AUCTORES
Globalize your Research

Review Article
*Corresponding Author: P. Syamasundar Rao, MD, Professor and Emeritus Chief of Pediatric Cardiology, UT-Houston McGovern Medical School, 6410 Fannin, UTPB Suite # 425, Houston, TX. 77030.
Citation: P. Syamasundar Rao (2021) Role of Balloon Pulmonary Valvuloplasty in the Management of Pulmonary Stenosis. J.
Clinical Cardiology and Cardiovascular Interventions, 4(15); Doi:10.31579/2641-0419/195
Copyright: © 2021 P. Syamasundar Rao, This is an open-access article distributed under the terms of the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author
and source are credited.
Received: 07 July 2021 | Accepted: 06 September 2021 | Published: 21 September 2021
Keywords: pulmonary stenosis; balloon pulmonary valvuloplasty; balloon:annulus ratio; restenosis; pulmonary insufficiency; immediate results; intermediate-term results; long-term results; congenital heart defects; historical aspects; indications
Although there is definitive evidence for pressure gradient relief both immediately after and at follow-up after balloon pulmonary valvuloplasty (BPV) for pulmonary stenosis (PS), the progression of pulmonary insufficiency (PI) at late follow up emerged as a concern. To address the concern for development of PI during late follow-up, balloon/annuls ratio used for BPV was reduced to 1.2 to 1.25. Recurrence of stenosis was seen in nearly 10% of patients. The causes of recurrence were identified to be balloon/annulus ratio less than 1.2 and immediate post-BPV gradients in excess of 30 mmHg. Recurrent obstructions can be effectively relieved by repeat BPV. The BPV procedure is safe and effective in fetal, neonatal and adult subjects as well. The BPV is also effective in palliating cyanotic congenital heart disease patients with valvar PS. Despite the limitations, BPV is currently considered as therapeutic procedure of choice in the management of congenital PS in both the pediatric and adult populations. BPV provides an excellent alternative to surgical intervention and has become the preferred intervention for initial treatment for PS in neonates, infants, children, adolescents, and adults. Careful follow-up to detect development of significant PI and investigate methods to prevent PI are recommended.
Pulmonary valve stenosis may be an isolated lesion or may be seen in association with other congenital heart defects [1-4]. The most common pathology is a “dome-shaped” pulmonary valve with fusion of pulmonary valve leaflets protruding into the pulmonary artery as a conical, windsock-like structure. The valve leaflets are usually thickened and domed. The pathologic, pathophysiologic, clinical, chest x-ray, electrocardiographic (ECG), echo-Doppler and angiographic features of pulmonary stenosis (PS) were reviewed by the author elsewhere [1-8] and will not be repeated here. Surgical pulmonary valvotomy [9] has been a standard management approach for this lesion until Kan and her associates [10] reported on the application of the techniques of Dotter and Grüntzig and their associates to successfully treat pulmonary valve stenosis. In this paper the role of balloon pulmonary valvuloplasty (BPV) in the management of PS will be reviewed.
Historical Aspects
Historical aspects of percutaneous BPV were reviewed by the author in the past [11-13] and will only be briefed here. Rubio-Alverez and associates [14,15] were the first to attempt relief of pulmonary valve obstruction by using an ureteral catheter with a wire; this was in the early 1950s. In 1979, Semb et al [16] accomplished relief of pulmonary valve obstruction by forcefully pulling an inflated balloon of a Berman angiographic catheter across the pulmonary valve. There were no other reports of usage of this technique by these or other investigators. As stated above, Kan and her associates [10] applied the techniques of Dotter and Judkins [17] and Grüntzig and associates [18] to relieve pulmonary valve obstruction; this was reported in 1982. This type of static balloon dilatation is currently used all over the world to treat pulmonary valve stenosis. The author's group was among the first to recommend balloon/annulus (B/A) ratio of 1.2 to 1.4 for BPV [19,20], examine causes of restenosis after BPV [21], call attention to the development of pulmonary insufficiency (PI) during follow-up [22], and revise B/A ratio to 1.2 to 1.25 for BPV to reduce the probability of PI at follow-up [23,24] .
Indications for Balloon Pulmonary Valvuloplasty
There is a general consensus that indications for percutaneous transcatheter therapy should be same as those used for surgical intervention; however, some investigators were using gradients of 40 mmHg as an indication for BPV instead of surgical criteria for intervention of peak-to-peak gradient in excess of 50 mmHg. The author was concerned with this lowered criteria and examined this issue in a greater detail [25]. The reported results of BPV in patients with peak-to-peak systolic pressure gradients less than 50 mmHg [25] and the natural history study [26] were reviewed to see if the author's concern is valid. Fifty-three patients from the published literature as of that time had BPV which resulted in reduction (p < 0>
This editorial was written more than three decades ago and the author continues to maintain these assertions [8,22,24,27,28]. In addition, the reports of significant PI at late follow-up after BPV [22,23,29,30] further support the idea of non-intervention in patients with mild PS. Unfortunately, the American Heart Association’ Committee [31] on guidelines for intervention in pediatric cardiac disease use gradients of 40 mmHg or right ventricular peak systolic pressure of 50 mmHg for balloon therapy.
At the present time, most percutaneous interventional procedures in children are performed under general anesthesia and the pulmonary valve gradients are lower with general anesthesia than with conscious sedation. Therefore, the criteria alluded to above are not necessarily applicable. Accordingly, the pre-procedural Doppler gradients are usually used in making a decision on the need for BPV. Because of effects of pressure recovery phenomenon [32,33], correction to account for pressure recovery should be applied.
Dysplastic pulmonary valve is generally considered a relative contraindication for balloon dilatation. Our own experience [34] and that of others [35] imply that balloon valvuloplasty is the initial treatment of option and B/A ratios of 1.4 to 1.5 are likely to be effective in children with dysplastic valves [34]. It should be understood that favorable result will occur only in the presence of commissural fusion.
Some cardiologists do not recommend BPV in adult patients with moderate to severe stenosis if they are asymptomatic [36]. Because of poor response to exercise [37] and possible development of myocardial fibrosis, we recommend balloon valvuloplasty to relieve the obstruction in adults with moderate to severe PS, irrespective of the symptoms [1,8,27,28].
Preparation for BPV
The diagnosis and assessment of severity of PS are made by standard clinical, roentgenographic, ECG, and echo-Doppler data. After a diagnosis of moderate to severe PS (gradients ≥ 50 mmHg) is confirmed, arrangements for cardiac catheterization, selective cineangiography, and BPV are made [1,4,24,27,28]. A full explanation of the cardiac catheterization and balloon valvuloplasty procedure along with the risks associated with such procedures is given to the patients/parents. Such informed consent is crucial because of probability of acute complications and limited long-tem results.
Sedation and Anesthesia
In the past, BPV has been performed by sedating the patient with a mixture of meperidine, promethazine and chlorpromazine, administered intramuscularly and supplemented with intermittent doses of midazolam (versed) (0.05 to 0.1 mg/kg IV) and/or Fentanyl (0.5 to 1.0 microgram/kg IV), as necessary. General anesthesia with endotracheal ventilation was reserved to infants below the age of 3 months. Other cardiologists use ketamine for sedating these patients. More recently, most institutions are using general anesthesia for all transcatheter interventional cases including BPV in the pediatric population. The author recommends that institutional practices should be respected with regard to the type of sedation/anesthesia used and availability personnel to provide such services should also be considered.
Vascular Access
Percutaneous femoral venous route [38] is preferred entry site for cardiac catheterization including BPV. In the absence of femoral venous access, other sites such as axillary [39] or jugular [40] venous or transhepatic [41] routes may be used, although such entry sites are awkward compared to traditional femoral venous route. A # 5 to # 7 French sheath is inserted into the femoral vein by Deselets-Hoffman modification of the Seldinger technique; the size of the sheath is largely dependent on the expected size of the balloon valvuloplasty catheter.
A #3, 4 or 5 French blood pressure monitoring arterial line is introduced percutaneously into the femoral artery in infants, children and adolescents and adults respectively to continuously monitor the arterial blood pressure and to intermittently monitor O2 saturation and blood gases.
Hemodynamic Evaluation
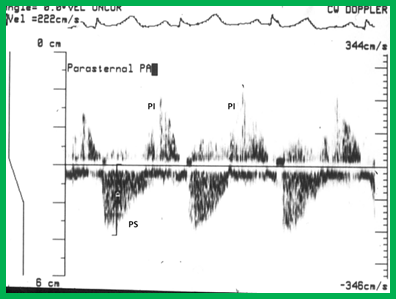
I usually start the procedure with Berman angiographic catheter. The RV and pulmonary arterial pressures are recorded and the peak-to-peak gradient across the pulmonary valve is measured. This gradient is used to appraise the severity of PS. If the Berman angiographic catheter can't be advanced into the pulmonary artery, the catheter is replaced with either a multipurpose, right coronary artery or cobra catheter and with the help of a soft-tipped guide wire such as straight Benson (Cook), the pulmonary valve is crossed and pressure pullback recordings made to obtain the pulmonary valve gradients. While pressure pullback recording is important, if it was very difficult to cross the pulmonary valve, it may not be wise to record such a pressure pullback tracing. In such cases, separately recorded RV and pulmonary arterial pressures may be used to evaluate the pulmonary valve gradient.
The RV and femoral artery pressures are simultaneously recorded; such recordings also help assess the severity of PS. RV peak systolic pressure equal to or greater than 75% of aortic or left ventricular peak systolic pressure is considered significant and such degree of pulmonary valve obstruction requires relief of obstruction.
Heart rate, aortic (or femoral artery) pressure and cardiac index are measured both before and after balloon valvuloplasty to ensure that a change in pulmonary valve gradient after the procedure is not related to a change in cardiac output, but indeed is related to the balloon procedure. We currently calculate the cardiac index with assumed oxygen consumption instead of former methods of computing cardiac index by thermodilution method and Fick technique with measured oxygen consumption.
Cineangiography
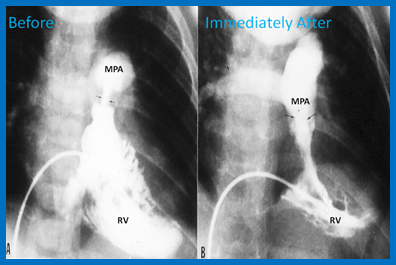
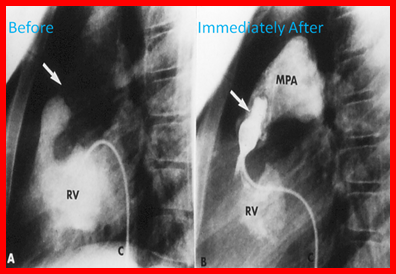
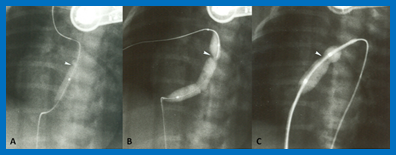
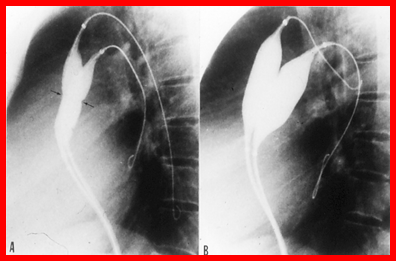
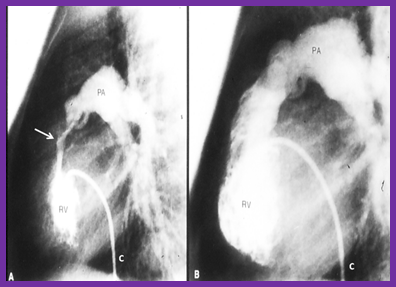
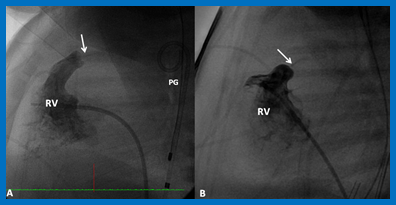
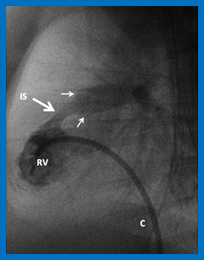
RV cineangiogram in a sitting-up (15º LAO and 35º cranial - Figure 1A) and straight lateral views (Figure 2A) is performed to confirm pulmonary valvar obstruction, to assess the size and function of the right ventricle, to detect tricuspid insufficiency, and most importantly, to measure the pulmonary valve annulus. Berman angiographic catheter is positioned in the right ventricular apex with the balloon inflated during right ventricular cineangiogram.
Other angiograms are not usually necessary unless the echocardiographic or hemodynamic information necessitates exclusion of other defects. Selective angiography of the left ventricle and coronary arteries are performed in patients older than 50 years, depending on the institutional practices or in patients in whom coronary artery disease is suspected.
Balloon Valvuloplasty Procedure
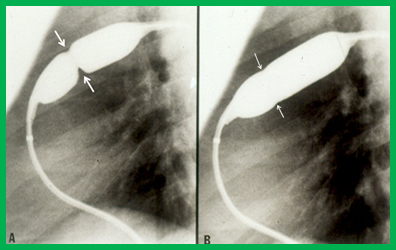
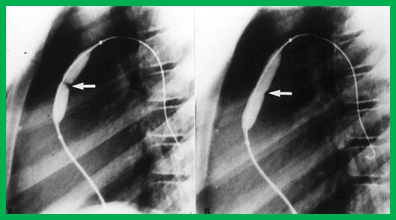
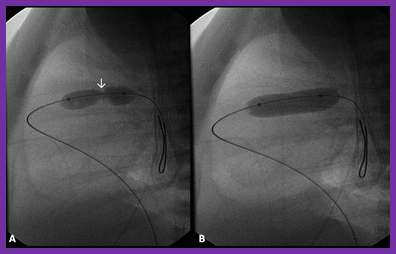
The BPV procedure consists of positioning a balloon dilatation catheter across the narrowed pulmonary valve over an extra-stiff, exchange-length guide wire and inflating the balloon until the waisting of the balloon is abolished (Figures 3 and 4).
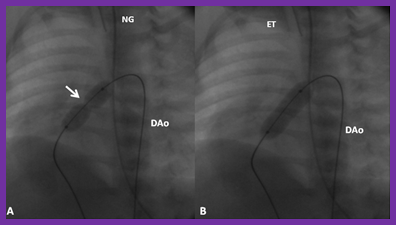
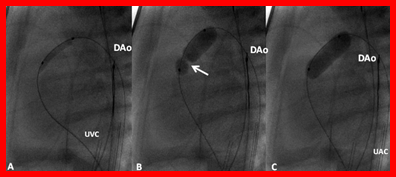
A #4- to # 6-French balloon wedge, multi-purpose, right coronary artery, cobra, angled Glidecath or any other end-hole catheter, depending on the cardiologist’s choice and the patients’ anatomy, is positioned in the RV outflow tract. A soft-tipped guide wire (my preference is 0.035-inch Benston straight guide wire [Cook]) is used to cross the pulmonary valve. In neonates and young infants, a 0.014-inch coronary guide wire with a floppy end is used to cross the pulmonary valve. The guide wire and then the tip of the catheter are advanced into the distal left (preferable) or right pulmonary artery. In neonates and young infants the catheter may be situated in the descending aorta via patent ductus arteriosus (Figure 4).
The above guide wire is removed while leaving the catheter in place. Then, a 0.014-in to 0.035-in, J-tipped, exchange-length, extra-stiff guide wire is passed through the catheter and the catheter is removed. The selection of the wire diameter is entirely dependent upon the selected balloon valvuloplasty catheter. If the size of the sheath already in the femoral vein does not house the chosen balloon dilatation catheter, the sheath is up-sized to the correct size at this juncture.
The chosen balloon valvuloplasty catheter (see the next few sections for balloon catheter selection) is advanced over the guide wire, but within the sheath and placed across the pulmonary valve (Figures 3A and 4A). A frozen video frame of the right ventricular cineangiogram is displayed on the screen and the bony landmarks, namely, ribs, sternum, or other fixed land marks are used to verify the position of the balloon catheter.
Sometimes it may not be possible to place an appropriate-sized balloon dilatation catheter across a markedly narrowed pulmonary valve, particularly in newborn infants. In those occasions, a smaller, 3–6 mm diameter balloon catheters may used first to predilate, then go with a larger, more appropriate-sized balloon catheters (Figure 5).
The balloon is inflated with contrast material, diluted 1 in 4, while monitoring the pressure of balloon inflation; any of the commercially available inflators may be used. The pressure of inflation is gradually increased to the maximum of manufacturer-recommended inflation pressure or until disappearance of the balloon waisting (Figures 3B and 4B). If the balloon is not correctly centered across the pulmonary valve, the catheter is repositioned and balloon re-inflated. I usually perform one additional balloon inflation after satisfactory balloon inflation is achieved.
Balloon Dilatation Catheters
Several types of balloon catheters were used in the past; these were reviewed elsewhere [8]. At present, most cardiologists, including our group, use Tyshak II balloon dilatation catheters for BPV because they have low profile, permitting their passage through small sheaths and easily track over the guide wire. The Inoue balloon was used in adult subject with good results [44]. The chief advantage of the Inoue balloon compared with conventional balloon catheters is that that balloon diameter is adjustable allowing stepwise dilation possible.
Balloon Diameter
The original suggestion was to utilize a balloon diameter 1.2 to 1.4 times the pulmonary valve annulus; these recommendations were devised on the basis of immediate [45] and immediate plus follow-up [19,20,46] results. Large balloons (≥ 1.5 times the pulmonary valve annulus) are likely damage to right ventricular out flow tract [47] and therefore, should not be used. In addition, such large balloon have no benefit over and above that offered by balloons with B/A ratio of 1.2 to 1.4 [20,46].
The recommendations of using balloons 1.2 to 1.4 time the valve annulus have generally been followed by most cardiologists performing BPV. However, more recent observations of pulmonary insufficiency at late follow-up [22,23,29,48-50] brought forward concerns regarding the use of large balloons [23,24,51,52]. Based on thorough examination of all the available data [23,24,51,52] it was recommended that we should attempt for a B/A ratio of 1.2 to 1.25 instead of the previously recommended 1.2 to 1.4 [19,20,45,46]. Such smaller balloons will probably result in good relief of pulmonary valve stenosis whilst at the same time may thwart development of significant PI at late follow-up.
In children with dysplastic pulmonary valves, balloons as large as 150% (B/A ratio of 1.5) of pulmonary valve annulus [34] may be necessary to produce adequate relief of obstruction. High pressure balloons [53] may also increase the effectiveness of balloon valvuloplasty in patients with dysplastic pulmonary valves.
Balloon Length
The length of the balloon used is largely dependent on the size of the patient; 20 mm-long balloons in neonates and infants, 30 mm-long balloons in children and 40 mm- or 50 mm-long balloons in adolescents and adults are generally recommended. However, no data exist either from the literature or from our own series to evaluate whether one balloon length is better than the other in producing successful relief of PS. Shorter balloons tend to slip and may not center across the pulmonary valve during balloon inflation. Long balloons tend to impinge on the tricuspid valve, producing tricuspid insufficiency [54] or on the conduction system, resulting in heart block [55]. Consequently, use of 20, 30 and 40/50 mm-long balloons for neonates and infants, children and adolescents and adults, respectively appears appropriate.
The length of the balloon used is largely dependent on the size of the patient; 20 mm-long balloons in neonates and infants, 30 mm-long balloons in children and 40 mm- or 50 mm-long balloons in adolescents and adults are generally recommended. However, no data exist either from the literature or from our own series to evaluate whether one balloon length is better than the other in producing successful relief of PS. Shorter balloons tend to slip and may not center across the pulmonary valve during balloon inflation. Long balloons tend to impinge on the tricuspid valve, producing tricuspid insufficiency [54] or on the conduction system, resulting in heart block [55]. Consequently, use of 20, 30 and 40/50 mm-long balloons for neonates and infants, children and adolescents and adults, respectively appears appropriate.
Number of Balloons
Prior to the availability of large diameter balloons, two balloons placed across the pulmonary valve (Figure 6) were used if the pulmonary valve annulus is too large to dilate with a single balloon. When two balloons are utilized in such situations, the formula listed below may be used to calculate the effective balloon size [56]:
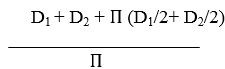
Where, D1 and D2 are diameters of the balloons used.
This formula was simplified to 0.82 (D1+D2) by Narang et al [57].
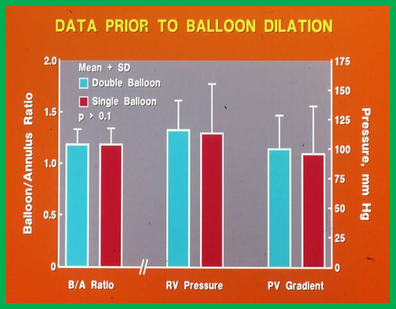
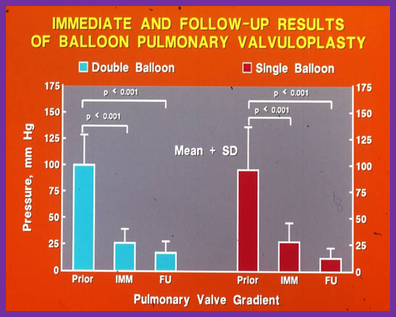
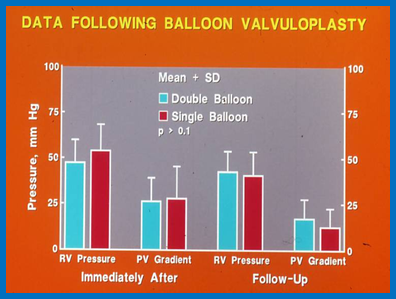
Use of double balloon technique in place of single balloon for pulmonary valvuloplasty was advocated by some interventionalists [58], especially for adult subjects. We compared the results of single balloon with double balloon valvuloplasty techniques [56] and found that the results of double balloon valvuloplasty are good and similar to, but not better than those seen with single balloon valvuloplasty (Figures 7, 8 & 9), provided B/A annulus ratios are equivalent [56,59]. Additionally, the double balloon technique does indeed lengthen the BPV procedure and requires a second femoral venous access. Furthermore, large diameter balloon catheters are currently available and make the use of single balloon instead of two balloons possible. Nonetheless, the double balloon method may be more helpful in sustaining stable balloon position across the pulmonary valve in some adolescents and adults.
Maintaining the Position of the Balloon Across the Pulmonary Valve During Balloon Inflation
At times it may not be possible to maintain the position of the balloon across the pulmonary valve during balloon inflation. Utilizing appropriate length of the balloon depending upon the age of the patient (as mentioned in a preceding paragraph) and holding the balloon catheter tight to curtail its movement is expected to circumvent this problem. Double balloon technique, especially in adolescents and adults may be useful. Use Adenosine [60] or rapid right ventricular pacing [61] to induce transient cardiac standstill, thus achieve stable position of the balloon during valvuloplasty have been advocated and such techniques may be used at the discretion of the cardiologist performing the procedure. However, we have not found these techniques necessary for PS, although they may be useful for balloon aortic valvuloplasty [62]. Inoue balloon catheters [44], because of their configuration may help hold the balloon across the valve during valvuloplasty. Nucleus balloon (NuMed) with a “barbell” configuration and hourglass-shaped V8 aortic valvuloplasty balloons (Venus Medtech) may also help keep the balloon across the pulmonary valve. However, these balloon catheter are bulky and their usefulness has not been validated.
Pressure, Number and Duration of Balloon Inflation
Balloon inflation pressure (2.0 to 8.5 atm) used, number of balloon inflations (one to four) employed and duration balloon inflation (5 to 60 seconds) are diverse and differed from one study to the other. However, there are no data to support use one parameter over the other. We have scrutinized these parameters from our study subjects [42,59]. The balloon inflation characteristics of the patients with good results were compared with those of poor results. No significant differences were detected indicating that the results of valvuloplasty are not linked to the above mentioned balloon inflation characteristics. We have also analyzed these data [42,59] with random cutoffs of maximum pressure, number of balloon inflations and duration of balloon inflation and found that higher pressure, larger number of inflations and longer duration of balloon inflation did not positively influence residual gradients at follow-up, especially when the effect of B/A ratio is accounted for. Based on these and other considerations, I suggest that balloon inflation at or below the level of balloon burst pressure stated by the balloon catheter manufacturer and continue balloon inflation until the waisting of the balloon abolished (Figures 3B, 4B and 6B). The duration of balloon inflation should be as short as possible, usually just until after the waist disappears. Shorter balloon inflation cycles produce less hypotension and more rapid return of aortic pressures towards normal. We generally perform one additional balloon inflation following disappearance of waisting, to ensure satisfactory valvuloplasty.
Post-Balloon Hemodynamic Evaluation and Follow-up
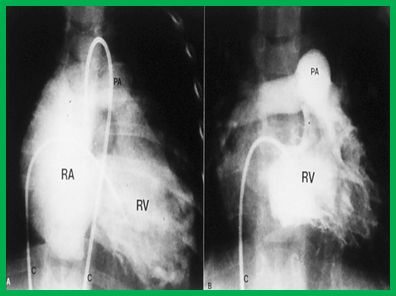
After completion of BPV, pressure gradient across the pulmonary valve, simultaneous femoral artery and RV pressures, and pulmonary and femoral arterial oxygen saturations are recorded in an attempt to evaluate the result of the procedure. Either a Tuohy-Borst or a multi-Track catheter [63] may be used to measure the pulmonary valve pressure gradients. This would allow retaining the guide wire across the pulmonary valve in place should the result prove to be not satisfactory (peak-to-peak valvar gradient ≥30 mmHg). In such instances, a repeat balloon valvuloplasty may be performed with a larger balloon (2 mm larger than the initial balloon used). Then, the guide wire and catheter are withdrawn and right ventricular cineangiogram is performed with a Berman angiographic catheter positioned in the RV apex; this will help assess the mobility of the pulmonary valve leaflets, visualize the jet of contrast across the dilated pulmonary valve (Figures 1B and 2B), detect infundibular stenosis and identify tricuspid insufficiency.
The patients are observed in an intermediate care setting until next morning while monitoring heart rate, pulse oximetry, blood pressure, pulses, and bleeding at the puncture site. An ECG and an echocardiogram are usually performed on the morning after the valvuloplasty. Clinical, ECG and echo-Doppler assessment is performed at 1, 6, and 12 months and 2 and 5 years after the procedure. We would also recommend follow-up every 5 years there afterwards, particularly to evaluate PI.
Immediate Results
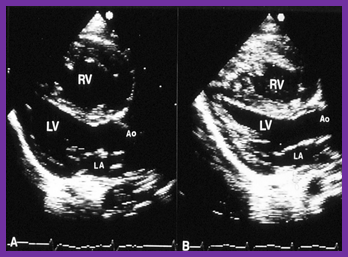
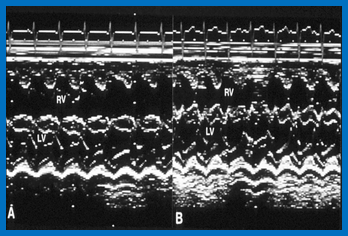
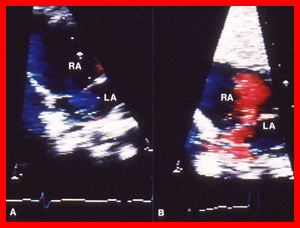
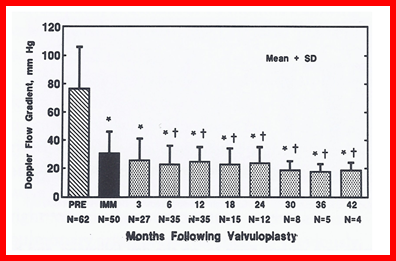
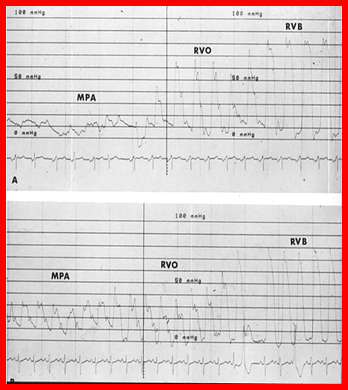
Immediate results of BPV were presented by the author in the mid-1980s [64,65] with subsequent publication of immediate results in larger groups of patients [4,22,42,66]. Reduction of peak-to-peak systolic pressure gradients across the pulmonary valve and right ventricular peak systolic pressures along with mild increase in pulmonary artery pressures occurred (Figures 10 and 11) after balloon dilatation without a change in the cardiac index. The jet width of contrast material across the PV become wider (Figures 1 and 2). The size of the right ventricle decreased (Figures 12 and 13). On post-balloon cine-angiographic and echocardiographic studies, excursion of the pulmonary valve leaflets appeared freer with less doming. Right-to-left shunt across the atrial septum, if present prior to balloon valvuloplasty, decreased, abolished or reversed (Figure 14). However, some children with very severe PS developed infundibular obstruction [68], some requiring beta-blocker therapy [68,69]. The issues related to development of infundibular obstruction will be discussed in a later section of this chapter. Surgery was avoided in most, if not all patients. All patients with the exception of neonates were discharged home within 24 to 48 hours after balloon valvuloplasty [4,22,42,64-66].
Acute Complications
Complications related to balloon valvuloplasty have been extremely low. The Valvuloplasty and Angioplasty of Congenital Anomalies (VACA) registry reported results of 822 BPV procedures performed at 26 institutions, representing initial experience at these centers [70]. The death rate was 0.24% with a major complication rate of 0.35% [70]. Since this is initial experience of the participating centers, the complication rate should become even lower with increasing experience.
Decrease in arterial pressure during balloon inflation, transient bradycardia and premature beats have been uniformly observed by most investigators. However, these abnormalities rapidly revert to normal once the balloon is deflated [67]. Hypotension may be less if a patent foramen ovale (PFO) is present [71]; probably related to right-to-left shunting across PFO filling the left ventricle. Double, bifoil or trefoil balloons have been advocated by some cardiologists to avoid the hypotension problem, but these catheters are bulky and do not truly have space to allow forward flow. The author recommends short periods of balloon inflation, which are likely to decrease the degree and duration of hypotension [67].
Blood loss, right bundle branch block, transient or permanent heart block, cerebrovascular accidents, loss of consciousness, cardiac arrest, convulsions, balloon rupture at high balloon inflation pressures, rupture of tricuspid valve papillary muscle, and pulmonary artery tears have been reported, though rare [4,70]. Meticulous attention to the technique, use of appropriate diameter and length of the balloon, avoiding high balloon inflation pressures and short inflation/deflation cycles may thwart or decrease the complications [4]. Infundibular obstruction [68,69] may also develop and will be reviewed in a later section of this paper.
Transient prolongation of the QTc interval [72,73] and premature ventricular contractions [74] after BPV have been reported, raising concerns for development of R-on-T phenomenon with resultant ventricular arrhythmia. Occasional instances of ventricular arrhythmia have been seen, but none of the patients in our large series [22] and many other studies were known to develop significant ventricular arrhythmia. However, it is prudent to monitor patients' ECG after balloon valvuloplasty.
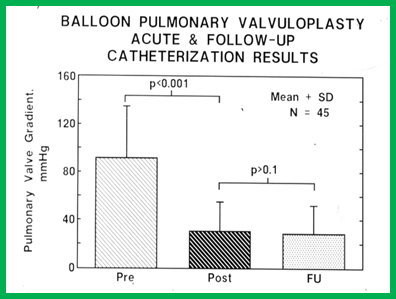
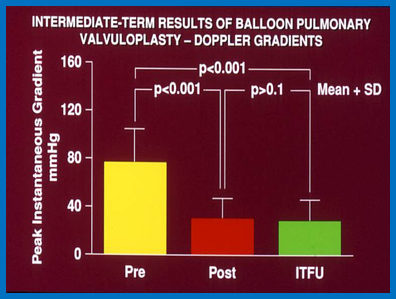
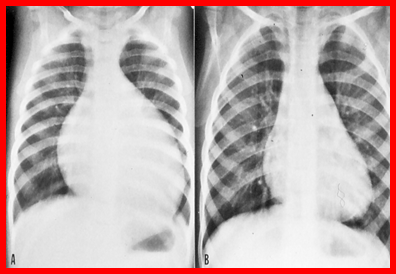
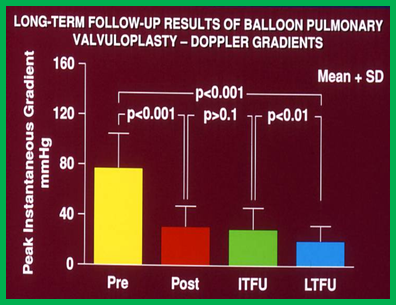
At intermediate-term (defined as six months to 2 years) follow-up, the pulmonary valve gradients remain improved compared to pre-valvuloplasty values and are unchanged when compared immediate post-valvuloplasty gradients for the group as a whole. This reduction in the gradients was demonstrated by both catheterization-measured peak-to-peak systolic pressure gradients (Figure 15) and Doppler-calculated peak instantaneous gradients (Figures 16 and 17) [4,22,24,42,59,66]. The size of the heart on a chest x-ray (Figure 18), right-to-left atrial shunt (Figure 14), right ventricular function, tricuspid insufficiency (Figure 19) and infundibular constriction (Figures 20 and 21) continued to improve during follow-up [4,24,59,66,67].
However, when results of each patient are separately reviewed, 8 to 10% patients developed restenosis (Figure 22) defined as gradient in excess of 50 mm Hg [21,22]. The causes of restenosis [21] will be reviewed in a subsequent section of this paper. Patients with restenosis have been successfully treated by repeat dilatation with balloons larger than those used at the time of initial balloon procedure [76]. However, if the reason for recurrence is pulmonary valve annular hypoplasia, pulmonary valve leaflet dysplasia, fixed infundibular obstruction (not controlled by beta-blocker therapy) or significant supravalvar pulmonary artery stenosis, surgical intervention is indicated. Improvement in atrial right-to-left shunting (Figure 14), right ventricular function and tricuspid insufficiency (Figure 19) continued during follow-up [22].
Long-Term Follow-Up Results
At long-term follow-up, the results of 80 patients who were monitored for three to ten years (median seven years) were scrutinized [22] and will be discussed under the following headings:
Residual Gradients
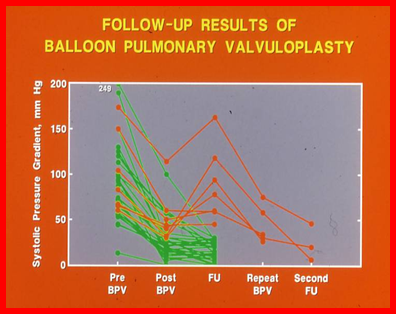
The long-term follow-up results of BPV are excellent, with very low (17 ± 12 mmHg) residual pulmonary valve gradients (Figure 23); these gradients were lower than the pre-valvuloplasty gradients (p < 0>
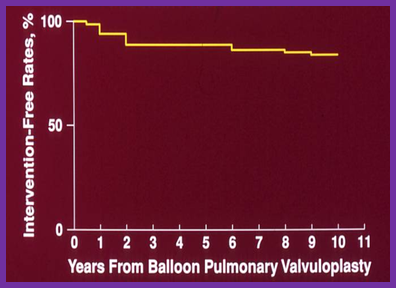
Four children had re-interventions during long-term follow-up, in addition to seven children requiring repeat balloon valvuloplasty to treat restenosis and two children requiring the resection of fixed infundibular obstruction during intermediate-term follow-up. These late re-interventions consisted of surgery to relieve supravalvar pulmonary artery stenosis (N=1) and infundibular pulmonary stenosis (N=1), and repeat balloon valvuloplasty to relieve recurrent valvar stenosis (N=2). The actuarial re-intervention-free rates were in the high and mid-80s at five and ten years, respectively (Figure 24) [22].
Ventricular Dimensions
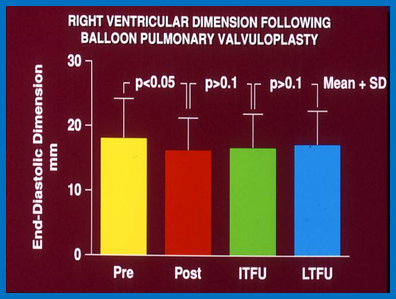
While there was a significant decrease (p < 0.05) in the right ventricular end-diastolic dimension immediately following the balloon procedure, there was no further change (p > 0.1) at intermediate and long-term follow-up (Figure 25) [22]. In addition, the RV dimension was within the normal values for the square root of the body surface area for the given age. The left ventricular end-diastolic dimension had increased (p < 0>
Pulmonary Insufficiency
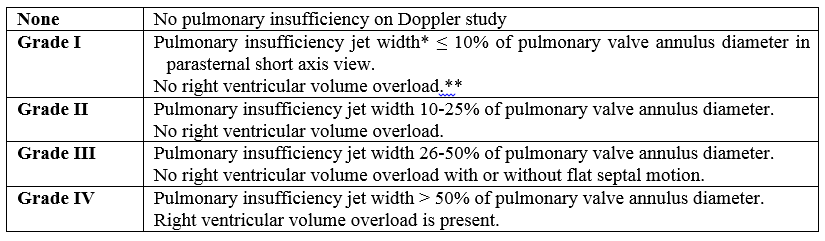
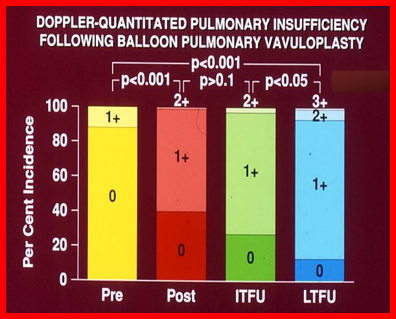
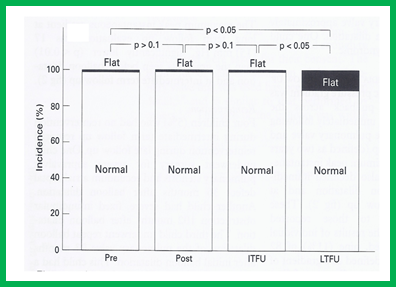
A grading system was developed to evaluate the degree of PI (see Table I) [22]. A gradual but significant (p < 0.05 to p < 0.001) increase in the prevalence of PI was seen from pre-valvuloplasty to one day after BPV, and then throughout intermediate-term and long-term follow up (Figure 26). There was also an increase in the prevalence of flat septal motion (Figure 27) which may indicate the development of a right ventricular volume overload secondary to PI; however, no patient developed paradoxical septal motion.
Summary of Long-term Results
In summary, the long-term results of BPV are excellent, with an infrequent need for re-intervention, and this affirms that BPV is the treatment of choice in the management of valvar PS; however, our study raises concern regarding the development of PI at late follow-up [22].
Complications at Long-Term Follow-Up
The complications at long-term follow-up include femoral venous obstruction, pulmonary valve restenosis, and PI. Femoral venous obstruction may develop [5] and has been seen in 7 to 19% of the patients; such obstruction is more likely in small babies. Additional pulmonary valve obstruction is minimal beyond what was seen at mid-term follow-up [22]. If dysplastic valves without commissural fusion, supravalvar pulmonary artery stenosis or severe fixed infundibular obstruction are the reasons for recurrence, surgical intervention may be needed. PI has been observed during long-term follow-up [22,52] and will discussed in a later section of this paper.
Restenosis and Predictors of Restenosis
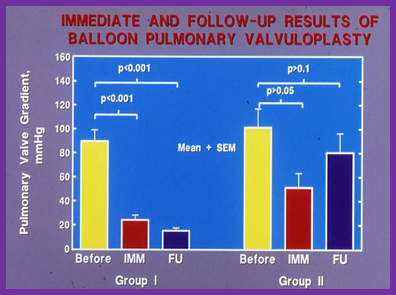
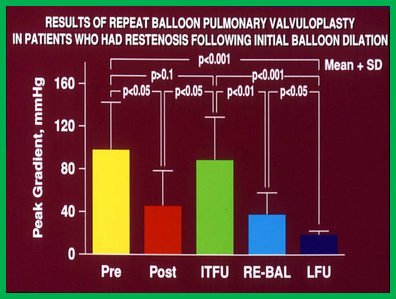
As mentioned above, restenosis following BPV does occur (Figure 22). The causes of restenosis after balloon pulmonary valvuloplasty were investigated by scrutinizing the follow-up results of 36 children [21]. The study subjects were divided into two groups: Group I – 29 children who had good results with residual peak-to-peak systolic pressure gradients of less than 30 mmHg at follow-up, and Group II – 7 children who had poor results with gradients ≥ 30 mmHg at follow-up. In Group I, the peak-to-peak pulmonary valve gradients decreased (p<0> 0.05) which increased to 81 ± 41 mmHg at follow-up (Figure 28, right panel). Of these seven children, five had repeat balloon dilatation with significant (p<0>
Fourteen sets of biographic, anatomic, physiologic, and technical data were examined by multivariate logistic regression analysis to identify the factors causing recurrence [21]. The age at valvuloplasty, duration of follow-up, frequencies of pulmonary valve dysplasia, valve annulus hypoplasia, infundibular PS, RV hypoplasia, RV peak systolic pressure, pulmonary valvar and infundibular systolic pressure gradients, the number of balloon inflations, balloon inflation pressure, and duration of balloon inflation were similar (p > 0.1) between the two groups (for the interested reader, see Tables I, II and III of our publication [21]). However, stepwise logistic regression analysis identified two factors responsible for restenosis: 1. A B/A ratio <1>30 mmHg. The relationship between the B/A ratio (Figure 29) and immediate post-valvuloplasty gradients (Figure 30) on the one hand and the recurrence at follow-up on the other is shown in Figures 29 and 30. The rate of restenosis decreases (p = 0.001 to 0.002) as the B/A ratio increases. With a B/A ratio of > 1.2, there were no recurrences (Figure 29). Immediate post-valvuloplasty peak-to-peak pulmonary valve gradients > 30 mmHg are associated with a higher rate of recurrence (p = 0.001) when compared with post-BPV gradients < 30>
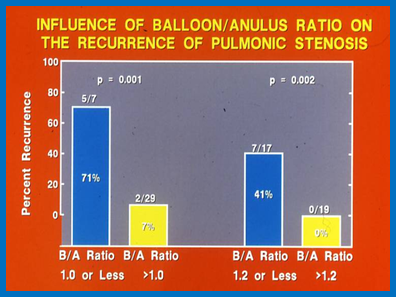
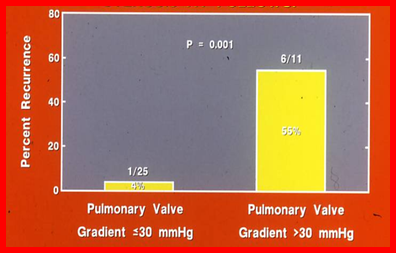
On the basis on these data, we extrapolated that a B/A ratio of less than 1.2 is likely to be the reason for recurrence at intermediate follow-up and such recurrences may be foreseen by an immediate post-valvuloplasty gradient in excess of 30 mmHg [21]. Therefore, we supported the use of larger balloons to decrease the valvar (not infundibular) gradients to < 30>
Since the role of balloon size in recurrence is now known, most cardiologists use balloons larger than the valve annulus for BPV, and therefore the reasons for recurrence at the present time are more likely to be local anatomic abnormalities such as valve ring hypoplasia, PV dysplasia, and supravalvar pulmonary artery stenosis [8].
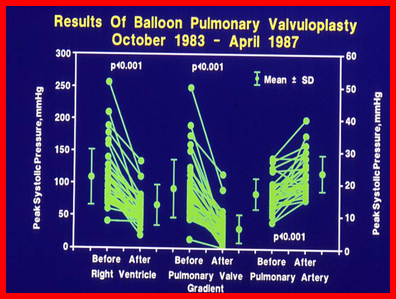
As indicated above, the recurrence of PS after balloon valvuloplasty was observed. We have studied the feasibility and effectiveness of repeating balloon valvuloplasty to relieve the recurrent obstruction [76]. Eighty-five children underwent balloon pulmonary valvuloplasty between 1983 and 1993, with a reduction in pulmonary valve peak gradients from 91 ± 41 mmHg to 25 ± 19 mmHg (p < 0>
However, at the present time, most cardiologists use balloons larger than the pulmonary valve annulus and therefore, the recurrences described above may not occur as frequently as before. If the reason for recurrence is pulmonary valve annular hypoplasia, pulmonary valve leaflet dysplasia, fixed infundibular obstruction (not controlled by beta-blocker therapy) or significant supravalvar pulmonary artery stenosis, surgical intervention is indicated.
Management of Restenosis After Prior Surgery
The recurrence of PS following prior surgical valvotomy has been reported. There are limited reports of managing such post-surgical PS by BPV. From our BPV group [4], there were two patients, aged three and 14 years, who had pulmonary valve gradients of 120 and 146 mmHg at post-surgical follow-up cardiac catheterization. BPV was performed in both of these children, with a reduction of the pulmonary valve gradients to 48 and 34 mmHg, respectively. In one of these children, a follow-up echo-Doppler study 10 months after BPV showed a peak instantaneous gradient of 25 mmHg. These results are encouraging. It was concluded that BPV is the treatment of choice for restenosis following prior surgical therapy [4].
Infundibular Stenosis & BPV
Occurrence of infundibular narrowing after balloon pulmonary valvuloplasty has been studied [68,69]. Fontes and his colleagues [69] have reported the emergence of important infundibular obstruction after BPV. They reviewed the results of 33 patients with severe PS who had supra-systemic systolic pressures in the RV; 24 (73%) patients developed infundibular stenosis. These authors suggested administration of propranolol for gradients ≥ 50 mmHg. They also showed that the infundibular obstruction regresses during follow-up. They conclude that infundibular stenosis is reactive and reversible and in spite this balloon valvuloplasty should remain the treatment of preferred option even in patients with severe pulmonary stenosis [69].
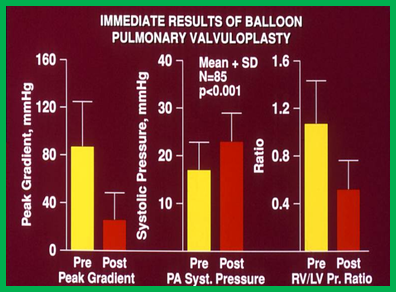
We have designed a study to investigate the prevalence and significance of this problem and its clinical implications [68]. We analyzed the data on 62 consecutive children (aged seven days to 20 years [median, six years]) who had BPV during a 55-month period ending in May 1988 [68]. The peak-to-peak systolic pressure gradient across the pulmonary valve decreased from 93 ± 43 to 27 ± 19 mmHg (p < 0>
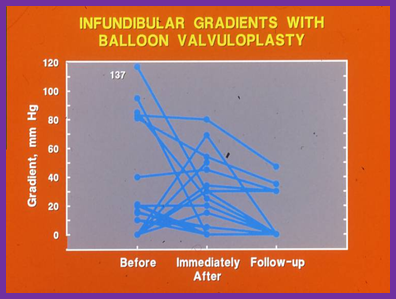
At intermediate-term follow-up, the infundibular obstruction either disappeared or further decreased (Figures 20A, 21C, and 32). At the time of the conclusion of this study [68], no child required surgical intervention. Nevertheless, at follow-up after a longer duration [22], three (4%) of 80 children required surgical intervention to relieve fixed infundibular stenosis, months or years following initial balloon valvuloplasty.
A total of 18 (29%) of 62 PS patients had infundibular gradients. The influences of the patient’s age at valvuloplasty and the severity of the pulmonary valve stenosis on the development of infundibular obstruction was examined; the prevalence of infundibular obstruction was higher with increasing age and an increasing degree of PV obstruction (Figure 33) [68].
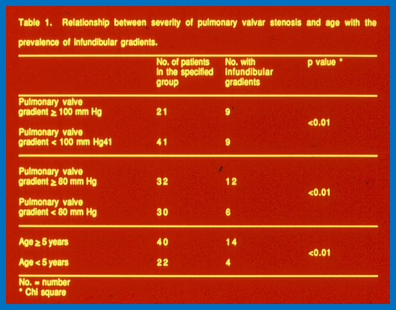
We concluded that infundibular gradients are seen following BPV in nearly 30% patients, with a higher incidence (75%) in patients with severe PS with supra-systemic right ventricular pressure [68,69]. The prevalence of infundibular obstruction is more common with increasing age and severity of PS. Children who develop systemic or supra-systemic right ventricular pressure secondary to a hyper-reactive infundibulum should receive beta blockade therapy [68,69]. The recommendation to use a beta blockade for infundibular gradients > 50 mmHgis appropriate [68.69]. The infundibular obstruction does regress to a great degree at follow-up (Figures 20A, 21C, and 32) and the need for surgical intervention is rare. The probability for the development of infundibular gradients should not deter cardiologists from the use of balloon valvuloplasty in the management of valvar PS. BPV should be performed prior to the age of five years and prior to the development of pulmonary valve peak-peak systolic gradients more than 80 mmHg, to prevent/reduce infundibular obstruction. The recommendations for the management of post-balloon infundibular PS [77] are summarized in Table II.
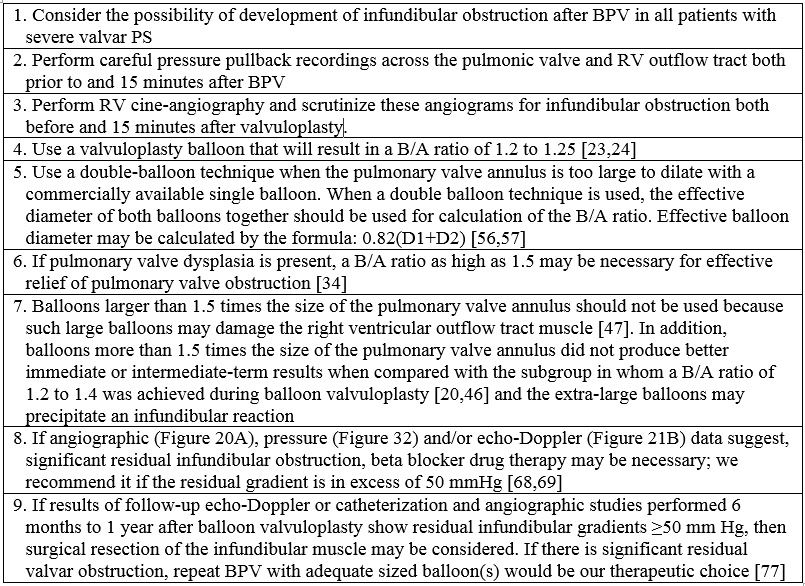
Modified from Rao PS, Thapar MK. Am Heart J 1991; 121: 1839-1840 [77].
Pulmonary Insufficiency
We were among the first to point out that PI may become a significant problem during long-term follow-up after BPV [22]; there was a progressive increase in the prevalence and severity of PI (Figure 26). PI was also observed in 40-90% of patients by other investigators. But RV dilatation (volume overloading) did not develop in most studies, including ours (Figure 27). However, in one study [29] severe PI was observed in six of 107 (6%) patients at late follow-up; some of these patients required surgical replacement of the pulmonary valve. The data from these investigators [29], along with that reported by us [22,78], led the author to conclude [23] that the development of significant PI at late follow-up, as reported by Berman [29], is an important observation and that attempts to establish the causes of late-onset PI, to develop methods to avoid such problems, and to undertake cautious long-term follow-up studies to corroborate Berman’s findings are needed.
Berman’s study [29] indicated young age, severe degrees of PS, large B/A ratio, use of noncompliant balloons, and low post-BPV peak-to-peak systolic pulmonary valve gradients as features that had a role in the development of late PI. Other investigators, as reviewed elsewhere [8], also documented the late development of PI. Accordingly, methods to avoid such problems should be sought. My independent analysis [23,24] suggested balloons 1.2 and 1.25 times the size of the pulmonary valve annulus may be a correct choice for BPV instead of the previously recommended B/A ratios of 1.2-1.4 [19-21,45]. It was believed that such smaller balloons are likely to provide good relief of pulmonary valve obstruction while at the same time may prevent significant PI at late follow-up. However, careful long-term follow-up studies are necessary to corroborate that this modification in balloon size will indeed prevent late-onset PI [8,23].
Comparison with Surgery
The comparison of balloon valvuloplasty with surgical pulmonary valvotomy is challenging because: 1. Extremely few or no studies exist that compare concurrent balloon and surgical procedures, and there are no randomized studies to address this issue, 2. There are intrinsic problems in comparing “older” historical surgical results with “current” BPV, and 3. There is a relatively short duration of follow-up after BPV. In the past, the author compared the outcomes of surgery from nine papers with those of BPV in 11 publications [4]. In the surgical group, 46 to 234 patients were followed for a few months to 30 years following the surgical relief of PS. The operative mortality varied between 3% and 14%. Poor results, defined as residual PV gradients ≥ 50 mmHg, were seen in 0 to 8% of patients. The multi-institutional natural history study [26] found poor results in 4% of the patients. PI was reported in all studies. In the BPV group, six to 53 patients were followed for one week to 34 months after BPV; no mortality was reported. The reappearance of pulmonary valve obstruction varied between 14% and 23
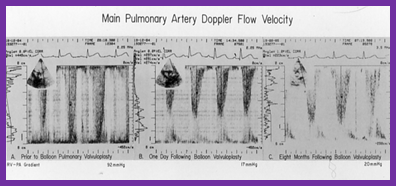
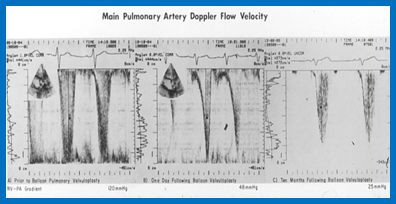
In the beginning, cardiac catheterization (Figure 15) was used to assess the follow-up results of BPV. Following the demonstration of the efficacy of echo-Doppler studies in quantifying the residual gradients [4,75,78], echo-Doppler studies were used almost exclusively by most investigators in the assessment of the results of BPV at follow-up. In 1989, the author reported follow-up echo-Doppler studies of 50 children, 3 to 36 months after BPV [42,59]. The peak Doppler flow velocity (Figure 41) was used to calculate the peak instantaneous Doppler gradient using a modified Bernoulli equation (Figure 42). There was reduction (p < 0> 0.1). There was excellent correlation (r = 0.9) between cardiac catheterization-measured and Doppler-derived gradients at follow-up [42,59].
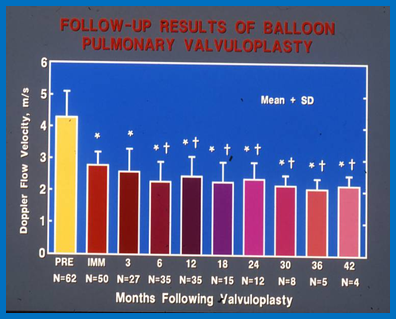
Cardiac catheterization is no longer performed for the evaluation of residual gradients, but may be undertaken if catheter re-intervention is contemplated. The assessment of the immediate, intermediate-term, and long-term results of BPV by echo-Doppler studies in terms of residual gradients (Figures 16,17,21,23,41, and 42), ventricular dimensions (Figure 25), degree of pulmonary insufficiency (Figure 26 and 43 ), and interventricular septal motion (Figure 27) was demonstrated in Figures 16,17,21,23,25-27 and 43). Based on these observations, it may be concluded that echo-Doppler studies are excellent tools in the follow-up evaluation of BPV.
Balloon Valvuloplasty in Specific Age Groups
The above review included discussion of BPV which are mostly focused on infants, children, and adolescents. In the ensuing sections the results of BPV in the fetuses, neonates, and adults will be reviewed.
Pulmonary Stenosis/Atresia in the Fetus
Prenatally diagnosed critical PS and pulmonary atresia with intact ventricular septum (PAIVS) carry poor prognosis for postnatal biventricular repair. The extent to which simple BPV in the fetus prevents severe RV hypoplasia is not clearly understood [82]. The rationale behind using fetal BPV is to establish antegrade flow across the pulmonary valve; augment ventricular filling; decrease tricuspid insufficiency; improve RV diastolic function; and increase normal division of myocardial cells through the remaining fetal life, thereby improving growth of the RV. Hopefully, such interventions increase the chances of a biventricular outcome. The indications for fetal BPV are not clearly established; critical PS or PAIVS in the fetus with signs of impending or near hydrops are suggested indications, but with the intent of producing biventricular outcomes. Nearly one-third of cases of PAIVS in utero may have coronary arterio-venous (CAV) fistulae and fetuses with small, unipartite RVs and those with RV dependant coronary circulation (RVDCC) are not candidates for relief of RV outflow obstruction. But, babies with small CAV fistulae and a reasonable sized RV may undergo the procedure. Some investigators developed criteria to predict single ventricular outcome [83]; if three of the following four criteria are present, single ventricular outcome is likely: 1. Tricuspid/mitral valve ratio <0>
The procedure of BPV is usually performed between 21 to 30 weeks of gestation. Maternal general anesthesia is usually used. Although general anesthesia imposes certain risks to the mother, it facilitates re-positioning the fetus to an appropriate lie to assist performing BPV. Fetal anesthesia and paralysis are induced by fetal intramuscular injection of atropine, vecuronium, and fentanyl. The technique of accessing the fetus is similar to that used by Daffos and associates [85] for chorionic villous sampling. A 16 to 19 gauge needle is introduced under ultrasound guidance trans-cutaneously via the maternal abdominal wall and uterus and then across the fetal chest (or subcostal) into the RV outflow tract. A floppy-tipped 0.014" coronary guide wire is used to cross the PV. Once the position is confirmed by fetal ultrasound, a coronary balloon angioplasty catheter with a balloon diameter larger than pulmonary valve annulus (B/A ratio of 1.2 to 1.3) is positioned across the pulmonary valve and the balloon inflated at the manufacturer's recommended pressure. If the percutaneous route is not successful, the uterus is exposed with a mini-laparotomy
In an early publication by Tulzer and colleagues [86], the authors reported two fetuses who had fetal BPV at 28 and 30 weeks’ gestation, respectively. Both babies had successful opening of the pulmonary valve with decrease in the degree of tricuspid insufficiency and improved RV function and were delivered at 38 and 35 weeks, respectively. However, both babies required post-natal BPV and aorto-pulmonary shunts. Nonetheless, both babies eventually achieved biventricular circulation. Subsequently, a number of other investigators reported their experiences and results of fetal BPV with one to 2 cases [84, 87-90] as well as larger case series [91-93]. In the larger case studies, 5 to 23 fetuses had BPV at a median of 24 to 28 weeks gestation [91-93]. The procedural success varied between 60 and 100%; deaths related to the procedure were not seen and but some complications (pericardial effusion and bradycardia) occurred. In successful cases, larger RV caused by reduced afterload and increased filling occurred, thus improving the likelihood of biventricular outcome. Despite initial improvement, several babies developed progressive restenosis requiring repeat fetal BPV or early delivery. Most babies required postnatal BPVs and aorto-pulmonary shunts. Postnatal outcomes varied with biventricular outcomes in most, one-one-half ventricular outcomes in a few, and single ventricular outcome in a few [91-93]. While the data is limited, fetal BPV appears safe and effective.
Critical Pulmonary Stenosis in the Neonate
The term ‘critical PS’ is generally reserved to describe very severe PV stenosis resulting in supra-systemic right ventricular systolic pressure, a right-to-left atrial shunt across the PFO, ductal-dependent pulmonary blood flow, or a combination thereof. The author has reviewed transcatheter management of critical PS in multiple publications in the past [4,43,94-99], and will only be examined briefly here. Neonates with obstruction that is less than severe/critical should undergo BPV later, past the newborn period [98,99]. Tynan and his colleagues [100] extended the BPV technique of Kan [10] to neonates with critical PS. The procedure of BPV in neonates is similar to that used in older children, with some exceptions. These babies usually require prostaglandin E1 (PGE1) infusion to increase systemic arterial oxygen saturation and to decrease the complications associated with BPV. The procedure of traversing the PV and positioning the balloon dilatation catheter across the PV is slightly more difficult than that encountered in older children. RV cineangiographic frames from sitting-up (150 LAO and 300 cranial) (Figure 44) and lateral (Figure 45) views serve as guides during the procedure to ensure the correct position of the guide wires, catheters and balloons.
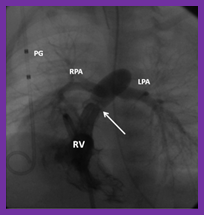
A right coronary artery (Cordis), angled Glidecath (Meditech) or cobra (Cook) catheter (usually #4 French), according to the cardiologist’s preference, is placed in the RV outflow tract and a floppy-tipped coronary guide wire is passed across the pulmonary valve. The guide wire is then advanced into either branch pulmonary artery or into the descending aorta via the patent ductus arteriosus (Figure 4); the author prefers the latter because of the improved stability of the guide wire which in turn facilitates positioning a suitable sized balloon catheter across the pulmonary valve. The catheter in the RV outflow tract is advanced over the guide wire, across the pulmonary valve, and into one of the branch pulmonary arteries or the descending aorta. The coronary guide wire is exchanged with a guide wire that is appropriate for the selected balloon valvuloplasty catheter. If it is not possible to advance the catheter across the pulmonary valve, balloon dilatation with smaller balloon catheters (3-4 mm diameter coronary angioplasty balloon catheters) may be performed prior to using the appropriate-sized balloon catheter (Figures 5 and 46). If an appropriate-sized balloon catheter can be passed across the PV, BPV is performed in a conventional manner (Figure 4). The selection of balloon size for BPV is the same as that used for children (B/A Ratio of 1.2 to 1.25), as discussed in the preceding sections.
The results are generally good, with a reduction in the pressure gradient across the pulmonary valve, RV peak systolic pressure and RV to aortic systolic pressure ratio, and increased flow-width across the pulmonary valve demonstrated by angiography. Despite the improvement in the pressure gradients, some patients require continued infusion of PGE1 thought to be related to decreased compliance of the RV. Aorto-pulmonary (modified Blalock-Taussig) shunts or ductal stents are used by some investigators as an alternative to prolonged PGE1 infusion. For additional discussion of the immediate and follow-up results, the reader is referred our prior publications [4,43,67,94-99].
Pulmonary Stenosis in Adult Subjects
Following Kan's report [10] of BPV in children, Pepine and his associates [101] applied this technique in an adult patient and produced good results. Subsequently other groups of cardiologists [58,102-105] used this procedure to relieve pulmonary valve obstruction in adults.
The technique of balloon pulmonary valvuloplasty is essentially similar to that used in children, however, because of physical size of the pulmonary valve annulus, some adults may need simultaneous use of two balloons for balloon valvuloplasty [58,102]. However, more recently, larger diameter balloons became available for clinical use and therefore, double balloon technique is not necessary in all cases. In addition, as discussed above (Number of Balloons section) and elsewhere [20,56], the double balloon technique is similar to but not superior to the single balloon method, especially when equivalent B/A ratios are used. Subsequently, Inoue balloon were used in adults [103,106,107] with good results. The chief advantage of the Inoue balloon over the conventional balloons is that the balloon diameter can be increased, making stepwise dilatation feasible. Balloon sizes similar to or 1 mm larger than PV annulus were used in adults which seems to be effective [44,104,105]. But, systematic evaluation of the influence of B/A ratios in adult subjects has not been performed. As stated in the section on Balloon Diameter, I would suggest a B/A ratio of 1.2 to 1.25 in adults also.
Immediate results of balloon valvuloplasty in adult patients are excellent [4,44,58,101-107] and are similar to those observed in children. Good results has been seen even in the sixth and seventh decades of life [107-109].Infundibular obstruction may develop after balloon valvuloplasty; such problem has been shown in teenage [66,68] and adult patients [58,105]. Infundibular obstruction appears to be more common in older patients than in younger patients [68]; this is probably related to long-standing right ventricular hypertension with resultant right ventricular infundibular hypertrophy in older patients [68]. However, the infundibular obstruction tends to resolve with time [68,69] after balloon valvuloplasty, as reviewed in the section on Infundibular Obstruction.
Results at follow-up, though reported in a few studies, do signify persistent relief of pulmonary valve obstruction. It may be concluded that that successful balloon pulmonary valvuloplasty is possible in adult patients and we recommend balloon valvuloplasty as preferred treatment option for management of PS for this group of patients also [1].
The Mechanism of Valvuloplasty
Inflation of a balloon placed across the stenotic pulmonary valve applies radial forces on the stenotic pulmonary valve without any axial component [42,110,111]. The mechanism of valvuloplasty has been evaluated by direct inspection of the valve at surgery [112] and of postmortem specimens [113]. It has also been studied by indirect examination of angiographic [42,114] and echocardiographic [115] changes following BPV. Splitting of the valve commissures, tearing of valve leaflets and avulsion of the valve leaflets have been seen in all these studies and are possibly the mechanism by which pulmonary valve stenosis is relieved by balloon valvuloplasty. The radial dilating force exerted by balloon inflation is likely to rupture/tear the fused valve commissures, the weakest part of the valve mechanism. But, in some patients, if the fused commissures are too strong to be torn, valve cusp tears and even avulsion of valve leaflets may occur. The latter events are likely to produce severe PI. In patients with pulmonary valve dysplasia, successful balloon valvuloplasty may not be possible unless there is associated commissural fusion. For a more detailed discussion of mechanism of balloon valvuloplasty, the reader is referred to detailed discussion presented elsewhere [111].
Right Ventricular Filling and Compliance
Right ventricular filling abnormalities and decreased compliance of the RV muscle are expected to be present in children with RV outflow tract obstruction in a manner similar to those of the left ventricle in patients with left ventricular outflow obstruction. Indeed such abnormalities were demonstrated by Vermilion and colleagues [116]; there was decreased RV filling in early diastole and increased filling during atrial contraction. But, their findings suggested no change in the RV filling abnormalities and compliance characteristics following successful BPV [116]. However, these findings are at variance with our clinical observations. Consequently, we investigated this issue with the help our patient data [117]. Of the 75 patients who underwent balloon pulmonary valvuloplasty, 10 children had arterial desturation secondary to right to left shunt across the PFO. Peak to peak pulmonary valve gradients were reduced from 118 ± 38 mmHg to 28 ± 17 mmHg (p<0>
Improved O2 saturation following BPV is related to abolished or reduced right to left shunt across the PFO. Th Role of Balloon Pulmonary Valvuloplasty in the Management of Pulmonary Stenosise only difference between pre- and post- valvuloplasty states is decreased pulmonary valve gradients, thereby reducing RV afterload. This decreased RV afterload may have enhanced RV filling with resultant reduction in right to left shunt. Perhaps the Doppler recordings [116] are not sensitive enough to detect improved RV filling after BPV [117].
Pulmonary Stenosis Associated with Other Heart Defects
Introduction.Cyanotic congenital heart defects (CHDs) constitute 20-25% of all CHDs. In a subgroup of cyanotic CHDs, obstruction to the pulmonary blood flow by a stenotic pulmonary valve causes arterial oxygen desaturation, and transcatheter management of these will be reviewed. The defects in this group are tetralogy of Fallot (TOF), transposition of the great arteries (TGA), double outlet right (or left) ventricle, double-inlet left ventricle, tricuspid atresia, ventricular inversion (congenital corrected transposition of the great arteries {CCTGA}) and other types of univentricular hearts, all with non-restrictive inter-ventricular communication and severe pulmonary valve stenosis. These patients are usually symptomatic in the neonatal period or early in infancy. The pathologic, pathophysiologic, clinical, chest x-ray, ECG, echo-Doppler and angiographic features of cyanotic CHD were discussed by the author elsewhere [7,118,119] and will not be reviewed here. Total surgical correction is feasible in some of these patients [7,118-120] while in others, complete surgical correction is not possible. In the latter group of patients, surgical palliation to augment the pulmonary blood flow with aortopulmonary shunts [121,122] is a standard management approach. Following the report by Kan and her associates [10], we applied the BPV technique, initially to isolated PS cases [64,65], as reviewed in the preceding sections of this paper, and subsequently extended the technique to cyanotic CHDs [123-125]. In this section, issues related to BPV in cyanotic CHDs will be reviewed.
Indications for BPV in Cyanotic CHD. The indications for BPV are cyanotic cardiac defects which are not amenable to surgical correction either due complexity of the defect or to the size of the patient at the time of presentation, but nonetheless require palliation for pulmonary oligemia. In older children, symptoms related to hypoxemia and polycythemia are indications for such interventions. Hypoplasia of the pulmonary valve ring, main, and/or branch pulmonary arteries is another indication, even if symptoms are absent.
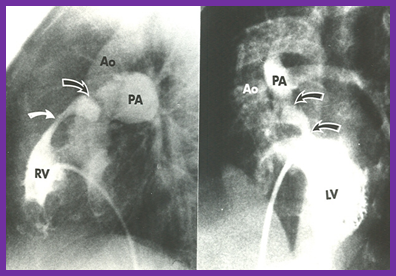
The presence of two or more sites of obstruction (Figures 48 and 49) is considered a prerequisite when employing balloon valvuloplasty [123,124]. The reason that we adopted this principle is because if valvar PS is the sole obstruction, relief of such an obstruction may produce a marked increase in the pulmonary blood flow, the elevation of pulmonary artery pressure, and pulmonary vascular resistance. In the presence of two obstructions in series, the relief of one obstruction decreases the total resistance to flow into the lungs, with the resultant relief of pulmonary oligemia; yet the pulmonary artery pressures remain normal (Figure 50).
Procedure of Balloon Pulmonary Valvuloplasty. The technique of BPV is essentially similar to that used for isolated valvar PS and is described in detail elsewhere [124-129]. In brief, a # 4- or 5-French multi A-2 catheter (Cordis) or a similar catheter is advanced across the PV and is positioned in the distal branch (left or right) of the pulmonary artery. A suitable-sized (0.014 to 0.035”) flexible tip J guide wire is positioned in the distal left or right pulmonary artery via the catheter already in place, and the catheter is removed. A balloon angioplasty catheter is then positioned across the pulmonary valve and the balloon is inflated (Figures 51 & 52). The diameter of the balloon is selected to be 1.2-1.25 times that of the pulmonary valve annulus (although this used to be 1.2-1.4 in the past), as discussed in a preceding section of this paper. One or more balloon inflations are usually performed. Ten to 15 minutes after BPV, systemic arterial saturation, adequate oxygen saturation data to enable the calculation of systemic and pulmonary flows, pulmonary artery and/or right (or left in TGA patients) ventricular angiography, and pressure pullback across the pulmonary valve and infundibulum (Figure 50) are recorded.
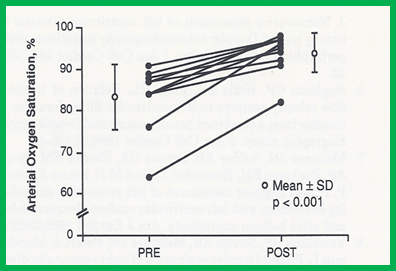
Immediate Results. The immediate results of BPV in cyanotic CHDs were presented by the author in the late 1980s, with the subsequent publication of the immediate results from a larger group of patients [122-127]. The diagnoses in these 14 patients were TOF in ten patients, TGA with VSD and valvar and subvalvar PS in three, and dextrocardia and ventricular inversion with VSD and valvar and subvalvar PS in the final patient. The systemic arterial oxygen saturation (69.9 ± 11.5% vs. 81.4 ± 12.3 %; p < 0>
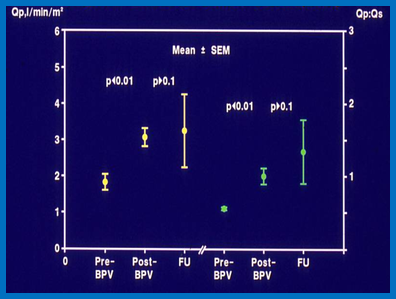
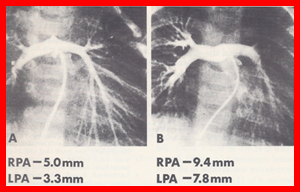
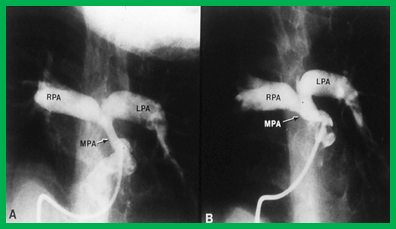
Follow-Up Results. Follow-up cardiac catheterization at six to 36 months (13 ± 10 months) after BPV revealed a persistent increase in the systemic arterial oxygen saturation (82 ± 9%), pulmonary blood flow and Qp:Qs (Figure 53). These values remained essentially unchanged (p > 0.1) from the immediate post-BPV values and continued to be better (p < 0> 0.1). An increase in the size of the pulmonary arteries (Figures 54 and 55) occurred. Six children with TOF had successful surgical correction four to 24 months (12 ± 9 months) after BPV. Four of these children were thought to have very small pulmonary arteries (prior to BPV) and considered not suitable for total surgical correction at that time. Two children with TGA had Blalock-Taussig shunts, which led to improvement. The remaining children were clinically doing well and awaiting further surgery at the time of our report [125].
Comments. The successful palliation of pulmonary oligemia in patients with cyanotic CHDs is feasible by BPV; this procedure may be performed in lieu of a conventional Blalock-Taussig shunt. The growth of the pulmonary arteries that we and others observed is similar to that seen following the Brock procedure and systemic-to-pulmonary artery shunts. Consequently, the author recommends BPV in these patients if the pulmonary artery size is marginal for undergoing surgical correction. In view of the current state of the art, with the feasibility of surgical repair at a younger age, it is prudent that BPV is performed in selected patients with tetralogy of Fallot or other cyanotic defects in concert with a surgical colleague’s opinion regarding the feasibility of complete repair at a given age and state of the pulmonary arterial anatomy. There is also some controversy as to whether the BPV procedure causes significant growth of the pulmonary valve annulus [130,131]. It should also be noted that this technique has been extended [132] successfully to a group of children with truly diminutive pulmonary arteries.
In view of these diverse observations, as alluded to in the preceding paragraph, the author concludes that not all cyanotic CHD patients with PS are candidates for BPV, and suggests that BPV is undertaken in selected patients. The criteria that must be met in such cases are: 1. The infant/child requires palliation of pulmonary oligemia but is not suitable for total surgical correction because of the size of the patient, the type of the defect or other anatomic abnormalities, 2. The valvar obstruction is a significant component of the RV outflow tract obstruction, and 3. Multiple obstructions in series are present so that there is residual subvalvar obstruction after the relief of PV obstruction, such that flooding of the lungs is prevented. Additional indications are the presence of contraindications for open heart surgery, or refusal of consent for open heart surgical correction by the parents/guardians [128,129].
Other RV Obstructive Lesions.
There are a number of RV obstructive lesions that may need treatment and these include, intracavitary right ventricular outflow obstructions (isolated infundibular stenosis, double-chamber RV, and hypertrophic cardiomyopathy involving the RV), subpulmonary obstructions in the morphologic left ventricle in patients with CCTGA (secondary to muscular mal-alignment, fibro-muscular ridge {similar to the sub-aortic membrane that is normally located in the left ventricle}, aneurysm of the membranous septum, and intra-cardiac blood cyst, etc.), supravlavar pulmonary artery stenosis (congenital or acquired), external compression causing supravalvar PSfollowing the Nuss procedure, and branch pulmonary artery stenosis. Some of these require medical/surgical interventions and others may be benefited by transcatheter therapy and will not be reviewed in this paper but were addressed elsewhere [1,67,133] for the interested reader.
Summary and Conclusions
Since the initial description of BPV by Kan and her associates in 1982, the procedure has been widely used by many cardiologists for treatment of valvar PS. We recommend that the procedure be performed for peak-to-peak systolic pressure gradients in excess of 50 mmHg, although some cardiologists use 40 mmHg as an indication for BPV. Obstructions which are severe and critical, irrespective of age and pulmonary valve dysplasia, should undergo balloon valvuloplasty at the time of presentation. The BPV procedure entails placing one or more balloon angioplasty catheters across the stenotic valve over an extra-stiff guide wire(s) and inflating the balloon(s) two or more times. The radial forces of balloon expansion produce valvotomy. The currently recommended B/A ratio is 1.2:1 to 1.25:1. Immediate reduction of systolic pressure gradient, increase in width of the stenotic jet, and free motion of the pulmonary valve leaflets with less doming have been observed following balloon valvuloplasty. Right ventricular function improves, tricuspid insufficiency gets better, and right-to-left shunt across the atrial septum is abolished or decreases. Complications are rare with a prevalence of 0.35%. At intermediate-term follow-up, peak-to-peak systolic pressure gradient reduction is seen both by catheterization and Doppler-studies for the group as a whole. Yet, restenosis, defined as gradient ≥ 50 mmHg, has been observed in nearly 10% of children. Late follow-up results are scanty. But the available data indicate excellent results with low pulmonary valve gradients and minimal additional restenosis beyond what was observed at intermediate-term follow-up with event-free rates of high-80s and mid-80s at 5 and 10 years after valvuloplasty, respectively and significant increase in the prevalence of PI.
BPV is also useful in the fetus, in the neonate, in children with dysplastic pulmonary valves, in patients with pulmonary valve stenosis associated with other heart defects, and in adults with PS. Mechanism of valvuloplasty was investigated and it appears that the radial dilating force exerted by balloon inflation is likely to rupture/tear the fused commissures. Right ventricular filling abnormalities appear to improve after balloon valvuloplasty, resulting in reduction of right to left shunt across the atrial septum. Predictors of restenosis were investigated and were found to be B/A ratio < 1>
Regression of right ventricular hypertrophy on ECG occurs after balloon valvuloplasty and the ECG is a useful adjunct in the evaluation of results of balloon dilatation. But, ECG evidence for improvement does not become obvious until six months after balloon dilatation. Doppler gradients are generally reflective of residual obstruction, can detect PI and echo-Doppler studies are useful and reliable non-invasive monitoring methods.
Infundibular gradients occur in nearly 30% patients; higher prevalence is noted in the older patients and in those with severe obstruction. If the residual infundibular gradient is ≥ 50 mmHg, beta blockade therapy is recommended. The infundibular obstruction regresses at follow-up to a great degree with only occasional patient requiring surgery. Residual PI is present in the most patients at late follow-up; in most studies surgical intervention was not required. However, a few studies show significant PI to require pulmonary valve replacement. Decreasing the B/A ratio to 1.2 to 1.25 at the time of initial BPV may reduce the PI at follow-up. Studies comparing balloon with surgical treatment are scanty. Surgery is associated with higher incidence of mortality and morbidity and of PI, but with a greater reduction of gradient.
In conclusion, BPV is the treatment of choice for relief of pulmonary valve stenosis in the fetuses, neonates, children and adults. Use of balloons 1.2 to 1.25 times larger than PV annulus may produce optimal results. Fifteen-to-twenty year follow-up studies to 1. Identify the significance of residual PI and 2. If reduction of B/A ratio to less than 1.25 has any beneficial effect in reducing late PI are recommended.
Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.









































