AUCTORES
Globalize your Research

Case Report
*Corresponding Author: Vincenzo Marcelli, Department of Neuroscience, Psychology, Drug’s Area and Child’s Health, University of Florence, Florence, Italy.
Citation: Giannoni B., Marcelli V., Volpe G, Marcelli E., Fetoni AR, (2024), Severe isolated bilateral posterior semicircular canal hypofunction inducing perverted head shaking downbeat nystagmus, International Journal of Clinical Case Reports and Reviews, 20(2); DOI:10.31579/2690-4861/520
Copyright: © 2024, Vincenzo Marcelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 August 2024 | Accepted: 29 August 2024 | Published: 29 November 2024
Keywords: perverted head shaking nystagmus; down beating nystagmus; head shaking test; head shaking nystagmus; posterior semicircular canals hypofunction
Downbeat nystagmus evoked by horizontal head shaking is most often a sign of central vestibular pathology. Rarely, however, such a sign may be present in peripheral pathologies that are well recognized clinically and semeiologically.
Isolated hypofunction of the two posterior semicircular canals is also a very rarely described condition, often idiopathic or mainly due to deficiency, traumatic, autoimmune or ototoxic disorders.
A 77-year-old man presented to our observation with a history of severe unsteadiness.
The clinical and instrumental examination showed a downbeat nystagmus elicited by a horizontal head shaking test (perverted) and an impairment of both posterior semicircular canals.
Findings suggesting other peripheral vestibular pathologies responsible for this sign or even a central vestibular lesion were absent. Clinical evaluation and blood testing ruled out the conditions reported as potentially responsible for bilateral posterior canal hypofunction.
The case described should lead us to consider isolated idiopathic hypofunction of both posterior semicircular canals associated only with the nystagmus finding of a head shaking downbeat nystagmus, among the peripheral vestibular pathologies already described in the literature that could be responsible for perverted Head Shaking Down Beat Nystagmus (p-HSDBN). Therefore, when faced with the latter finding in a non-emergent outpatient setting, among the various etiopathogenetic hypotheses, this type of peripheral cause should be carefully excluded before sending patients for more invasive and costly tests that may be useless and may delay healing and recovery.
The aim of our study is to present the unique case of a patient with downbeat nystagmus elicited by a horizontal head shaking test (perverted) due to an impairment of both posterior.
The Head Shaking Test (HST) is a simple bedside method used to highlight vestibular asymmetry induced by both peripheral and central lesions. In fact, in the case of predominance of one vestibular hemi-system over the other, the rapid oscillation of the seated patient's head in the horizontal plane can induce the appearance of nystagmus (Head Shaking Nystagmus - HSN), the direction of which generally indicates the predominant side [1-4]. Rarely, HST performed in the horizontal plane may generate a pure vertical nystagmus or a vertical/torsional nystagmus. This type of response is termed 'perverted' head shaking nystagmus (p-HSN) or 'cross coupled' nystagmus and is most often indicative of central pathology [5-7].
Among the different types of p-HSN, downbeat nystagmus (p-DBHSN) is the most common. It represents an altered response, often seen in stroke [7-11], drug intoxication [12,13], carential [11,14], toxic [15-18], neoplastic [7,19] and paraneoplastic [20,21] and degenerative diseases [7,22-24], due to dysfunction of the neurological structures that normally provide the correct coupling of head movements with the oculomotor response. Lesions of the nodal/ventral uvula are responsible for the inappropriate transmission of the vestibulo-ocular reflex (VOR) response elicited by horizontal HS to the vertical VOR pathways [25].
In the case of p-DBHSN, another possible pathomechanism involves a floccular/parafloccular lesion responsible for the loss of the normal inhibitory action that these structures exert on the central connections of the anterior semicircular canals to the vestibular nuclei (and not those of the posterior canals). The latter mechanism would lead to a relative predominance of the anterior semicircular canal signals over those of the posterior canals [5, 11, 24] and thus to an imbalance of the signal in favor of a tonic slow upward sliding of the eyeball.
On the other hand, p-HSN can occasionally be found as a sign of common peripheral vestibular pathologies such as benign paroxysmal positional vertigo (BPPV) [26], unilateral vestibular loss (UVL) or Menière's disease (MD) [27-29], and in rarer conditions such as vestibular paroxysmia [30]. In these cases, however, the clinical history and the morphological and temporal peculiarities of spontaneous or positional nystagmus can help clarify its origin.
In this report we present the unique case of a patient with p-HSDBN due to an idiopathic impairment of both posterior semicircular canals, in the absence of findings suggesting other peripheral vestibular pathologies responsible for this sign or even a nuanced central vestibular lesion.
A 77-year-old man presented in January 2023 with a two-month history of severe unsteadiness in the absence of oscillopsia. A slight bilateral subjective hearing loss was present before the onset of vestibular dysfunction and unchanged at the onset of vestibular dysfunction.
At the time of first evaluation a thorough general and specialized medical history was taken.
The patient underwent audiometric and impedance testing and a complete neuro-otologic examination including visuo-oculomotor (gaze-evoked nystagmus, saccade and smooth pursuit) and vestibulo-oculomotor (positional and positioning maneuvers with and without visual fixation) and hyperventilation testing. A clinical head impulse test (cHIT), a VOR cancellation test, a clinical infrared suppression head impulse test performed on all planes (IR-cSHIMP) and a horizontal head shaking test (HHST) were also administered. Instrumental vestibular evaluation included a Fitzgerald-Hallpike bithermal binaural caloric test, air conduction oVEMPs and c-VEMPs (Interacoustics, Middelfart, Denmark) to assess utricular and superior and saccular and inferior vestibular nerve function, and a video head impulse test (vHIT) recording (ICS Impulse, GN Otometrics, Taastrup, Denmark) with 20 impulses per canal (amplitude 5°-20°, head velocity 50° to 250°/s, sampling rate 250 Hz, cutoffs 0. 8 and 0.7 for horizontal and vertical canals, respectively) with a v-SHIMP test as well.
The patient also underwent routine blood tests and more specific ones with particular emphasis on folic acid, vitamin B1 and B12, electrolytes and thyroid hormone testing; a screening immunologic blood profile was also performed.
Finally, patient was submitted to a thorough neurological examination and to a cranial MRI with and without contrast targeted to the regions of the posterior fossa and of the cerebellopontine angle.
In the patient's personal history, there was no evidence of exposure to solvents or other toxic substances or recent head trauma. The patient's only general pathology was hypertension.
Blood laboratory tests were normal (especially regarding folic acid, vitamin B1 and B12, electrolytes and thyroid hormones) and there was no hematologic evidence of autoimmunity.
Audiometry and impedance testing revealed a mild bilateral sensorineural hearing loss compatible with presbycusis.
Bedside neuro-otologic examination revealed no spontaneous, positional, or positioning nystagmus. In particular, there was no spontaneous and/or positional downbeat nystagmus. cHIT, and VOR cancellation test were normal, as were bedside oculomotor tests. Performing the IR-cSHIMP test in the horizontal plane provided evidence of the normal horizontal anti-compensatory saccades generated at the end of the rotation to recover the visual target in motion integral with the head, which was briefly lost due to normal VOR gain. The same was the case when testing the vertical VOR with downward motions, thus stimulating the anterior canals. In contrast, rapid upward rotations, then with excitatory stimulus on the posterior canal, failed to show any anti-compensatory response, bilaterally. Horizontal Head shaking test revealed a pure and long-lasting p-DBHSN (video 1) which was associated with a strong subjective increase of postural imbalance.
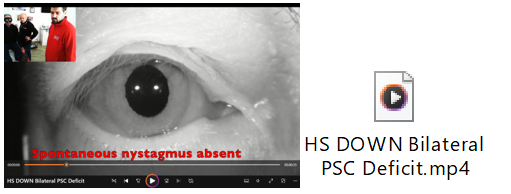
Video 1: The video shows first absence of spontaneous nystagmus and then the down beat nystagmus induced by horizontal head shaking test. Note the patient's need to hold on to the operator and be supported from behind due to the strong unsteadiness.
Video-HIT revealed severe bilateral posterior semicircular canal (PSCC) hypofunction with left and right PSCC VOR gains of 0.3 and 0.23, respectively (normal gain cut-off: 0.7) (Figure 1). However, “clustered” refixation compensatory saccades were present as an indication of the non-acute nature of the disorder and its partial compensation. c-VEMPs and o-VEMPs plotting resulted normal on both sides. Caloric testing was within the normal range.
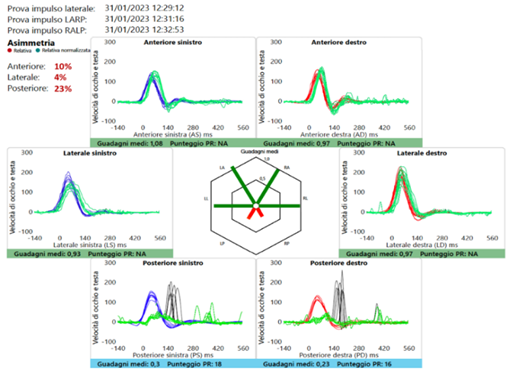
Figure 1: The patient's v-HIT trace shows normal function of the horizontal and anterior canals and a marked reduction in the gain of both PSCCs. Rapid rotation of the head in the plane of the latter with an earth-fixed target results in the appearance of overt saccades, which are already sufficiently clustered at the time of the first evaluation (v-HIT: video Head Impulse Test; PSCCs: Posterior Semicircular Canals).
The neurological examination was unremarkable. MRI of the brain showed only a few and small white matter areas of gliosis. Therefore, our diagnosis was bilateral hypofunction of the posterior semicircular canals of idiopathic nature.
Nevertheless, we started the patient on a course of specific vestibular re-education that lasted about 3 months. At the same time, the patient was recommended piracetam therapy at the dose of 1200 mg twice a day, for about 2 months.
At the 3-month follow-up, the patient reported a marked subjective improvement in postural complaints. The IR-cSHIMP test performed in the posterior canal plane was now positive for the presence of small upward vertical anti-compensatory saccades, and the HST now showed only a small DB nystagmus, still without torsional components.
We report on a clinical case that has in itself the peculiarity of the diagnosis of severe, idiopathic and isolated bilateral posterior canal hypofunction, and thus of rarely encountered disorder of peripheral vestibular function, but above all that of having, as the main revealing bedside vestibular sign, that of a pure DB nystagmus evoked by a HHST (“perverted” nystagmus), which in many cases suggests a disorder of central vestibular structures.
Testing for head-shaking nystagmus is a useful bedside vestibular test to detect asymmetry of velocity storage within the vestibulo-ocular reflex that occurs after peripheral or central vestibular lesions.
The HST is primarily performed in the horizontal plane, as performing the test in the vertical plane is more complex due to the frequent functional limitations of the cervical spine and the resulting lower standardization of results [1]. For generating HSN, asymmetric vestibular input during head rotation and asymmetric charging of the velocity storage system (VSM) is essential [3]. Another possible mechanism to induce HSN could be an asymmetric VSM function [32] and asymmetric peripheral dynamics [3], as might occur when one cupula responds more slowly than the other.
Since the lateral semicircular canal is almost always involved in peripheral vestibular pathology and the input from this canal is functionally predominant, the most observed HSN is a horizontal nystagmus, usually with its rapid phase directed to the predominant side [2,3,33,34]. More rarely, in labyrinthine disorders, there is exclusive or predominant dysfunction of the vertical semicircular canals, which may result in HSN whose rapid phase beats mainly or exclusively downward or upward in the frontal plane, even when the system is stimulated in the horizontal plane. On the other hand, an HSN that beats in a different plane than the one on which the stimulus is applied is called "perverted" or "cross-coupled" nystagmus [5,6] and is much more often an expression of dysfunction of central vestibular structures including stroke [7-10], demyelinating disorders [6], drug toxicity [12,13] and degenerative disorders [22-24]. In most cases, perverted HSN of central origin is purely vertical and with down beat direction (p-DBHSN).
The exact pathomechanism of central p-DBHSN remains uncertain and several hypotheses have been proposed. The first is based on a pathological loss/reduction of the normal inhibitory effect of the flocculus/paraflocculus on the activity of the central connections of the anterior semicircular canals, which otherwise physiologically override the activity of the posterior semicircular canals, at the vestibular nuclei [5,24,35]. Another hypothesis considers the function of the nodulus/ventral uvula, which is known to be important in ensuring that eye rotation occurs in the same plane as head rotation [25,36-37], and whose lesion is responsible for the inappropriate transfer of the activity of the horizontal VOR pathways, evoked by horizontal head shaking, to the vertical VOR pathway [38].
Therefore, when faced with a p-HSDBN, especially in an acute setting and in a first aid context, it is imperative to rule out the presence of a potentially life-threatening central pathology before considering other possible explanations.
As a matter of fact, in our patient's case, although we were not dealing with an acute-onset condition but with a long-standing disorder, among the first causes we were concerned to rule out was that of a potential morphological or functional lesion of a central nature underlying the p-DBHSN. Thorough neurological and neuro-radiological investigation and hematochemical findings seemed to exclude such an origin.
As mentioned above, other possible causes of p-HSDBN may be present in some cases of peripheral pathology. In a large cohort of subjects with a positive HST, p-DBHSN was indeed found in 24.1% of peripheral vestibular disorders, particularly benign paroxysmal positional vertigo (11.8%), acute unilateral vestibular loss (18.2%) and Meniere's disease (8.3%) [39]. Sometimes p-DBHSN could be a sign of pathology between the periphery and the centrality, i.e. vestibular paroxysmia [30].
In these cases, a p-DBHSN can be generated by an absolute or relative prevalence of the activity of the anterior semicircular canals, in the presence of normal and symmetrical functionality in the horizontal plane. Actually, an anterior semicircular canal signal predominance could theoretically be produced by a peripheral posterior semicircular canal hypofunction (i.e., caused by a canal jam altering normal endolymphatic dynamics, neuritis, hydrops) as well as by an abnormal excitation of the anterior canal afferents (ephaptic mechanism). All these above-mentioned peripheral disorders often exclusively or predominantly affect one of the two labyrinths, so any p-DBHSN that may be present is likely to have a torsional component in addition to the vertical. Peripheral vestibular pathologies that are rarely associated with p-DBHSN are usually well identified with an accurate history and careful bedside examination, and p-DBHSN is often almost completely reversible when the pathology is in an interictal phase or is healing. Our patient had no history of positional vertigo nor one suggestive of long-lasting, recurrent, episodic vertigo. He had no auditory symptoms (aural fullness, continuous or pulsatile tinnitus) or vestibular disturbances other than unsteadiness and postural instability. The sign of p-DBHSN was present at the time of the visit despite the onset of symptoms dating back to a few months earlier and bedside neuro-otologic examination revealed no nystagmus findings other than p-DBHSN. The only sign evidenced by the vestibular clinical examination and allowing a direction toward peripheral organ pathology was the bilateral lack of anti-compensatory saccades at IR-cSHIMP performed on the posterior canal plane. This observation confirms the extreme usefulness of this simple test (and whose method and results are reported elsewhere [31], which allows the evaluation of the vertical canals function with only basic instrumentation such as VOS. Instrumental testing with vHIT did indeed confirm a marked reduction in VOR gain with stimulation of PSCCs and normal function of the horizontal and anterior canals. Posterior canal hypofunction was evidenced by the presence of overt saccades that appeared sufficiently clustered to suggest that the lesion was not recent. The v-SHIMP paradigm was also performed, but this test, unlike the IR-cSHIMP, does not have the ability to verify posterior semicircular canal function under these conditions. A normal low-frequency horizontal VOR function was also demonstrated by caloric testing. Among the instrumental studies, cVEMPs were also normal, indicating proper function of the inferior vestibular nerve and supporting a primary and exclusive lesion of the PSCC afferent pathways.
There are few contributions in the literature that report on isolated bilateral PSCC hypofunction and analyze its possible causes and implications. In 2017, Tarnutzer and coll. [40] (reported that in 52 patients with PSC dysfunction, only 12 (23%) had bilateral hypofunction. Only 2 out of 12 patients with bilateral deficits showed impairment of other cochleo-vestibular receptors sufficient to allow diagnostic guidance, as was the case with most of the unilateral deficits. Thus, in the case of bilateral posterior canal hypofunction, as in our patient, the diagnosis of idiopathic nature of the lesion often remains the most common. In fact, our subject's audiometric studies showed only a picture of presbycusis, and his vestibular tests did not show any signs other than PSC hypofunction. Lerchundi and colleagues [29] also reported that among the 41 patients in their cohort with bilateral PSC failure, the most common cause was idiopathic (68%), followed by hypovitaminosis (12%), trauma (9.7%), autoimmune disease (5%), bilateral Meniere's disease, superficial siderosis, hypothyroidism, and ototoxicity, each accounting for less than 2%. All the causes just mentioned had been excluded in our patient.
In 2021 Li et al. [30] report a case series of 23 patients with loss of PSC function, of whom only 14 had isolated loss of function and of these only 2 had bilateral loss. Of these 2, only one of the subjects complained of unsteadiness as in our patient and was diagnosed with autoimmune disease. The other patient had a diagnosis and symptomatology compatible with vestibular paroxysmia. In the patient we studied, both possible causes were excluded by the hematologic and neuroradiologic (no evidence of neurovascular conflict) examinations. Moreover, in the 2 patients studied by Li and colleagues, p-DBHSN was indeed reported, but always in the presence of spontaneous DB nystagmus. Spontaneous DB nystagmus was instead absent in our patient.
To the best of our knowledge, this is the first description of a p-DBHSN associated to bilateral PSCC hypofunction peculiar for at least five different reasons: 1) bilateral PSCC hypofunction was not associated with other nystagmus findings and it was possible to attest its presence only thanks to video-HIT or by performing a simple IR-cSHIMP test, the latter of recent description but of extreme ease; 2) on video-HIT, “clustered” refixation compensatory saccades indicates a good compensation of the VOR reflex and justifies the absence of oscillopsia, while patient’s symptom testifies a weak compensation of vestibulo-spinal reflex; 3) normal c-VEMPs indicated a normal function of inferior vestibular nerves, confirming a primitive lesion of PSCC (and not a relative hyperactivity of the two anterior semicircular canals); and 4) despite the severe bilateral PSCC hypofunction the absence of spontaneous and/or positional downbeat nystagmus in static conditions suggests a good control of the tonic imbalance on the vertical plane but completely lost in dynamic conditions; 5) etiology of bilateral PSCC hypofunction remained unknown.
Although the cause could not be determined, the prompt identification of the pathological signs in the case of our patient allowed us to start a vestibular rehabilitation therapy that was of great subjective help to the patient and led to an objective improvement of the clinical and instrumental situation.
The case presented is, in our opinion, interesting because, first, it brings to light a rare diagnostic probability such as that of isolated and idiopathic bilateral hypofunction of the two posterior semicircular canals and, second, that such pathology was evidenced by the presence of a unique nystagmus sign, p-DBHSN, the latter generally and more frequently indicating a central vestibular pathology.
Except in a first aid setting, where such a sign can only be deepened for an acute central origin, in a second to third level outpatient setting and in the presence of a chronic disturbance a p-DBHSN should also raise the suspicion of the simultaneous and isolated presence of a posterior canal deficiency, even in the absence of autoimmune, toxic, deficiency or neurological pathology.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
