As melanotic neuroectodermal tumour of infancy can demonstrate focal muscular differentiation, molecular assay and fluorescent in situ hybridization (FISH) evaluation is advantageous for appropriate distinction [3, 4].Rhabdomyosarcoma is a neoplasm occurring in older individuals whereas embryonal rhabdomyoblastoma is a frequent subtype incriminating younger children. The neoplasm commonly implicates sinonasal tract and is composed of miniature, primitive, spherical, bluish cells intermingled within scattered rhabdomyoblasts. The neoplasm is immune reactive to myogenic markers such as myogenin or myoD1. Epitheloid, pigmented, melanogenic cellular component is usually absent [3, 4].Ewing’s sarcoma and alveolar rhabdomyosarcoma delineate extensive tumour necrosis, a feature typically absent in melanotic neuroectodermal tumour of infancy.Benign or malignant haemato-lymphoid cells can morphologically simulate neurogenic cells although an expression of haemato-lymphocytic markers is observed along with non-reactivity to epithelial or melanotic immune markers(3,4).Immune profile of melanotic neuroectodermal tumour of infancy is diverse from lymphoma. Also, the neoplasm is devoid of reoccurring molecular modifications. Thus, cogent molecular and cytogenetic analysis is beneficial in differentiating the neoplasms with characteristic chromosomal translocations accompanying haemato-lymphoid neoplasia[4].
Approximately 16% of non –Hodgkin’s lymphoma (NHLs) are discerned within jaw bones. An estimated two-thirds instances are diffuse large B cell lymphoma (DLBCL). Older age individuals are commonly implicated. Lymphoblastic lymphoma or Burkitt’s lymphoma predominantly demonstrate monotonous, miniature to medium- sized spherical cells in the absence of biphasic cell population. Flow cytometry, immune histochemical assay for terminal deoxynucleotidyl transferase (TdT) and molecular studies can assist tumour differentiation and classification.Malignant melanoma appearing in childhood delineates a distinctly malignant cellular morphology, is immune reactive to S100 protein or adjunctive, immune reactive melanoma markers and is non-reactive to cytokeratin[3,4].Classically, clear cell sarcoma occurs within extremities of young adults. The neoplasm is comprised of uniform, spindle-shaped to elliptical cells with clear to pale, eosinophilic cytoplasm. Primitive, neurogenic cells are absent. Clear cell sarcoma characteristically demonstrates reoccurring chromosomal translocation t(12;22)(q13;q12) with consequent emergence of EWS-ATF1 chimeric gene and an infrequent t(2;22)(q34;q12) genetic translocation[3,4].
Congenital granular cell tumour of new born (congenital epulis) emerges within a similar age group as melanotic neuroectodermal tumour of infancy. Nevertheless, characteristic histology aids distinction betwixt the entities[3].Odontogenic tumour of childhood can clinically simulate melanotic neuroectodermal tumour of infancy on account of identical tumour localization and representation, although the neoplasm is exceptional prior to 6 years[4].Desmoplastic small round cell tumour is an infrequent, aggressive neoplasm arising within abdomen of adolescents and young adults. A male preponderance is observed. Neoplasm is composed of nests of spheroidal, blue cells with variable cytoplasm, hyperchromatic nuclei and a circumscription of desmoplastic stroma. Epitheloid, melanogenic cellular component is usually absent. Chromosomal rearrangements of EWSR1 gene, akin to Ewing’s sarcoma, are discerned [3, 4].
Investigative Assay
Evaluation with computerized tomography (CT) is optimal for tumour discernment besides procuring information regarding appropriate surgical manoeuver. Intraosseous lesions commonly display a well circumscribed, hypodense tumefaction. Aggressive, advanced tumours are accompanied by extensive bone destruction. A well-defined, unilocular, osteolytic lesion is cogitated which expands and decimates incriminated cortical bone (7, 8). Imaging studies represent the tumour as a well demarcated, radiolucent, bony, lytic lesion with accompanying features of localized demolition of soft tissue, akin to a malignant neoplasm.Computerized tomography (CT) demonstrates a hyper-dense nodule with enhanced bone remodelling and expansion(7).Magnetic resonance imaging (MRI) reveals a circumscribed, expansive neoplasm appearing hypo-intense upon T1 and T2 weighted imaging.Generally, computerized tomography is adopted to define the neoplasm and evaluate appropriate surgical approach although magnetic resonance imaging is superior in illustrating the soft tissue component. Due to diverse imaging features described with melanotic neuroectodermal tumour of infancy, accrual of cogent tissue specimens is necessary for appropriate diagnosis (8).
Prognostic Outcomes Although benign, biologic behaviour of melanotic neuroectodermal tumour of infancy is inadequately inferenced. Rapid tumour progression and significant, localized tumour infiltration or relapse can be alarming. Localized tumour reoccurrence appears in an estimated 6.5% subjects although the proportion varies from 10% to >35% individuals. Tumour reoccurrence appears on account of multi-centric tumour growth or inadequate surgical extermination of the neoplasm with multiple surgical interventions. Fatality due to tumour reappearance is observed, especially with incrimination of central nervous system or vital organs [8, 9].
Malignant melanotic neuroectodermal tumour of infancy accounts for an estimated 6.5% instances and segregation betwixt benign and malignant neoplasm can be challenging as pertinent diagnostic criterion or immune markers are undefined. Cogent histological manifestations along with a mitotic index ≥ of 2 mitosis per 10 high power fields or Ki67 proliferation index exceeding >25% and immune reactive CD99 are associated with tumour aggression. Preponderant neuroblast -like cells with an insignificant component of enlarged, melanogenic cells also display aggressive behaviour and enhanced localized tumour reoccurrence. Preliminary age of disease discernment appears to be a prognostic indicator of tumour relapse. Tumours detected within 2 months of infant life can probably reappear within 6 months and are associated with reduced disease- free survival. Tumours detected within 4.5 months of infant life delineate an intermediate possibility of tumour reoccurrence. Melanotic neuroectodermal tumour of infancy is associated with tumour metastasis in an estimated 3% instances. Neoplastic dissemination occurs within lymph nodes and central nervous system [7, 9].
Therapeutic Options
Optimal therapy for melanotic neuroectodermal tumour of infancy is comprehensive surgical excision with removal of a broad, 5 millimetre perimeter of uninvolved tissue along with eradication of incriminated teeth [8, 9].Comprehensive, localized surgical eradication of the neoplasm with tumour- free surgical perimeter is preferred. Adjuvant therapy can be adopted for treating residual neoplasm or tumour reoccurrence.Singular chemotherapy or radiation therapy or combination of chemotherapy with surgical extermination of the lesion can be adopted. The lesion can be subjected to enucleation and curettage. Adopted therapeutic modality is contemplated as curative where the neoplasm can be severed from abutting bone. Thereby, inferior aesthetic outcomes and altered facial development can be circumvented [8, 9].Tumour reoccurrence is discerned within 6 months following treatment and generally appears in subjects below < 4.5 months. Due to rapid tumour enhancement observed with melanotic neuroectodermal tumour of infancy with consequent, possible major anatomic deformities within circumscribing tissues, antecedent diagnosis is anticipated in order to obtain superior functional and therapeutic outcomes with minimalistic mutilating surgeries[8,9].Chemotherapy and/ or radiation therapy is employed in around 9.6% instances, especially prior to surgical eradication, in order to decimate tumour magnitude and enable comprehensive tumour resection.Neoadjuvant therapy is applicable for inoperable tumours, incrimination of central nervous system and vital organs or where surgical perimeter is undefined and tumour-incriminated. Cogent chemotherapy can initiate maturation of primitive, neurogenic tumour cells, depletion of neuroblast-like cellular component and predominance of epitheloid, melanogenic component [8, 9].
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
