AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Manchester, M8 5RB. United Kingdom.
Citation: A K G Venyo. (2022). Simple Cysts of the Kidney: A Review and Update. Journal of Clinical Surgery and Research. 3(2); DOI:10.31579/2768-2757/030
Copyright: ©2022 Anthony Kodzo-Grey Venyo, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 September 2021 | Accepted: 24 December 2021 | Published: 07 January 2022
Keywords: simple renal cyst; simple kidney cyst; ultrasound scan; computed tomography scan; magnetic resonance imaging scan; per-cutaneous aspiration; drainage; sclerotherapy; decortication; partial nephrectomy; simple nephrectomy; selective angiography
Based upon radiology imaging features of cysts of the kidney, cysts of the kidney tend to be classified as (a) simple kidney cysts which fall under the sub-classification of Bosniak Category I and II cysts, or (b) complex renal cysts which tend to be classified as belonging to Bosniak Category III and IV cysts, or intermediate category kidney cysts which are sub-classified as belonging to Bosniak Category IIF group of renal cysts. Simple renal cysts represent benign kidney cysts that quite often tend to be asymptomatic so that generally they tend not to require any treatment and they tend to be managed conservatively or expectantly. Nevertheless, if a simple cyst of the kidney becomes symptomatic, it does need to be treated and percutaneous drainage of the kidney cyst combined with sclerotherapy or surgical treatment tends to be selected. Additionally if the size of a simple renal cysts is increasing clinicians often undertake treatment of the cysts to provide reassurance to their patients. There is no global consensus opinion regarding the treatment of simple kidney cysts. Some of the manifestations of simple renal cyst include: (a) Asymptomatic cysts of the kidney that are found incidentally upon radiology imaging investigation of a different condition, (b) a palpable lump/mass in the loin, (c) abdominal / loin pain, (d) hypertension and during investigation of the hypertension the simple cyst or cysts are found, (e) visible haematuria, (f) non-visible haematuria, (g) increasing abdominal girth, (i) loss of appetite, (j) nausea and vomiting, (k) constipation, (l) weight gain and other non-specific symptoms. Diagnosis of simple cysts tend to be undertaken and distinguished from complex renal cysts or cystic renal tumours based upon imaging features of radiology imaging options including non-contrast ultrasound scan of the renal tract, contrast-enhanced ultrasound scan (CEUS) of the renal tract, non-contrast computed tomography (CT) scan of the renal tract, contrast-enhanced computed tomography (CECT) scan of the renal tract, non-contrast magnetic resonance imaging (MRI) scan of the renal tract, and contrast-enhanced magnetic resonance imaging (CEMRI) scan of the renal tract. Treatment options for simple kidney cysts have tended to involve various options including (a) conservative treatment / leave alone, (b) Expectant management with periodical radiology imaging for follow-up assessments, (c) Per-cutaneous aspiration of the kidney cyst(s)/drainage of the cyst(s), percutaneous aspiration / drainage and sclerotherapy of the kidney cysts, (d) selective renal artery angiography and super-selective embolization of the simple renal cyst(s), (e) marsupialization / decortication of the simple renal cysts by the open method or laparoscopy technique, (f) marsupialization / decortication of the simple renal cysts by the open method or laparoscopy technique plus wadding of the operation site with omental / fat interposition, (g) partial nephrectomy by the open or laparoscopy approach to excise the cyst(s), (h) nephrectomy by the open or laparoscopy technique for large simple polycystic kidneys. Complications that could be associated with aspiration / drainage and sclerotherapy of simple renal cysts include bleeding, infection, and pain plus recurrence and persistence of renal cysts and with regard to cysts in the upper pole of the kidney could be ensued by accidental injury to the spleen and basal lung atelectasis. Embolization of the arterial branch of large and multiple renal cysts could also be associated with post-embolization phenomenon (Wunderlich’s syndrome) including general malaise, fever, loss of appetite and raised white blood cell count that may mimic infection as well as last for a few weeks and this can be prevented by administration of pre-procedure and peri-procedure steroids for a short time. Other possible treatment options for simple kidney cysts that have not been tried include radiofrequency ablation of the residual cyst pursuant to aspiration / drainage / sclerotherapy of the renal cyst, and irreversible electroporation of the residual kidney cyst pursuant to aspiration/drainage/sclerotherapy of the kidney cyst. Considering that the morbidity that tends to be associated with open surgical treatment and laparoscopy treatment options for the management of simple kidney cysts tends to be worse in comparison with per-cutaneous aspiration/drainage/sclerotherapy, generally most clinicians tend not to undertake treatment of kidney cysts initially by the open and laparoscopy procedures. Considering that persistence / recurrence of simple renal cysts can occur or do occur pursuant to percutaneous aspiration/drainage/sclerotherapy of simple kidney cysts, it would be suggested that the undertaking of percutaneous angiography and super-selective embolization of residual simple renal cysts pursuant to the initial treatment or utilization of post-procedure radiofrequency ablation or irreversible electroporation of simple kidney cysts would help reduce the incidence of recurrent and persistent simple kidney cysts and if this is undertaken hopefully the need to undertake open or laparoscopy procedures for dimple kidney cysts would be reduced. There is a need to undertake a global multi-centre trial of various treatment options for simple kidney cysts in order to ascertain the best treatment option with durable long-term outcome of non-recurrence or persistence of the renal cyst(s).
Based upon radiology imaging features of cysts of the kidney, cysts of the kidney tend to be classified as (a) simple kidney cysts that fall under the sub-classification of Bosniak Category I and II cysts, or (b) complex kidney cysts which tend to be classified as belonging to Bosniak Category III and IV cysts, or intermediate category kidney cysts that are sub-classified as belonging to Bosniak Category IIF group of kidney cysts. [1]. Simple cysts of the kidney represent benign kidney cysts that quite often tend to be asymptomatic so that generally they tend not to require any treatment and they tend to be managed conservatively or expectantly. Nevertheless, if a simple cyst of the kidney becomes symptomatic, it does need to be treated and percutaneous drainage of the kidney cyst combined with sclerotherapy or surgical treatment tends to be selected [2]. However, it has also been iterated that complex cysts of the kidney tend to be treated surgically in view of the fact that complex cysts of the kidney tend to be associated with a high incidence of malignancy [2, 3, 4]. Apart from aspiration and drainage of simple kidney cysts, treatment of simple kidney cysts that are large and symptomatic or have been associated with haemorrhage into the cyst can be treated by means of selective angiography an super-selective embolization of the renal arterial branch that supplies the blood to the kidney cyst. Even though large symptomatic simple kidney cysts can also be effectively treated by means of partial nephrectomy with complete excision of the cyst by means of an open approach or laparoscopy approach and very large symptomatic simple kidney cysts could also be treated by means of full nephrectomy by the open technique or laparoscopy technique partial nephrectomy or full nephrectomy are considered too invasive and hence these procedures generally tend not to be undertaken for simple kidney cysts. The undertaking of minimally invasive treatment procedures for simple kidney cysts including aspiration / drainage of simple kidney cysts and selective angiography and super-selective embolization of kidney cysts does require a well trained and experienced interventional radiologist as well as a well equipped and well-staffed interventional radiology department. The ensuing article is divided into two parts: A) Overview which has discussed general aspects of cysts of the kidney including simple kidney (renal) cysts and aspects of other types of kidney cysts and (B) Miscellaneous narrations and discussions related to case reports, case series and studies related to simple kidney (renal) cysts.
To Review And Update The Literature Related To Simple Cysts Of The Kidney.
Internet data bases were searched including Google, Google Scholar, Yahoo, and PUBMED. The Search words that were used included: simple kidney cysts, simple renal cysts, cysts of the kidney, renal cysts, treatment of simple kidney cysts, treatment of simple renal cysts, aspiration of simple renal cysts, aspiration of simple kidney cysts, embolization of simple renal cysts, embolization of simple kidney cysts, sclerotherapy of simple kidney cysts, sclerotherapy of simple kidney cysts. Thirty two references were identified which were used to write the article which has been divided into (A) Overview which has discussed general aspects of cysts of the kidney including simple kidney (renal) cysts and aspects of other types of kidney cysts and (B) Miscellaneous narrations and discussions related to case reports, case series and studies related to simple kidney (renal) cysts.
([A}) Overview
General Comments / Definition
A kidney cyst refers to a fluid collection within or on the kidney
It has been stated that there are many types of kidney cysts based upon the Bosniak classification of kidney cysts.
Majority of kidney cysts are benign, simple cysts which can be monitored and not intervened upon; nevertheless, some kidney cysts tend to be cancerous or are suspicious for the diagnosis of cancer and they tend to be biopsied for pathology examination to confirm or negate the diagnosis of carcinoma of the kidney and some of the suspicious complex kidney lesions have tended to be removed for pathology examination though partial nephrectomy or nephrectomy.
It has been iterated that many kidney cysts tend to be seen in cystic kidney diseases and some of these cystic kidney diseases do include polycystic kidney disease and medullary sponge kidney.
It has been iterated that kidney cysts are classified based upon their malignant risk with utilization of the Bosniak classification system and that the Bosniak Classification System was originally created by Morton Bosniak (1929-2016), who was a faculty member of the New York University Langone Medical Centre in New York City [5, 6].
It has been iterated that ultrasound scan and slice imaging are currently the key modalities that are utilized for the diagnosis of simple kidney cysts.
Benign kidney cysts tend to be defined by a set of strict criteria.
It has been iterated that any cystic kidney lesions which do not meet these strict criteria should be classified as “atypical cysts” or “complex” cysts and they should be considered to be suspicious in order to exclude malignant lesions within the cysts.
It has been iterated that for over three decades, the Bosniak classification has been the pivotal tool for the diagnosing of cystic kidney masses that are larger than 1 cm.
It has also been stated that the Bosniak classification of kidney cysts has been based upon the results of a well-established pre- and post-contrast computed tomography (CT) scan protocol.
It has been iterated that cystic kidney lesions which are difficult to classify or which remain intermediate post contrast injection could benefit from a multi-modal diagnostic approach that combines computed tomography (CT) scan, non-contrast-enhanced and contrast-enhanced ultrasound scan and magnetic resonance imaging (MRI).
It has been stated that simple cysts tend to be found occasionally within kidneys and the finding of simple cysts within the kidney has tended to increase with the age of individuals in that simple cysts of the kidney tend to be found in 0.1% of children and simple cysts of the kidney tend to be found in 20% of individuals who are older than 50 years of age [7].
Classification of Bosniak Cyst of the Kidney.
It has been iterated that the Bosniak Classification of Kidney Cysts has classified Kidney Cysts into five groups [5 , 8] as follows:
Category I
Bosniak Category I kidney cysts are benign simple cysts that contain thin walls without septa, calcifications, or solid components, and they tend to have a density of 0 to 20 Hounsfield Units (HU) [1] which is about equal to the HU of water. It has been stated that in such cases, a computed tomography (CT) scan without contrast is stated to be enough for the classification of Bosniak Category I kidney cyst [4]. It has been stated that in such situations if a contrast-CT scan is undertaken, a Bosniak Category I cyst should not depict any significant contrast-enhancement [1].
Category II
Bosniak Category II kidney cysts cyst is a terminology that is utilized for a benign cyst that has few thin septa, which could contain fine calcifications or a small segment mildly thickened calcification. Category II Bosniak cyst does include homogeneous, high-attenuation (60 to 70 Hounsfield Units [1] lesions which measure less than 3 centimetres with sharp margins lesions, but which do not exhibit contrast-enhancement. It has been iterated that Hyper-dense cysts must be exophytic with at least 75% of its wall outside the kidney in other to allow for appropriate measurement of its margins or otherwise the kidney cysts are categorized as IIF [1, 6, 10].
Category IIF.
Bosniak Category IIF kidney cysts include kidney cysts that have multiple septa, a septum that is thicker than hairline, slightly thick wall, or with calcification, which could be thick. It also does include intra-renal cysts that are larger than 3 centimetres (1.2 inches). If
There is no contrast-enhancement (otherwise category III) [11]
There is high attenuation or there is a maximum 25% of their walls visible outside the kidney (otherwise category II) [1]
Category IIF cysts are stated to have a 5% to 10% risk of being kidney cancer, and therefore follow-up is recommended. Nevertheless, there is no consensus recommendation on the appropriate interval of follow-up [11]
Bosniak category IIF kidney cysts also have the following features: [11]
cystic lesion with increased abnormal findings
multiple thin septum
septa thicker than hairline or slightly thick wall
calcification, which may be thick
intrarenal, >3 cm
no contrast enhancement
Category III
Bosniak Category III kidney cysts are indeterminate cystic masses that contain thickened irregular septa with contrast-enhancement and 50 percent of these lesions are ultimately found to be malignant.
Other iterations related to category III Bosniak kidney cyst include: [11]
malignant risk 40-60%; surgical excision recommended
More complicated
uniform wall thickening/nodularity
thick/irregular calcification
thick septa
enhances with contrast
Category IV
Bosniak Category IV kidney cysts are malignant cystic masses that have all the characteristics of category III lesions but they also exhibit contrast-enhancing soft tissue components that are independent of but adjacent to the septa. 100 percent of these lesions are said to be malignant.
Other iterations related to Bosniak Category IV kidney cysts include: [11]
malignant risk greater than 80%; surgical excision recommended
large cystic components
irregular margins/prominent nodules
solid enhancing elements, independent of septa
Tabulated Summary of Bosniak Category Classification Features.
Simple cysts of the kidney could manifest as a mass [7].
Clinical Manifestations
Salient points related to the clinical manifestations of simple cysts of the kidney have been summated as follows: [7]
About 65% of cases of simple cysts of the kidney have tended to manifest as masses within the kidney which based upon their radiology imaging features could be confused with or could simulate cystic renal carcinoma but their imaging features tend to demonstrate the kidney lesions to be avascular with smooth contours [7].
It has been iterated that simple kidney cysts could calcify [7].
It has been iterated that there could develop haemorrhage into a simple kidney cyst which would tend to make the individuals to develop pain.
Additionally some of the manifestations of simple renal cysts do include:
Asymptomatic - Asymptomatic individuals who are incidentally diagnosed as having simple renal cyst or renal cyst upon radiology imaging including ultrasound scan, CT scan and MRI Scan.
Loin pain / flank pain or discomfort.
Hypertension – some cases of simple renal cysts may be diagnosed following investigation for hypertensin.
Haematuria – Some patients who have simple renal cysts may manifest with visible or non-visible haematuria.
Increase in abdominal girth or circumference – Some individuals who have polycystic kidney disease may manifest with increasing abdominal girth or bloating size of their abdomen.
Other non-specific symptoms – Some patients who have polycystic kidney disease may complain about weight gain, difficulty in swallowing, vomiting and at times constipation and these symptoms are non-specific.
Radiology Imaging
Various radiology imaging options can be used in the assessment of kidney cysts to ascertain if the cysts are benign cysts, cysts that are potentially suspicious to necessitate exclusion of malignant kidney cystic tumours, complex kidney cysts or obvious kidney tumours. Some of the radiology imaging options include;
Ultrasound scan of the kidney and renal tract as well as contrast-enhanced ultrasound scan (CEUS) of kidneys and renal tract.
Computed tomography (CT) scan including non-contrast as well as contrast-enhanced CT scan of kidneys and renal tract.
Magnetic Resonance Imaging (MRI) scan including non-contrast and contrast-enhanced MRI scan of the kidneys and renal tract.
Recent modified 2019 Bosniak Classification of kidney cysts has been described for the assessment of kidney cysts.
Schieda et al [12]. made the ensuing summations related to the 2019 version of Bosniak Classification of Kidney cysts:
Cystic kidney masses tend to be commonly encountered in clinical practice.
In 2019, the Bosniak classification of cystic kidney masses, which was originally developed for computed tomography (CT) scan had undergone a major revision to incorporate magnetic resonance imaging (MRI) scan and is referred to as the Bosniak Classification, version 2019.
The proposed changes in the Bosniak Classification version 2019 has attempted to (a) define kidney masses (for example, cystic tumours with less than 25% enhancing tissue) to which the classification should be applied; (b) emphasize specificity for the diagnosis of cystic kidney cancers which thereby has decreased the number of benign and indolent cystic masses that are unnecessarily treated or imaged further; (c) improve interobserver agreement by defining imaging features, terms, and classes of cystic renal masses; (d) reduce variation in reported malignancy rates for each of the Bosniak classes; (e) incorporate magnetic resonance imaging (MRI) scan and to some extent ultrasound scan (US); and (f) be applicable to all cystic kidney masses encountered in clinical practice, including those which had been considered indeterminate with the original classification.
The authors had instructed upon how, utilization of computed tomography (CT) scan, magnetic resonance imaging (MRI), scan and to some extent ultrasound (US) scan. The revised classification can be applied, with representative clinical examples and images.
Practical tips, pitfalls to avoid, and decision tree rules have been included to help radiologists and other physicians apply the Bosniak Classification, version 2019 and better manage cystic renal masses.
An online resource and mobile application have also been made available for clinical assistance.
Some of the updates to the Bosniak Classification of cystic kidney masses based upon Version 2019 of the Bosniak Classification include the following:
CT scan: Proposed Bosniak Cyst of Kidney Classification Version 2019.
Category I -
CT scan: Proposed Bosniak Classification Version 2019.
Well-defined, thin, (<2>
MRI Scan: Proposed Bosniak Classification Version 2019.
Well-defined, thin, (<2>
Category II
CT scan: Proposed Bosniak Classification Version 2019.
Six types, all well-defined, with thin (equal to or less than 2 mm smooth wall.
Cystic masses with thin equal to or less than 2 mm and few 1 to 3 septa; septa and wall could contrast-enhance; could contain calcification of any type.
Homogeneous hyperattenuating equal to or higher than 70 Hounsfield Units (HU) masses upon non-contrast CT scan.
Homogeneous non-contrast-enhancing masses that amount to higher than 20 Hounsfield Units (HU) upon renal mass protocol computed tomography (CT) scan and the cyst could contain calcification of any type.
Homogeneous masses of 9 to 20 Hounsfield Units (HU) upon non-contrast computed tomography (CT) scan.
Homogeneous masses of 21 to 30 Hounsfield Units (HU) at portal venous phase of computed tomography (CT) scan.
Homogeneous low-attenuation masses that are too small to be characterised.
MRI Scan: Proposed Bosniak Classification Version 2019.
Three types of well-defined cysts with thin equal to or measuring less than 2 mm smooth walls:
Cystic masses with thin ( less than or equal to 2 mm) and few ( 1 to 3) contras-enhancing septa; any non-contrast-enhancing septa; may contain calcification of any type.
Homogeneous masses markedly hyper-intense at T2-weighted imaging (Similar to CSF) upon non-contrast magnetic resonance imaging (MRI) scan.
Homogeneous masses that are markedly hyper-intense upon T1-weighted imaging of approximately 2.5 times normal parenchymal signal intensity upon non-contrast magnetic resonance imaging (MRI) scan.
Category IIF
CT Scan: Proposed Bosniak Classification Version 2019.
[1] Cystic masses with a smooth minimally thickened, 3 mm contrast-enhancing wall, or smooth minimal thickening of up to 3 mm of one or more contrast-enhancing septa or many equal to or more than 4 smooth thin equal to or less than 2 mm contrast-enhancing septa.
MRI Scan: Proposed Bosniak Classification Version 2019
Two types:
Cystic masses with a smooth minimally thickened up to 3 mm contrast-enhancing wall, or smooth minimal thickening of up to 3 mm of one or more contrast-enhancing septa, or many equal to or more than 4 smooth thin equal to or less than 2 mm contrast-enhancing septa.
Cystic masses that are heterogeneously hyper-intense upon non-contrast fat saturated T1-weighted MRI imaging.
Category III
CT Scan: Proposed Bosniak Classification Version 2019.
[1] One or more contrast-enhancing thick equal to or greater than 4 mm width or contrast-enhancing irregular displaying less than or equal to mm obtusely marinated convex protrusion(s) walls or septa.
MRI Scan: Proposed Bosniak Classification Version 2019
[1] One or more enhancing thick equal to or greater than 4 mm width or contrast-enhancing irregular displaying equal to or less than 3 mm obtusely marginated convex protrusion(s) walls or septa.
Category IV.
CT Scan: Proposed Bosniak Classification Version 2019
One or more contrast-enhancing nodule(s) that measure equal to or higher than 4 mm convex protrusion with obtuse margins, or a convex protrusion of any size that has acute angles.
MRI Scan: Proposed Classification Version 2019.
One or more contrast-enhancing nodule(s) that measure equal to or higher than 4 mm convex protrusion with obtuse margins, or a convex protrusion of any size that has acute angles.
Treatment of Simple Kidney Cysts
Small asymptomatic simple kidney cysts tend to be left alone with no treatment or they could be observed with periodical radiology imaging to access progress of the cysts including clinical assessment of individuals who have moderate-sized kidney cysts but patients who have very small renal cysts tend to be discharged.
Percutaneous aspiration of kidney cysts- Treatment of simple kidney cysts that are associated with pain / increase in size of the cyst could be undertaken by per-cutaneous aspiration of the cysts.
Continuous negative pressure catheter drainage of simple kidney cysts. It has been iterated that some cases of simple kidney cysts can be treated by mans of continuous negative pressure catheter drainage [7, 13].
Sclerotherapy – It has been iterated that some simple kidney cysts have tended to be treated by means of sclerotherapy including alcohol sclerotherapy [7].
Selective angiography and super-selective embolization of the arterial branch to the kidney cysts.
Considering that simple kidney cysts could be small, large, single, or multiple including congenital polycystic kidneys that contain simple cysts, simple cysts of the kidney tend to be managed based upon the size, number, and location of the cysts, the age of the patients, the comorbidities of the patient, the experience and availability of an interventional radiologist and an adequately staffed radiology department as well as the availability of a well-trained urologist and anaesthetist. Some of the treatment options include:
Conservative management
Percutaneous aspiration / drainage of the cysts,
Per-cutaneous aspiration / drainage of the cyst plus sclerotherapy.
Percutaneous aspiration / drainage of the cyst followed by per-cutaneous renal artery angiography plus super-selective embolization of the arterial branch or branches feeding the cyst or cysts pursuant to the drainage to ensure recurrence of the cysts is avoided or minimized.
Per-cutaneous renal artery angiography plus super-selective embolization of the arterial branch or branches feeding the cyst or cysts alone in some cases.
Per-cutaneous renal artery angiography plus super-selective embolization of the arterial branch or branches feeding the cyst or cysts preceding the drainage the cyst or cysts to ensure bleeding complicating the drainage of large and multiple cysts is avoided or minimized.
Decortication (marsupialisation) of the renal cyst / cysts under laparoscopic procedure or as an open procedure alone.
Decortication (marsupialisation) of the renal cyst / cysts under laparoscopic procedure or as an open procedure with wadding / fat interposition of the site.
Partial nephrectomy to excise the cyst by laparoscopy technique or by the open method.
Simple total nephrectomy with excision of the entire kidney in some rare cases of multiple polycystic diseases of the kidney causing obstruction of the bowel.
Some of the potential treatment options of simple renal cysts that have so far not been reported include:
Radiofrequency ablation of the cyst alone or after aspiration of the cyst to reduce the incidence of recurrence of the cyst or cysts.
Irreversible electroporation of the cyst alone or after aspiration of the cyst to reduce the incidence of recurrence of the cyst or cysts.
Macroscopic Examination Features
It has been iterated that gross examination of specimens of simple cysts of the kidney tend to demonstrate thin-walled cortical cysts of the kidney that tend to measure up to 10 cm that tend to be filled with clear yellow fluid [7].
Microscopic Examination Features
It has been stated that microscopy examination of specimens of simple kidney cysts does tend to demonstrate the ensuing features: [7]
Microscopy examination of specimens of simple kidney cysts does tend to demonstrate a single layer of cuboidal, flattened, or atrophic epithelium of the kidney tissue [7].
Microscopy examination of specimens of simple cysts of the kidney tend to demonstrate cysts that could have thickened walls with haemosiderin laden macrophages as well as atrophic epithelium [7].
Differential Diagnoses
Some of the differential diagnoses of simple cysts of the kidney include:
Complex cysts of the kidney.
Adult cystic nephroma
Acquired cystic kidney disease
Multi-locular cystic renal neoplasm of low malignant potential
Tubulocystic renal carcinoma.
Polycystic kidney disease
Paediatric cystic nephroma.
Outcome
The outcome following various treatment options for simple kidney cysts tend to be good. The symptoms of a number of patients tend to resolve including pain, haematuria, hypertension, nausea and vomiting as well as haematuria.
Some cases of simple renal cysts tend to recur, or tend to be ensued by haematuria or bleeding into large cysts following treatment.
There may be residual cyst that could grow bigger after some minimally-invasive procedures.
There may be bleeding on retroperitoneal muscle bed which could be temporary.
If percutaneous aspiration or drainage of upper pole cysts, the procedures could be associated with development of pneumothorax or injury to the spleen that could be accidental but with modern radiology facilities this can be avoided.
Open surgical procedures tend to be associated with increased morbidity in comparison with minimally invasive procedures and with the increasing development of interventional radiology most of these treatment procedures in the developed world have tended to radiology image-based minimally invasive procedures that have been discussed in the latter part of the article with a discussion of the outcome and complications associated with the various procedures.
[B] Miscellaneous Narrations And Discussions From Some Case Reports, Case Series And Studies Related To Simple Cysts of the Kidney.
Zerem et al. [13] undertook a study which had aimed to evaluate whether continuous per-cutaneous catheter drainage with negative pressure does yield better results in comparison with single-session alcohol sclerotherapy in the management of symptomatic simple kidney cysts. With regard to the subjects and methods, Zerem et al. [13] reported that Eighty five (85) patients who had ninety two (92) simple kidney cysts were randomly assigned into two groups in a prospective controlled trial. One group of patients underwent treatment by means of sonography-guided continuous catheter drainage with negative pressure and the other group of patients underwent single-session alcohol sclerotherapy. Zerem et al [13]. analysed: patient demographics, clinical characteristics, outcome of treatment, as well as complications associated with the drainage procedure. Zerem et al. [13] summarised the results as follows:
The initial volume of the cysts did not differ significantly between the two groups of patients; nevertheless; the final volume was significantly smaller between within the continuous drainage group (P = 0.026).
During the follow-up period of 24 months, 37 (40%) of the cysts had disappeared completely; 24 of the of the 46 cysts in the drainage group that amounted to 52% and 13 of the 46 cysts in the sclerotherapy group that amounted to 28% (P = 0.033) disappeared completely.
With regard to the sclerotherapy group, the probability of disappearance of the cysts was found to be highly dependent upon the size of the cyst and noted to be less for giant cysts (P = 0.01).
The size of the cyst was found not to be a significant factor with regard to the probability of disappearance of the cyst in the with regard to the drainage group (P = 0.15).
The probability of disappearance of giant cysts that measure greater than 500 ML in volume did differ significantly between the two groups (P = 0.009); nevertheless, there was no difference with regard to the probability of disappearance of moderately large sized cysts (P = 0.16).
Three out of 14 (21.4%) patients who had giant cysts within the drainage group and 10 (76.9%) out of 13 such patients within the sclerotherapy group did develop recurrence that did necessitate additional treatment (P = 0.007). They were successfully treated by means of continuous catheter drainage.
Zerem et al. [13] made the following conclusions:
Continuous catheter drainage of kidney cysts with negative pressure is more efficient in comparison with single-session alcohol drainage in the management of giant simple kidney cysts.
With regard to moderately large simple kidney cysts, the two methods have portended similar results.
Brown et al. [14] iterated that simple kidney cysts are common benign lesions of the kidney with up to 4% of patients who have kidney cysts developing symptoms that necessitate intervention and the symptoms tend to include pain and haematuria. Brown et al. [] undertook a systematic review of the literature in order to ascertain the efficacy as well as safety of aspiration-sclerotherapy of symptomatic simple kidney cysts. Brown et al. [] undertook a systematic review with utilization of Cochrane guidelines on published literature from 1990 to 2020. They reviewed Random Controlled Trials (RCTs), cohort studies, as well as case series that met their inclusion criteria and they also cumulative analysis of outcomes of the treatments. Brown et al. [14] reported that a total of 4071 patients from 57 studies who had undergone aspiration +/- sclerotherapy for simple kidney cysts. 87.7% of the patients who had undergone aspiration with sclerotherapy had demonstrated evidence of ‘treatment successes with greater than 50% reduction in the size of the cyst as well as complete resolution of their symptoms. Brown et al. [14] additionally reported the following:
Four hundred and fifty three (453) transient complications had occurred that amounted to 11.2% of the cases and a major complication rate of less than 0.1% that involved 4 patients was reported.
Their pooled analysis of all available current literature had demonstrated that aspiration-sclerotherapy is safe as well as effective first-line treatment option for symptomatic simple kidney cysts.
Even though they were not able to compare those patients who underwent aspiration alone with aspiration-sclerotherapy, it was evident that utilization of a sclerosing agent is integral to treatment success; nevertheless, the optimum agent, volume, frequency of injection, as well as dwelling time are yet to be defined.
Brown et al. [14] recommended that the size of the kidney cyst should be taken into consideration when discussing the treatment options of simple kidney cysts; nevertheless, they had concluded that it is reasonable for the undertaking of aspiration-sclerotherapy to be utilized in the first instance with regard to all cases of symptomatic kidney cysts. Brown et al. [14] additionally, proposed that definitions of outcomes of treatment measures should be undertaken in order to allow for direct comparative analysis across future studies related to the treatment of simple cysts of the kidney.
Mohsen et al. [15] reported their experience with utilization of 95% ethanol as sclerotherapy for the treatment of symptomatic simple kidney cysts. With regard to the patients and methods, Mohsen et al. [15] reported that sixty patients who had 64 symptomatic simple kidney cysts had undergone treatment by means of ultrasound scan (US)-guided percutaneous aspiration and injection of 95% ethanol in 31 men and 29 women whose mean age was 46 years with a standard deviation (SD) of 22. With regard to the presentation of the patients, Mohsen et al. [15] reported that 34 patients had manifested with renal pain, nine patients were found to have renal mass, 11 patients manifested with hypertension, and 6 patients had haematuria. With regard to the side whether left or right, Mohsen et al, [15] reported that 24 kidney cysts were on the right, and 32 kidney cysts were on the left as well as 4 patients had bilateral kidney cysts. Mohsen et al. [15] stated that the patients were evaluated after 1 month and after that they were evaluated every 6 month by means of clinical assessment, ultrasound (US) scan examination of the renal tract, and intravenous urography. Mohsen et al. [15] defined success as complete when there was total ablation of the kidney cyst and partial success when there was recurrence of the cyst of less than half the original cyst volume with resolution of the previous symptoms. Failure of the procedure was defined as the recurrence of more than half of the volume of the kidney cyst and / or persistence of the presenting symptoms. Mohsen et al. [15] summarised the results as follows:
Pursuant to aspiration and ethanol sclerotherapy, there was non-visible haematuria in two patients and low-grade fever of less than 38.3 degrees centigrade in two patients but no major complications.
During a follow-up that had ranged between 14 months and 40 months and a mean follow-up of 19 months, there was complete ablation of the kidney cyst in 54 kidney cysts as well as partial resolution of the kidney cyst in 10 cases.
The kidney pain had disappeared or was much improved with regard to all of the patients.
Pursuant to the ablation of the kidney cyst, hypertension was well controlled with patients not requiring any anti-hypertension medication in all 11 patients who were hypertensive prior to their aspiration and ethanol sclerotherapy procedure as well as the haematuria disappeared in all six patients who had haematuria preceding their treatment procedure.
Mohsen et al. [15] made the ensuing conclusion and recommendation:
Ethanol sclerotherapy for symptomatic simple kidney cysts is simple, minimally invasive, as well as highly effective.
They do recommend ethanol sclerotherapy as first-line treatment option in these patients.
Yonguc et al. [16] compared the efficacy and safety of per-cutaneous ethanol as well as polidocanol sclerotherapy in the management of simple kidney cysts. Yonguc et al. [16] reported that with regard to materials and methods, between 2008 and 2013, symptomatic Bosniak type 1 kidney cysts that had a diameter of 5 cm upon ultrasonography (US) or computed tomography (CT) scan were included in the study and they were divided into two groups. Patients who were in group 1 were treated by means of ultrasound scan-guided percutaneous polidocanol sclerotherapy, and patients in group 2 were treated by means of ultrasound scan-guided per-cutaneous sclerotherapy. Yonguc et al. [16] documented the pre-operative as well as post-operative ultrasound scan findings in order to compare the recurrence of the cyst as well as the reduction in the size of the cysts. They defined success as complete or partial as greater than 90% reduction in the size of the cyst or 50% to 90% reduction in the size of the cyst respectively. They also defined failure of treatment as less than 50% reduction in the size of the kidney cyst. Yonguc et al. [16] compared the success rates of the two treatment groups. They assessed the intra-operative pain with utilization of a visual analogue scale (VAS) just pursuant to the operation. Yonguc et al. [16] summarized the results as follows:
The follow-up period of the patients had ranged between 12 months and 76 months with an average follow-up of 36 month in group 1 and a the follow-up period ranged between 10 months and 78 months with an average follow-up of 39 months in group 2.
Group 1 did consist of 86 patients who had 89 simple kidney cysts and group 2 did consist of 57 patients who had simple kidney cysts.
Anatomical success was recorded in 49 patients that amounted to 55.1% of cases and in 48 patients that amounted to 84.2% of the kidney cysts in groups 1 and 2 respectively with a P value of P < 0>
Clinical success was found in 56 patients that amounted to 65.1% of cases and in 43 patients that amounted to 75.4% of patients within groups 1 and 2 respectively.
Major complications was identified in one patient within group 2 that involved the development of aseptic psoas abscess, and no major complication developed within patients that were in group 1.
Minor complications did occur in ten patients within group 2 that included non-visible haematuria in six patients as well as fever and nausea in four patients and in eight patients within group 1 that consisted of non-visible haematuria in in six patients and fever and nausea in two patients.
The mean VAS scores were documented as 21+/_ 1.04 and 4.26 +/- 1.99 within the ethanol and polidocanol groups, respectively with a p value of P < 0>
Ethanol was noted to be significantly more painful in comparison with polidocanol in the sclerotherapy of simple kidney cysts.
. Yonguc et al. [16] made the ensuing conclusions:
Even though the complication rates and the VAS scores of ethanol sclerotherapy are higher in comparison with those of polidocanol, its success rates appear to be also higher.
The decision regarding which sclerosing agent should be used should be based upon the patients’ comorbidities, location of the kidney cyst, as well as the experience of the surgeon.
Aribas et al. [17] evaluated the efficacy of single-session per-cutaneous sclerotherapy with needle aspiration or catheter drainage, under ultrasound (US) scan- or computed tomography (CT) scan-guidance based upon the size of the kidney cyst, and depth of the kidney cyst in 22 symptomatic kidney cysts. With regard to the methods, Aribas et al. [17] iterated that sclerotherapy with utilization of 95% ethanol for 20 minutes was undertaken in 22 symptomatic cysts in 15 patients. The method of aspiration or drainage was chosen based upon the size and depth of the kidney cyst. Catheter drainage of the kidney cyst was undertaken for larger kidney cysts that measured higher than 6 cm and shallow kidney cysts that measured less that 7.5 cm in 12 patients (12 kidney cysts) and needle aspiration of kidney cyst was undertaken for smaller in that they measured less than 6 cm or were deeper and more than 7.5 cm in 10 patients with 10 kidney cysts. The follow-up of the patients did range between 1 month and 62 months and the median follow-up of the patients was 6.0 months. Aribas et al. [17] summarized the results as follows:
The mean and median volume reduction of the kidney cysts was respectively 94.1% and 97.0%.
The average volume reduction of the kidney cyst and the mean and median cyst volume reduction was 94.7% and 96.0% with ultrasound scan-guided methods and 93.3% and 99.0% with computed tomography (CT) scan-guided methods (P = 0.382). The median volume loss was 97.5% with needle aspiration and 96.5% with catheter drainage (P = 0.839).
No correlation was found between the groups and volume reduction of the kidney cysts was found.
All the procedures were documented as successful.
No major complications or recurrences were observed or noted.
Aribas et al. [17] made the ensuing conclusions:
The undertaking of single-session per-cutaneous alcohol sclerotherapy with utilization of needle aspiration or catheter drainage under the guidance of ultrasound scan or computed tomography scan, is an effective as well as safe method for the treatment of symptomatic simple kidney cysts.
Computed tomography- (CT)- guided needle aspiration could be more suitable for the treatment of deeper and / or smaller kidney cysts that measure less than 6 cm, and ultrasound- (US)-scan guided catheter drainage could be preferable with regard to cases of shallow and / or larger kidney cysts that measure more than 6 cm.
Agostini et al. [18] presented the long-term results of sclerotherapy of symptomatic simple kidney cysts with alcohol and aethoxysclerol followed by protracted seven-day drainage and compared the efficacy of the two sclerosing agents that were used in the treatment of kidney cysts. With regard to the materials and methods, Agostini et al. [18] reported that sixty-six (66) symptomatic patients had undergone per-cutaneous therapy with the undertaking of drainage and sclerotherapy of 72 simple kidney cysts in a day hospital setting. The kidney cysts were divided into two groups according to the size of the kidney cysts with Group 1 and Group II with cyst volume smaller or larger than 600 ml respectively for a better comparison of the results. The kidney cysts were punctured directly under local anaesthesia with a 7 French Trocar catheter with utilization of the “one-shot” technique and ultrasound scan-guidance. A pigtail catheter was next left within the cyst for the complete evacuation of the cyst fluid. Sclerotherapy was undertaken by injection of 95% alcohol or 3 Percentage aethoxyssclerol for 40 minutes and this was followed by seven-day drainage. On the basis of dimensional criteria, they defined response to treatment as recovery, partial recurrence or recurrence. Agostini et al. [18] summarized the results as follows:
Agostini et al. [18] made the following conclusions:
Akinci et al. [19] demonstrated the efficacy as well as long-term results of the single-session ethanol sclerotherapy in simple kidney cysts. With regard to materials and methods, Akinci et al. [19] reported that ninety-eight kidney cysts in 97 patients whose ages had ranged between 18 years and 76 years and whose age was 54 years were included in the study. The indications for the undertaking of the percutaneous drainage of the kidney cyst procedures included: flank pain in 74 patients, hydronephrosis in 12 patients, hypertension in 8 patients, and reassurance of the patient in view of increasing size of the cyst with regard to three patients. The mean follow-up period of the patients was 24.4 months. The procedures were undertaken with the guidance fluoroscopy as well as ultrasound scan at all times with utilization of 5-7 French pigtail catheters. Following the cystogram which was obtained in all cases, 95% ethanol with a volume of 30% to 40% of the kidney cyst volume was utilized as a sclerosing agent upon an outpatient basis. The maximum volume of the injected ethanol was 200 ml. Follow-up assessment examinations were undertaken 1 month, 3 months, 6 months and 12 months pursuant to the procedure and once each year thereafter. Akinci et al. [19] summarised the results as follows:
Akinci et al. [19] made the following conclusions:
Akinci et al. [20] stated that simple kidney cysts are rare in children and that simple kidney cysts in children tend to be managed conservatively unless the manifest with symptoms. Akinci et al. [20] undertook a study to demonstrate the efficacy as well as the long-term results of single-session ethanol sclerotherapy in symptomatic simple kidney cysts in children. With regard to the materials and methods, Akinci et al. [20] stated that three simple kidney cysts in three children who were aged 1 year, 5 years, and 16 years were included in their study. They reported that the indications for the treatment of the kidney cysts were flank pain in 1 case, hypertension in 1 case, as well as increasing size of the cyst and urinary tract infection in one patient. The follow-up of the patients had ranged between 3 years and 7 years and the mean follow-up period was 5.5 years. The procedures were undertaken under the guidance of ultrasound scan and fluoroscopy and intravenous sedation. After the undertaking of the cystogram, 95% ethanol with a volume of 40% alcohol of the cyst volume but not more than 100 ml was utilized as the sclerosing agent. Akinci et al. [20] summarised the results as follows:
Akinci et al. [20] made the following conclusions:
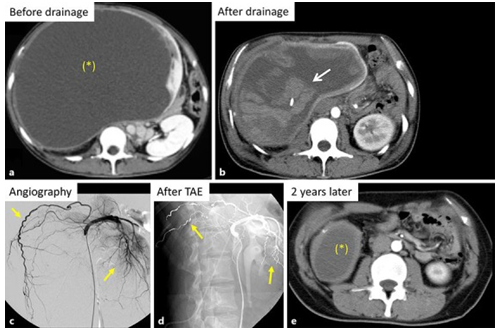
Toriu et al. [3] encountered 2 patients who had huge symptomatic simple kidney cysts With regard to the first case severe intra-cystic bleeding did occur pursuant to drainage of the kidney cyst and this was treated successfully by means of trans-arterial embolization (TAE). With regard to the second case, trans-arterial embolization (TAE) was undertaken prophylactically, and there was no bleeding associated with subsequent drainage of the kidney cyst. Toriu et al. [3] summated the cases as follows:
Case 1:
In August 2007, a 24-year-old Japanese woman was admitted into an outside hospital in order to investigate her symptoms of abdominal pain and abdominal distension. She had contrast-enhanced computed tomography (CT) scan of abdomen which demonstrated a huge homogeneous cyst that measured 50 cm x 25 cm x 18 cm that amounted to a total volume of 11,775 mL within her right kidney. The cyst was were noted to be thin and the lesion was noted to be sharply delineated from her renal parenchyma and based upon the features of the cyst, it was categorised as Bosniak Category I cyst based upon the Bosniak Classification. [1] (see figure 1a). Per-cutaneous catheter drainage of the kidney cyst was undertaken under ultrasound scan-guidance. Immediately after 4,000 mL of the cyst fluid was drained, the patient did develop severe abdominal pain and her haemoglobin dropped from 11.0 g/dL to 7.3 g/dL. In view of this further drainage and sclerotherapy of the cystic space was not undertaken. She had a CT scan of abdomen which demonstrated bleeding into the kidney cyst (see figure 1b). She did receive 800 mL of packed red blood cells. Nephrectomy was recommended; nevertheless, the patient expressed her wish to preserve her kidney and in view of this she was referred to the hospital of the authors. In her new hospital she had renal artery angiography which demonstrated elongated and narrow branches of her right renal artery encompassing the huge right renal cyst (see figure 1c). TAE was undertaken with utilization of 28 platinum micro-coils based upon the previously reported reports [4] [5] which resulted in occlusion of the feeding arteries while preserving the residual right kidney parenchyma. (see figure 1d). Pursuant to the TAE, the intra-cystic bleeding stopped and percutaneous catheter drainage was again undertaken under ultrasound scan-guidance and 4,000 mL of bloody fluid was drained. At her 2-years follow-up assessment, her right renal cyst had reduced to measurements of 6 cm x 4 cm x 4 cm with a volume of 75.4 mL (see figure 1e).
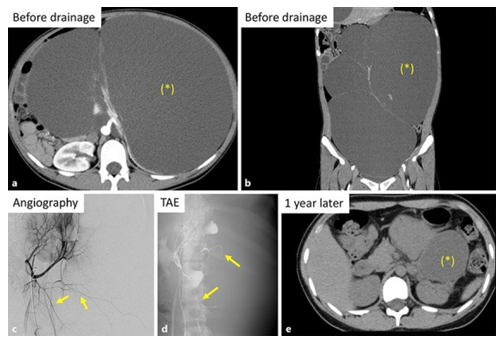
Case 2
In July 2016, a 16-year-old Japanese female was presented with abdominal distension. She had computed tomography (CT) scan of abdomen which demonstrated 4 huge cysts within her left kidney but her right kidney was normal. The total volume of the four cysts was 9,215 mL, and all her kidney cysts were categorized as Bosniak I cysts. (see figures 2a and 2b). Left nephrectomy was recommended in her referring hospital but the patient and her family preferred to avoid nephrectomy and to preserve her left kidney. She had genetic testing including PKD1 and PKD2 which were normal. In view of the fact that intra-cystic haemorrhage had developed in case 1 pursuant to catheter drainage of the kidney cyst, prophylactic TAE was undertaken in the patient so as to avoid bleeding. A total of 8 platinum micro-coils were utilized to block the branches of her left renal artery encompassing the cyst walls (see figures 2c and 2d). Subsequently a total volume of 9,400 mL of cyst fluid was drained from the left kidney cysts. Sclerotherapy was then undertaken through daily infusion of minocycline hydrochloride for 7 days and the catheters were removed. Cytology examination of the cystic fluid was negative for malignancy. During her 1-year post-procedure follow-up the total cyst volume had decreased to 633 mL (see figure 2e).
Toriu et al. [3] stated that their 2 reported cases had illustrated 2 main clinical issues including: (1) per-cutaneous catheter drainage of huge cysts is associated with a risk of severe intra-cystic haemorrhage, and (2) the undertaking of prophylactic TAE can be undertaken to prevent the development of such haemorrhage.
Shiraishi et al. [21] undertook a Japanese retrospective study related to the undertaking of laparoscopic decortication of kidney cysts of 36 patients following which they suggested that laparoscopic decortication of kidney cysts is a safe procedure that tends to be associated with satisfactory long-term symptomatic results. They additionally found that the procedure was still a challenge to undertake for peri-pelvic cysts. Shiraishi et al. [21] assessed the long-term results as well as radiological outcome of laparoscopic decortication of kidney cyst which was first reported in 1992. With regard to the patients and methods, Shiraishi et al. [21] retrospectively reviewed the records of 36 patients who underwent a total of 36 laparoscopic decortications within their institution between December 1993 and March 2004. Out of the 36 cysts 30 were peripheral cysts and six cysts were peri-pelvic cysts. The patients were questioned to ascertain if they had pain or not. They determined changes of the size of each cyst pursuant to decortication based upon the undertaking of computed tomography (CT) scans and the serial changes of each cyst were evaluated as the percentage of the diameter of the cyst preceding the surgery. They examined the relationship between the radiology image and symptomatic outcome or location of the cyst. Shiraishi et al. [21] summarized the results as follows:
.Shiraishi et al. [21] made the ensuing conclusions:
Esposito et al. [22] reported the radiology imaging follow-up of laparoscopic partial nephrectomy (LPN) in children as well as they had investigated the natural history of kidney cystic lesions pursuant to LPN. With regard to the patients and methods, Esposito et al. [22] reviewed the reports of ultrasound (US) scan imaging that were undertaken during the follow-up assessments of 123 children that included 77 girls and 48 boys whose mean age was 3.2 years, who had undergone LPN within two paediatric surgery centres between 2005 and 2015. Esposito et al. [22] summarized the results as follows:
Esposito et al. [22] made the following conclusions:
Porpiglia et al. [23] evaluated in a pilot prospective randomized trial, the safety, effectiveness as well as radiological recurrence of retroperitoneal kidney cyst decortication in comparison with retroperitoneal decortication with wadding utilizing peri-renal pedicled fat tissue. With regard to the patients and methods, Porpiglia, stated that from March 2004 to December 2007, 40 patients who had simple kidney cysts were enrolled and they were randomized into two groups as follows: Group A contained 22 patients who had undergone a simple retroperitoneal decortication (SRD) and Group B included 18 patients, who had undergone a decortication with wadding of the cyst with the utilization of peri-renal fat tissue (RDCW). Porpiglia et al. [23] recorded the following variables: the age of each patient, the gender of each patient, the side of the kidney cyst, the size of the kidney cyst upon ultrasound scan / computed tomography (CT) scan, the location of the cyst, the duration of the operation, the blood loss, the complications, the pathology, presence or absence of flank pain, hypertension, urinary tract compression or urinary infection. The reported primary endpoint of the trial was to evaluate as well as compare the efficacy of both treatment options. The secondary endpoints of the study were safety and pain, hypertension, and the resolution of urinary tract obstruction. Porpiglia et al. [23] summarized the results as follows:
Porpiglia et al. [23] made the ensuing conclusions:
Jaber and Ataya [24] reported an 86-year-old woman who had a history of orthotopic liver transplantation related to non-alcoholic steatohepatitis, stage 4 chronic renal disease secondary to calcineurin inhibitor toxicity, as well as paroxysmal atrial fibrillation and who was taking apixaban medication. She manifested with sudden right-sided abdominal pain which had radiated to her flank region. She was initially found to be hypotensive and she had tachycardia and following administration of intravenous fluids she responded well and became normotensive. The results of her initial haematology and biochemistry routine blood tests demonstrated a haemoglobin of 110 g/g/L, which rapidly dropped to 93 g/L, and her serum creatinine was 4.09 mg/dL which had risen from her baseline serum creatinine level of 2.46 mg/dL. She had a non-contrast computed tomography (CT) scan of abdomen and pelvis which demonstrated a hyper-dense right kidney with encompassing haemorrhagic fluid as well as stranding. She also had a history of bilateral simple kidney cysts related to her chronic kidney disease. In view of the fact that she did not have a history of trauma, it was presumed that she had developed spontaneous haemorrhage into one of her simple kidney cysts. Pursuant to a multi-disciplinary team meeting discussion between Urologists and Interventional radiologists it was decided that the patient should undergo renal artery angiography with the possibility of embolization of the arterial branch supplying the bleeding renal cyst. Selective renal artery angiography demonstrated multi-focal areas of active haemorrhage from both the superior and inferior poles of her right kidney. Following multiple passes to the third-order branches of her right renal artery, about 70% to 80% of her right was estimated to have been embolized. Pursuant to the embolization procedure, the lady’s haemoglobin became stable. She did experience persistence of supra-pubic pain as well as right loin pain, which did resolve 48 hours pursuant to her embolization procedure. The rest of her post-procedure stay was uneventful till she was discharged from the hospital. Jaber and Ataya [24] made the ensuing pertinent iterationsReports within the literature related to the treatment of renal intra-cystic bleeding by means of trans-catheter arterial embolization is scarce or rare as was undertaken with regard to their patient. [3]
Ubara et al. [25] reported a patient who had autosomal dominant polycystic kidney disease (ADPKD), who had been undergoing long-term haemodialysis and who had undergone trans-catheter arterial embolization (TAE) of the renal arteries in order to shrink the enlarged kidneys. Ubara et al. [25] reported that in 1983, the patient had commenced receiving haemodialysis due to chronic renal failure that was secondary to ADPKD. Nevertheless, the kidney size continued to increase. In 1997, the patient (a man) manifested with abdominal distension as well as anorexia, in addition to progression of his anaemia. He underwent upper gastro-endoscopy which demonstrated an oesophageal ulcer as well as severe external compression of the stomach. He underwent renal angiography with utilization of the Seldinger technique which demonstrated stretched as well as deformed segmental renal arteries and massive enlargement of the kidneys. TAE with utilization of stainless stell coils was undertaken on both renal arteries. Ubara et al. [25] further reported that with a rapid and progressive decrease in the size of the kidneys, the patient’s anorexia as well as anaemia improved and the gastrointestinal compression was eliminated. Ubara et al. [25] made the following iterations:
Ubara et al. [26] iterated that kidneys of patients who have autosomal dominant polycystic kidney disease (ADPKD) usually tend to continue to increase with regard to size, even after the patients commence dialysis treatment, and the mass effects could lead to severe complications. Ubara et al. [26] additionally stated that such external conventional treatments as surgical and laparoscopic procedures had not yielded satisfactory results. Ubara et al. [26] also iterated that in view of the fact that kidneys in patients who have ADPKD usually tend to be supplied by well-developed arteries, they attempted renal contraction therapy in patients who had ADPKD by renal transcatheter arterial embolization (TAE) with utilization of intravascular coils. After they had obtained informed consent, Ubara et al. [26] selected anuric patients who were undergoing dialysis treatment who had markedly distended abdomens or visible haematuria. Between October 1996 and December 2000, Ubara et al. [26] treated a total of 64 patients. Ubara et al. [26] measured the following: renal size, abdominal circumference, dry weight, haematocrit, and insulin-like growth factor-I prior to the undertaking of TAE and 3 months, 6 months, and 12 months pursuant to the TAE procedures. Ubara et al. [26] reported the results as follows:
Ubara et al. [26] concluded that their internal treatment with TAE is a safe and effective procedure which had resulted in improvement in the quality of life and nutritional status of patients who had ADPKD.
Masue et al. [27] reported the results of renal transcatheter arterial embolization (renal-TAE) in two patients who had autosomal dominant polycystic kidney disease (ADPKD) that was treated by means of haemodialysis (HD). A 73-year-old man and a 65-year-old woman who had been undergoing haemodialysis (HD) manifested with abdominal fullness, abdominal pain and loss of appetite. They had computed tomography (CT) scan of abdomen which demonstrated revealed polycystic kidneys. Both patients underwent renal artery angiography and renal trans arterial embolization (renal-TAE). Approximately 1 month pursuant to the undertaking of the renal TAE, the symptoms had improved and follow-up computed tomography (CT) scan of the abdomen showed decreased cyst volume. Masue et al. [27] concluded that the results they had obtained from treating their patients with renal TAE had suggested that renal-TAE is a useful treatment for patients who have ADPKD.
Suwabe et al. [28] iterated that currently, few strategies exist for the improvement in the quality of life (QOL) in patients who have autosomal dominant polycystic kidney disease (ADPKD) and massive kidneys. They also stated that renal transcatheter arterial embolization (TAE) does reduce the volume of kidney; nevertheless, the impact of TAE upon QOL in ADPKD patients undergoing haemodialysis is not known. Suwabe et al. [28] undertook a study to investigate the influence of renal TAE upon QOL in ADPKD patients who have massive kidneys and are undergoing haemodialysis. With regard to the method, Suwabe et al. [28] undertook a prospective observational study which enrolled 188 ADPKD patients who were undergoing haemodialysis that comprised of 92 men and 96 women; and whose mean age was 56.7 ± 9.1 years, who had undergone renal TAE at Toranomon Hospital between August 2010 and July 2014. Suwabe et al [28] used 36-item Short Form Health Survey (SF-36) questionnaire and their original 15-item questionnaire evaluate QOL. Suwabe et al. [28] summarised the results as follows:
Suwabe et al. [28] concluded that in ADPKD patients who are undergoing haemodialysis, renal TAE was effective in improving symptoms of abdominal fullness, appetite, heartburn and SF-36 scores (MCS and RCS scores), but not for sleep disturbance, constipation and physical strength (PCS score).
Soleimanzadeh et al. [29] iterated that simple renal cysts are the commonest type of benign renal tumours in adults and that they usually tend to be asymptomatic. As a prelude in their manuscript Soleimanzadeh et al. [29] stated a few things including: (a) Symptomatic renal cysts tend to be treated by means of per-cutaneous aspiration with or without injection of sclerosing agent, (b) laparoscopic decortication or wide surgery tends to be undertaken in rare cases. (c) Having taken into consideration the probable complications that ensue anaesthesia in open surgery as well as laparoscopic surgical methods, they have tended to utilize an innovative method by undertaking per-cutaneous aspiration, insertion of nephrostomy catheter for 24 hours and by injection of sclerosing agents and by leaving the agent inside the cyst whilst the catheter is removed immediately. (d) They evaluated the long-term results of their aforementioned method using ultrasound scanning. With regard to the materials and methods, Soleimanzadeh et al. [29] stated that twenty-eight (28) patients who had symptomatic renal cysts had undergone the process of inserting the per-cutaneous catheter and aspiration of its contents in two steps and one time injection of 95% ethanol. Pursuant to the first aspiration of the kidney cysts, the patients stayed admitted in the hospital for 24 hours. Then, the second aspiration was undertaken and the total fluid volume was measured. The patients were then followed up for a mean follow-up time period 14 months. They considered success of the procedure as no signs of relapse that was consistent with reduced size of the kidney cysts based upon ultrasound scan evaluation of the long-term results. Soleimanzadeh et al. [29] summarized the results as follows:
Soleimanzadeh et al. [29] made the ensuing conclusions:
Their study did show that their method of treating simple cysts of the kidney is safe, effective, as well as minimally invasive simple renal cysts and the method can be a proper substitute for other current methods that are being utilized to treat simple kidney cysts
Akinci et al. [19] published an article in order to demonstrate the efficacy as well as long-term results of the single-session sclerotherapy in simple kidney cysts. With regard to the materials and methods, Akinci et al. [19] stated that ninety-eight (98) kidney cysts in 97 patients whose ages had ranged between 18 years and 76 years and whose mean age was mean age was 54 years were included in their study. The indications for the undertaking of the drainage of the simple renal cysts included: flank pain in 74 patients, hydronephrosis in 12 patients, hypertension in 8 patients, patient re-assurance in view of increasing size of the kidney cysts in three patients. The mean follow-up of the patients was 24.4 months. The procedure was undertaken under the guidance of fluoroscopy and ultrasound scan at all times with utilization of 5-7 Fr pigtail catheters. After the cystogram which was obtained in all cases, 95% ethanol with a volume of 30% to 40% of the volume of the cyst was utilized as a sclerosing agent on an outpatient basis. The maximum volume of the injected ethanol was 200 ml. Follow-up examination assessments were undertaken at 1 month, 3 months, 6 months, and 12 months, pursuant to the procedure and once yearly thereafter. Akinci et al. [19] summarized the results as follows:
Akinci et al. [19] made the following conclusions:
Fontana et al. [30] undertook a study to ascertain the effectiveness and safety of three repeated alcohol injections for the treatment of simple large kidney cysts. With regard to the methods, from September 1991 to December 1997, Fontana et al. [30] treated 72 kidney cysts. The cyst was drained with utilization of an 8F mono J stent. Ninety-five percent sterile ethanol was injected into the cyst and left in place for 20 minutes. Two repeat alcohol injections were undertaken every 24 hours. After the third alcohol injection, the catheter was removed. In order to avoid pain in the last 39 patients, 20 mL of 2% lidocaine hydrochloride was injected into the kidney cyst for 15 minutes prior to the alcohol injections. Fontana et al. [30] summarised the results as follows:
Fontana et al. [30] concluded that in their experience, percutaneous drainage of symptomatic simple kidney cyst with three repeated alcohol injections does offer a high rate of success without the cost and morbidity associated with other procedures, such as operation or laparoscopy.
Okeke et al. [31] reported the results of a minimally invasive treatment of symptomatic simple kidney cysts as well as they proposed an algorithm for the management of symptomatic simple renal cysts. With regard to the patients and methods, Okeke et al. [31] stated that seventeen patients who had manifested with suspected symptomatic simple kidney cysts were referred for trial of aspiration of the simple renal cyst, and 16 of these patients had manifested with loin pain and one patient had presented with a flank mass. If the cyst as well as the symptoms recurred pursuant to a temporary response, they were managed by means of re-aspiration with sclerotherapy with utilization of 95% ethanol, or by means of laparoscopic de-roofing of the cyst. Okeke et al. [31] summarised the results as follows:
Okeke et al. [31] made the following conclusions:
Sakuhara et al. [32] undertook a study to evaluate the safety and effectiveness of trans-catheter arterial embolization (TAE) with utilization of ethanol in symptomatic patients who have enlarged polycystic kidneys. With regard to the materials and methods, Sakuhara et al. [32] stated that their prospective study was an institutional review board approved study which had been planned for patients who had symptoms that were related to enlarged polycystic kidney disease, such as a markedly distended abdomen, gastro-oesophageal reflux, as well as abdominal pain. At the time of the undertaking of the TAE, all of the patients had been undergoing dialysis treatment for chronic kidney failure, and their urine volume had decreased to less than 500 mL per day. Bilateral renal TAE was undertaken with absolute alcohol. Pursuant to the TAE, they evaluated changes in the volume of the kidney, clinical symptoms, laboratory data, as well as complications They analysed the differences in the kidney volumes of the patients, the clinical symptoms, abdominal circumference, and dry weights before the TAE and after the TAE with a mixed effect volume. Sakuhara et al. [32] summarized the results as follows:
Sukuhara et al. [32] concluded that kidney contraction treatment by the undertaking of TAE with ethanol injection did appear to be a safe and effective treatment with regard to patients who have symptomatic enlarged polycystic kidney disease.
None
Acknowledgements to
Case Reports in Nephrology and Dialysis and S Karger AG Basel for granting permission for reproduction of contents and figures from their journal article Under Copyright © 2018 by S. Karger AG, Basel This article is licensed under the Creative Commons Attribution-NonCommercial-4.0 International License (CC BY-NC) (http://www.karger.com/Services/OpenAccessLicense). Usage and distribution for commercial purposes requires written permission.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
