AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Mauro Alves, Netto Djaló. Hospital das Clínicas, Recife, PE, Brazil.
Citation: Mauro Alves, Nelson Albuquerque de Souza e Silva, Lucia Helena Alvares Salis, Bragança Pereira BD, Paulo H. Godoy, et al, (2023), Survival and Predictive Factors of Lethality in Hemodyalisis: D/I Polymorphism of The Angiotensin I-Converting Enzyme and of the Angiotensinogen M235T Genes, J, Surgical Case Reports and Images 6(6); DOI:10.31579/2690-1897/151
Copyright: © 2023, Mauro Alves. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 September 2023 | Accepted: 10 October 2023 | Published: 21 October 2023
Keywords: survival analysis; lethality; renal dialysis; polymorphism; genetic; peptidyl-dipeptidase a; kidney failure; chronic
Background: End-stage kidney disease patients continue to have markedly increased cardiovascular disease morbidity and mortality. Analysis of genetic factors connected with the renin–angiotensin system that influences the survival of the patients with end-stage kidney disease supports the ongoing search for improved outcomes.
Objective: To assess survival and its association with the polymorphism of renin-angiotensin system genes: angiotensin I-converting enzyme insertion/deletion and angiotensinogen M235T in patients undergoing hemodialysis.
Methods: Our study was designed to examine the role of renin-angiotensin system genes. It was an observational study. We analyzed 473 chronic hemodialysis patients in four dialysis units in the state of Rio de Janeiro. Survival rates were calculated by the Kaplan–Meier method and the differences between the curves were evaluated by Tarone–Ware, Peto-Prentice, and log rank tests. We also used logistic regression analysis and the multinomial model. A p value 0.05 was considered to be statistically significant. The local medical ethics committee gave their approval to this study.
Results: The mean age of patients was 45.8 years old. The overall survival rate was 48% at 11 years. The major causes of death were cardiovascular diseases (34%) and infections (15%). Logistic regression analysis found statistical significance for the following variables: age (p = 0.000038), TT angiotensinogen (p = 0.08261), and family income greater than five times the minimum wage (p = 0.03089), the latter being a protective factor.
Conclusions: The survival of hemodialysis patients is likely to be influenced by the TT of the angiotensinogen M235T gene. (Arq Bras Cardiol. 2014; [online].ahead print, PP.0-0)
The number of patients undergoing renal replacement therapy is on the increase all over the world, including Brazil1-3. Data from the Brazilian Society of Nephrology shows that between 1994 and 2009, the number of patients enrolled in chronic dialysis programs in Brazil more than tripled from 24,000, to 77,5893. Of these, 89.6% were on hemodialysis [3].
On July 1st, 2010, the number of Brazilian dialysis patients was 92,091. The annual crude mortality rate for patients with end-stage chronic kidney failure was 17.1% in 20093, and 17.9% in 2010 [4]. Despite major advances in recent decades in the treatment of chronic kidney disease,
cardiovascular disease is still the main cause of death for these patients, especially among those on dialysis. The cardiovascular mortality of hemodyalized patients is high (40% to 50% of the population of chronic kidney patients), significantly higher than for the general population5,6. The general population trend for cardiovascular mortality is decreasing, but, among hemodialyzed patients, it is increasing [4-8].
Traditional cardiovascular risk factors alone are not capable of explaining the high mortality rate for chronic kidney disease, dialysis population. Other factors need to be taken into consideration. Our view is that the key to improving survival is better knowledge of prognostic risk factors, be they traditional or not.
The primary objective of this study was to assess the survival of patients with end-stage chronic kidney failure who received hemodialysis in four centers in the State of Rio de Janeiro. patients were followed up for 11 years and compared to the general population to look at the correlation between mortality for those with cardiovascular risk factors and D/I and M235T polymorphisms of the angiotensin I-converting enzyme and the angiotensinogen genes, respectively. The secondary objective was to analyze cause of death by sex and age group.
Study Diagram:
Population of 4 HD centers (1997/98) -------- 11 years ------
• Death
• Survival on HD
• Transplanted
• Transferred
The initial study cohort comprised 473 chronic hemodialyzed patients from four hemodialysis centers. Three from the city of Niterói and one from Rio Bonito. This represented all eligible patients in those hemodialysis centers from July 15, 1997 to July 15, 1998.
Inclusion criteria: All adult patients (aged 18 years old or more at the time of selection for this study), regardless of age at the time hemodialysis treatment began, who had been on chronic hemodialysis for at least one year during the period between July 15, 1997 and July 15, 1998.
Exclusion criteria: Exclusion criteria included the presence of Acute Kidney Failure; refusal to participate in this study; and the fact that patients had already been submitted to kidney transplant before selection.
Death records: We used the Mortality Information System. Survival analysis used information from the study population data bases, and death records (1998 to 2008) in the State of Rio de Janeiro, with the objective of identifying individuals who passed away and to determine cause of death. Analysis was conducted with RecLink III software and consisted of six steps:
1. Standardizing the format of data variables.
2. Grouping records using identification keys.
3. Using algorithms to compare chains of characters.
4. Scoring record pairs on their level of global concordance.
5. Using threshold definitions to determine whether each pair was real, doubtful, borderline, or non-paired.
6. Manual revision of the doubtful or borderline pairs, aiming to reclassify as real pairs or non-pairs.
Study duration: Follow-up: 11 years; recruitment: July 15, 1997 to July 15, 1998; conclusion: December 31, 2008.
Variables: The variables studied were defined as follows:
1. Systolic Blood Pressure before the hemodialysis session: The first measurement recorded in the medical history was used in the recruiting stage of this study.
2. Length of hemodialysis in months at the time of recruiting. From this variable, it was possible to calculate the date hemodialysis started and the time of survival on hemodialysis. This was calculated by the sum of the time of hemodialysis at the beginning of the treatment, plus the time until the event (death, kidney transplant or conclusion of the study).
3. Body Mass Index. Calculated using the formula, weight in kg, divided by the squared height in meters. Weight was obtained prior to hemodialysis.
4. Monthly family income, as provided by the patient when he or she was admitted to the hemodialysis center. This information was registered in the medical record or it
was collected from the patient. The variable was measured in number of minimum wages at the time the treatment began in the hemodialysis center. Afterwards, we created the following categories: less than two times the minimum wage; from two to five times the minimum wage; and more than five times the minimum wage.
5. Age at the beginning of hemodialysis (in years).
6. Gender.
7. Basic cause of death: using data from the Mortality Information System of the State Secretariat of Health in the State of Rio de Janeiro, we identified the basic cause of death recorded in the Mortality Information System through selection rules.
8. Triglycerides: measured by the enzymathic method, at the time of recruiting.
9. Total cholesterol: measured by the enzymathic method, at the time of recruiting.
10. High-density lipoprotein: measured by the enzymathic method, at the time of recruiting.
11. Hematocrit: Percentage occupied by red blood cells in the total blood volume, at the time of recruiting.
12. Diabetes mellitus, diagnosis registered on the medical record at the time of admission in the hemodialysis center, and collected by us during recruiting.
13. History of ischemic heart disease, characterized by acute myocardial infarction, angina pectoris, or by some previous invasive coronary procedures. This information was collected from medical records.
14. History of stroke, collected from medical records.
15. History of smoking or former smoking, recorded in medical records at the time of admission to the hemodialysis center.
16. Polymorphism of genes of the angiotensin I-converting enzyme (I/D) and angiotensinogen (M235T). Samples of 5 mL of blood were drawn from patients at the time of recruiting and stored in tubes containing ethylenediaminetetraacetic acid, which were sent to São Paulo. The genetic polymorphism of the angiotensin I-converting enzyme (I/D) was determined by using a standardized essay with three primers. The variable M235T of the angiotensinogen gene was determined by the polymerase chain reaction method, followed by enzymatic digestion. The team who conducted the genotypic assessments did not have access to the clinical information of the study patients.
Patients who had undergone kidney transplant and patients who were alive on December 31, 2008, when the study was concluded, were censored to their respective dates.
The analyzed outcomes were: primary, time of survival; and secondary, basic cause of death.
The Research Ethics Committee in the University Hospital Clementino Fraga Filho, at Universidade Federal do Rio de Janeiro, approved this study.
Each variable was analyzed and its distribution, mean, and standard deviation was calculated. The Chi-Square test was used for categorical variables and the unpaired Student’s
t-test was used for quantitative variables (quantitative variables had normal distributions, as the sampling number was sufficiently large). A 5% significance level was adopted in both cases. The logistic regression model and the odds ratio calculation were used, as well as the multinomial logistic model, the Cox model, the classification and survival trees. The chosen variables were used as a base allowing a visual analysis of mortality and the variables associated with it.
Kaplan–Meier curves were used to visualize the survival of patients according to the chosen variable. The Tarone-Ware, Peto–Prentice and Log-Rank tests were used to assess the difference between curves. The statistical significance level adopted for curves was 5%. Analyses were conducted with R software. Survival curves were measured from the date estimated for the beginning of hemodialysis for each patient. The Hardy-Weinberg equilibrium was calculated. The statistics flowchart, shown in Figure 1 was used, and is described as follows:
1. Univariate exploratory data analyses.
2. Survival Kaplan–Meier curves with the study polymorphisms, comparing deaths caused by the circulatory system (the main cause of death) with other causes. To identify whether the differences found in the Kaplan–Meier curves were significant, we used the Tarone–Ware and the Peto–Prentice tests. We used the log rank test to compare survival curves, as it is the most widely used method. This is also known as the Mantel–Cox test, these tests are only different in the weights used.
3. Classification tree, with the objective of understanding which variables, or interaction of variables, are responsible for the analyzed phenomenon.
4. Survival tree, which was used for the same purpose as III.
5. Logistic regression was employed for all patients, taking death by any cause as the dependent variable and only selecting other variables that were clinically and/or statistically relevant.
6. Multinomial logistic model for all patients using all of the variables. The dependent variable at this point was death caused by atherothrombotic vascular disease (ischemic heart disease plus stroke), which was the biggest cause of death among diseases of the circulatory system. Multinomial models constitute an extension of logistic models, being used in cases in which the response variable is nominal, with more than two categories, as in this case.
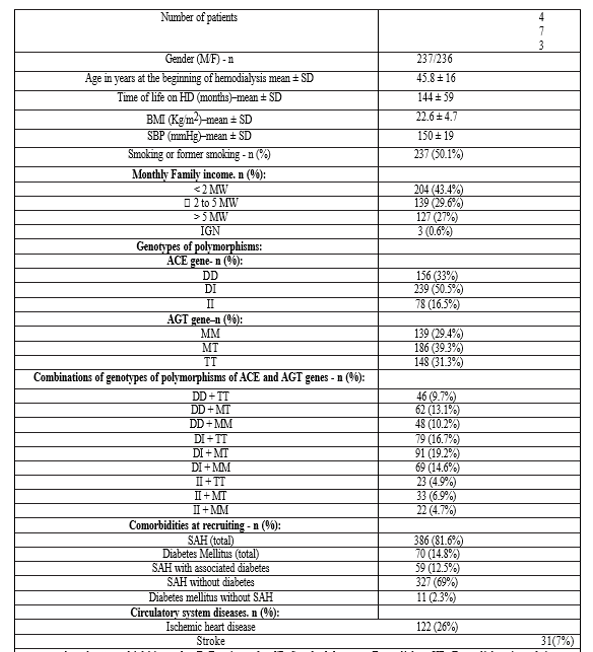
1) Clinical and demographic variables: Only one patient out of the 474 cases that met the selection criteria refused to participate in the study. Out of the 473 analyzed cases, 237 (50.1%) were male. The mean age at the beginning of hemodialysis was 46 years. The mean duration of hemodialysis (HD) at the time of recruiting was 52 months (4.4 years). The mean time of life on hemodialysis was of 144 months. The mean body mass index was > 30 kg/m2. Half of the population consisted of smokers or former smokers. Almost half of the cases (43.4%) had a monthly income of less than twice the minimum wage. The mean systolic blood pressure was 150 mmHg, and most cases (81.6%) were classified as hypertensive patients. Diabetes mellitus was present in 15% of the cases, and generally associated with hypertension. The DI genotype of the angiotensin I-converting enzyme (50%) and the MT genotype of the angiotensinogen (39.3%) were the most prevalent ones. Ischemic heart disease was present in 26% of the cases, and stroke in 7% (Table 1). With respect to biochemical and hematological data, we did not observe major changes from the normal rate for the variables studied, except for the low hematocrit mean (29%) (Table 2) (Figure 2).
2) Survival: The crude death rate at 11 years was 52%. There was a 48% survival rate at 11 years. The mean age at the time of death was 57 years old (± 15).
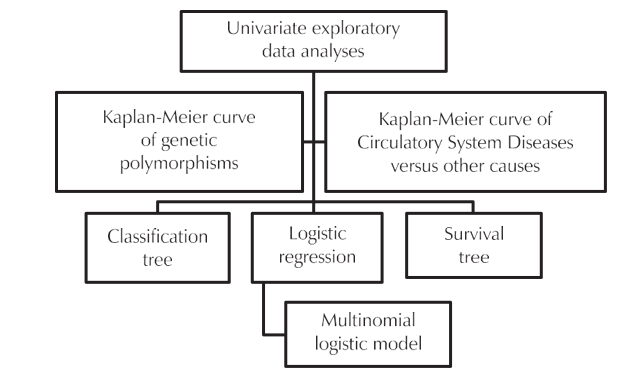
Figure 1: Diagram of the statistical analyses used
The Kaplan–Meier survival curve showed no differences between genetic polymorphisms of the gene in the converting enzyme (D/I) (Figure 3). We also built a Kaplan-Meier curve for polymorphism of the angiotensinogen. In this, we observed a tendency for the curve for the TT genotype to separate in relation to time of survival, even though the population was smaller (Figure 4). This trend was also confirmed when we separated the TT genotype of the angiotensinogen from the others in the Kaplan–Meier survival curve, with the Tarone-Ware test, and obtained a p value of 0.0976.
3) Probability of death and its association with the variables used in statistical models: The logistic regression model, using death by any cause as a dependent variable, found the following p values and odds ratios (OR) with 95% confidence intervals. Age (p value = 0.000038, OR = 1.027), angiotensinogen TT (in relation to MM) (p value = 0.08261, OR = 1.534) and monthly income greater than five times the minimum wage (a protective factor) (p value = 0.03089, OR = 0.600).
Using a multinomial logistic model for all patients and using all variables, with death caused by atherothrombotic vascular disease (ischemic heart disease plus stroke, the main cause of death in this cohort), as the dependent variable, we found the following variables to be statistically significant. Age (p = 0.019802), and TT polymorphism of the angiotensinogen (p = 0.001394). TT was significant for both for men (p = 0.039402) and women (p = 0.01518).
Because the study population at the time of recruiting had different periods of hemodialysis, and because it was not in Hardy–Weinberg equilibrium with regards to polymorphism of the angiotensinogen (p value < 0>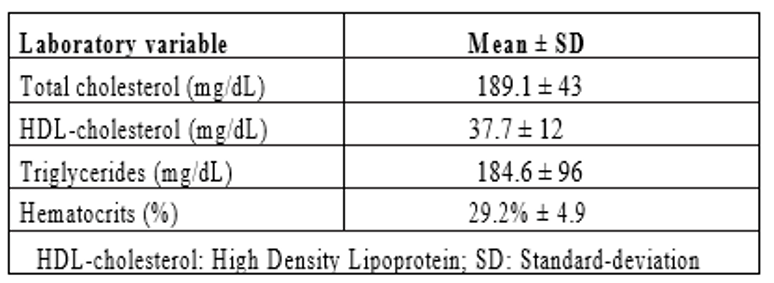
Table 2: Laboratory data (biochemical and hematologic) at recruitment (July 97/July 98) of patients on HD
In our study, there were very slightly more males (50.1%) than females, which is in accordance with 2008 Census from the Brazilian Society of Nephrology. It found that men make up 57% of the population with end-stage chronic kidney disease1. A study in Bahia found a 56.6% of patients to be male9. A cross-sectional analysis conducted in six hemodialysis clinics in the State of Rio de Janeiro also found a higher proportion of men (56%) [10].
The mean age of the study population was 46 years, which is lower than that found in a study in the State of Rio de Janeiro10 (54 years old), and also lower than another cross-sectional analysis conducted in a single dialysis center in the State of Rio de Janeiro, where the mean age was 52 years11. However, it was similar to the Bahia study9, which found a mean age of 49 years. In the 2010 Census from the Brazilian Society of Nephrology, 30.7% of the patients were aged 65 years or older [4].
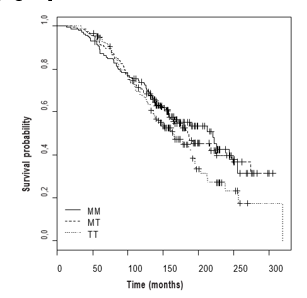
Figure 2 : Patient follow-up flowchart.
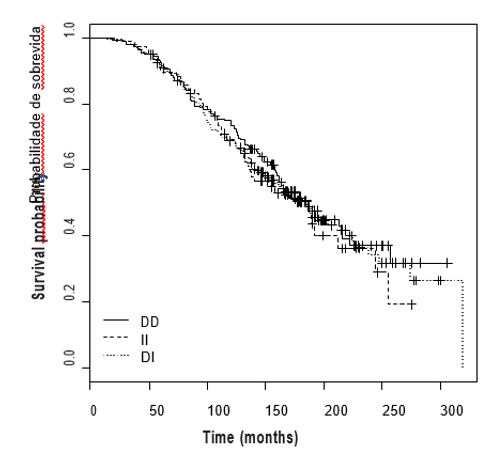
Figure 3: Kaplan–Meier curve for D/I polymorphism of the ACE gene.
The prevalence of arterial hypertension in our study (82%) was higher than the Bahia study (71%) [9], and higher than the analysis of six hemodialysis clinics in the State of Rio de Janeiro (61%)10; it was also higher than the single center study conducted in the State of Rio de Janeiro (55%) [11].
Diabetes mellitus prevalence in this study (15%) was much lower than that found in the 2010 Census by the Brazilian Society of Nephrology (28%) [4], lower than the Bahia study (21%) [9], and lower than the single center study in the State of Rio de Janeiro (20%)11. However, it was similar to the analysis involving six hemodialysis clinics in the State of Rio de Janeiro (17%) [10].
The overall survival rate found in this study was 48% at 11 years. This is higher than that found in studies with large patient cohorts, such as the European Dialysis and Transplant Association study, which recorded a 50% survival rate over five years [12]. It is also higher than the rate found in the United States, which was only 36% over five years13. Our survival results were also higher than those found in diabetic hemodialyzed patients in Japan14 (28% over 10 years). These differences can be explained by the fact that our population was younger, as well as the lower prevalence of diabetes in our study population.
With regards to the demographics of our patient cohort, it is worth mentioning that the mean age of 46 years represents a significant social impact, since this is the most economically active age group. Life
expectancy in the general Brazilian population was 73.48 years (73 years, 5 months and 24 days) in 2010, (77.32 years for females and 69.73 years for males) according to the research Tábuas Completas de Mortalidade, published on 01/12/2011 by the Brazilian Institute of Geography and Statistics15. At the age of 60, life expectancy in the Brazilian population in 2009, according to the same institute15, for both sexes was + 21.27 years (+ 19.55 for men, + 22.83 for women). This suggests that even though there was a good survival rate in our cohort, it is still lower than that of the same age group in the general Brazilian population.
A selection of survival rates from other studies are as follows. The French Tassin group found a 73% survival rate at five years16 with prolonged slow hemodialysis. A Brazilian study (3,082 hemodialysis patients, in seven Brazilian States) found a 58.2% survival rate at five years [17]. A national study of chronic hemodialysis survival in a cohort of 1,009 patients over 25 years, at three dialysis units in Santa Maria, Rio Grande do Sul, found a global survival rate of 64%, at five years, and 41%, at 10 years [18].
Our research showed similar mortality rates for male and female patients, which is different than the findings of the cohort study across seven Brazilians States [17] which found higher mortality among males.
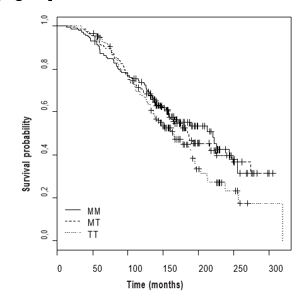
Figure 4: Kaplan–Meier curve for the M235T polymorphism of the angiotensinogen
In our study, diabetic patients had statistically higher mortality than non-diabetic ones (p = 0.0432). Lower survival among diabetics on hemodialysis has also been found in other analyses [18,19].
Body mass index was not associated with mortality in our study. A similar result was found by De Matos et al [17]. However, this finding is different from that published by Kalantar-Zadch et al [20].
Our findings showed that the highest cause of death was circulatory system diseases (34%), followed by infectious diseases (15%). Of the circulatory system conditions, the main cause was atherothrombotic vascular diseases (ischemic heart disease plus stroke), with 48% of cases. Infectious causes may be related to vascular access and with the immunosuppressive state associated with uremia. It is interesting to note that while the number of cardiovascular deaths is declining in the general population, the same is not true for patients on dialysis [21]. This difference is partly due to the demographic conditions of these individuals, when they started on dialysis. There were multiple comorbidities in our study, 15% of the cohort were diabetic, 92% were hypertensive, 26% already had ischemic heart disease, and 7% had had a stroke. A study [9] conducted in Salvador
concerning overall cardiovascular mortality and risk factors of patients on hemodialysis also showed high cardiovascular mortality of [41].7%.
We also analyzed the genetic polymorphisms of the angiotensin I-converting enzyme and of the angiotensinogen with mortality on hemodialysis. The results of the study by Inácio et al [22], in Niterói and Rio Bonito, of patients who presented as “healthy”, collected in practically the same period as our study, are different from ours for the D/I homozygotic polymorphisms in the gene of the angiotensin I-converting enzyme studied by these authors.
The literature on mortality in hemodialysis and its association with polymorphisms in the gene of the angiotensin I-converting enzyme, or of the angiotensinogen, is slim. Most studies in this area are of patients with particular diseases, diabetes being the most common.
Our study looked for a prognostic association between some polymorphisms of the renin–angiotensin system in chronic hemodialyzed patients in two important cities of the State of Rio de Janeiro. We found lower survival rates only the TT polymorphism of the angiotensinogen, and no difference in the survival rate for the D/I polymorphism of the angiotensin I-converting enzyme. Such results, showing a worse prognosis for the TT genotype, are similar to those found in analyses by Buraczynska et al [23], Lovati et al [24] and Miguel et al [27]. The differences found by the last two studies mentioned may have been due to the cohort being composed entirely of diabetics.
The study by Bzome et al [25] was designed to assess arterial hypertension complications. There was no association found between D/I polymorphisms of the angiotensin I-converting enzyme and poorer outcomes, unlike the findings in studies by Sakka et al28, Losite et al29, van der Sman-de Beer et al [30], Yoshida et al [26], Pérez-Oller et al31; Lovati et al24. These studies found decreasing survival rates for the DD genotype of the angiotensin I-converting enzyme, and many of them had short follow-up periods for a population of diabetics. Other studies [32-34] did not find any association for polymorphisms of the angiotensin I-converting enzyme or of the angiotensinogen. These studies also had short follow-ups and were conducted in a specific population with diabetic nephropathy.
Study limitations
The analysis of only two genetic polymorphisms in a highly complex system, such as the renin–angiotensin system is a limiting factor. The absence of other important variables to analyze the survival among hemodialyzed patients, such as hemoglobin, calcium, vitamin D, parathormone, erythropoietin, phosphorus, C-reactive protein, and serum albumin can also be limiting, as was the lack of information about the associations and dosages of medicines used by these patients.
The survival rate in our population was considered low when compared to the general population of the same age group. However, the survival in this cohort was high when compared to other studies involving Brazilian and North-American chronic hemodialyzed patients, as well as in comparison to most European studies. The main cause of death was circulatory system diseases, for both sexes, especially in older age groups, followed by infectious diseases and diabetes mellitus. In this study, it was not possible to demonstrate an association between polymorphisms in the gene that codifies the angiotensin I-converting enzyme (D/I) and mortality in hemodialyzed patients. The TT polymorphism of the M235 T angiotensinogen, age, and monthly family income were the variables that were associated with mortality in this cohort.
Conception and design of the research: Alves M, Silva NAS, Salis LHA; Acquisition of data: Alves M, Oliveira JMF; Analysis and interpretation of the data: Alves M, Silva NAS, Salis LHA, Godoy PH; Statistical analysis: Pereira BB, Nascimento EM; Writing of the manuscript: Alves M; Critical revision of the manuscript for intellectual content: Alves M, Silva NAS, Salis LHA, Oliveira JMF.
No potential conflict of interest relevant to this article was reported.
There were no external funding sources for this study.
This article is part of the thesis of Doctoral submitted by Mauro Alves, from Universidade Federal do Rio de Janeiro.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
