AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Varsha Ojha, Specialist Obstetrics and Gynecology, Prime Hospital, Dubai UAE.
Citation: Ojha V, Vinod K. Singhal, Khanna S., (2024), Robotics in Gynecology- A Review, J. Obstetrics Gynecology and Reproductive Sciences, 8(5) DOI:10.31579/2578-8965/224
Copyright: © 2024, Varsha Ojha. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 June 2024 | Accepted: 21 June 2024 | Published: 28 June 2024
Keywords: laparoscopic surgery; gynecologic procedures; robotic surgery; robotic surgery
This review article focuses on the development of robotics-based operations in the medical field especially in gynecology. The goal of the surgical robot is to improve surgical skills and compensate for human limitations. The robot's performance in performing duties correctly and consistently has been the key to its success. Tubal anastomosis was the first gynecologic surgery performed with Robotic assistance in 2000 followed by first Robotic Hysterectomy in 2002. In 2003 Da Vinci surgical system was developed which was FDA approved for gynecological surgery in 2005. It has gained popularity fast and is already playing a big part in many of the places where it is available. It consists of a high-resolution three-dimensional (3D) vision system adjacent to the patient on a cart with robotic branches. It provides unique technical advancement, with tremor filtration, improved ergonomics and lower muscular load as compared to both laparoscopic and open surgeries. Autonomous camera and energy instrument control, wrist articulation with 7 degree freedom, telestration and dual- console capabilities, overcoming the limitations of conventional laparoscopy, such as counterintuitive hand movements, 2 dimensional visualization, limited degree of motion and tremor amplification. Compared to laparoscopy, robotic assistance has a lower conversion rate to open procedures. Endo wrist movement of an automated machine during myomectomy surgery can perform proper and better suturing than traditional laparoscopy. The automated program is a noticeable improvement over laparoscopic surgery and, if price issues are resolved, can gain popularity among gynecological surgeons around the globe. Not unique to robotic system, the integration of indigo cyanine green fluorescence with the Da Vinci robotic system allows identification of lesions, and assessment of perfusion of bowel and ureter during deep infiltrating endometriosis resection.
Robotic systems typically consist of three main components: the surgeon console, the patient-side cart, and the vision system. The surgeon console allows for precise control of instruments, the patient-side cart holds the robotic arms, and the vision system provides high-definition, magnified 3D images of the surgical field. The integration of these components allows for unparalleled surgical precision.1
Historical Background
An orthopedic surgeon and his team created the "Arthrobot," a robot that was utilized for the first time in robotic surgery in Canada in 1983. Since then, surgical robots have developed and been applied to numerous surgical specialties, including gynecology, general surgery, ophthalmology, and urology. The next big move came in 1985. Kwoh and his colleagues used the Puma560 robotic arm to aid in performing a brain biopsy under CT guidance.2 With the introduction of PROBOT, the first surgical robot for the prostate, ROBODOC, the first surgical robot for hip replacement.
The ZEUS robot was used to execute the first successful telerobotic procedure, a cholecystectomy, at the start of the twenty-first century. A New York-based surgeon operated on a patient who had received treatment in France.2 Even the Penta-gon was presented with the idea of telerobotics as a safe solution that may allow surgical professionals to heal wounded soldiers on the battlefield without endangering further men. Mobile Advanced Surgical Hospital (MASH) was the project's moniker. The MASH method helped create the momentum for daily practical application in the hospital setting, even if it was never put into practice at the time.3
Over the past 30 years, gynecologic surgeons have added mildly interfering surgery to their surgical repertoire. The development of joint wristed instruments, tremor control, and three-dimensional (3D) stereoscopic vision for advanced tissue viewing and manipulation is one of the many amazing advantages of robot-assisted surgery (RAS).4 In 2005, the widely utilized da Vinci Surgical System received approval from the US Food and Drug Administration (FDA) for a select number of gynecologic procedures. Currently, the system is the only FDA-approved robotics stage available on the market. This particular platform offers several advantages over traditional laparoscopy, including reduced postoperative discomfort, improved surgeon ergonomics, faster analysis of the instrumentation's curve, elimination of the fulcrum effects, and a more organized integration of fluorescence technology for lymphovascular estimation.5
It provides superior visualization thanks to its wrist-like arm movement, high-resolution 3D perspective, and improved ergonomics.6 There is much space for improvement in the surgical performance of robotic surgery beyond the first and second years. Even after a long time, as evidenced by the declining surgical times, the quality of the surgery keeps improving. Robotic surgery should be explicitly contrasted with conventional laparoscopy in order to determine whether the increased direct and indirect expenses are warranted by any benefits in patient clinical outcomes. The increasing acceptance and use of computer-assisted laparoscopic technology raises important considerations about the learning process. Many modalities may be covered in a robotic surgery training course.7
Various robotic systems since then have been developed ranging from multiport , single port , to vaginal access platforms.
Gynecological robotic surgery has a wide range of applications and is expanding quickly. The da Vinci Surgical System is used for malignancies such as ovarian, cervical, or endometrial cancer, as well as benign indications include treatment for fibroids, irregular periods, endometriosis, pelvic prolapse, and ovarian growths. The robotic technology could help the gynecological surgeon with lymph node biopsies, oophorectomies, salpingectomies, hysterectomies, and myomectomies. Thus, it's possible that abdominal surgery will become outdated in the future—science fiction, as we mentioned. Numerous academic institutions worldwide have conducted substantial research on the application of robotic surgery and discovered that it significantly reduces the morbidity and death rates of patients suffering from gynecologic cancers.8
Randomized controlled trials and selective retroactive learning have shown that minimally invasive surgery is associated with lower blood loss, shorter hospital stays, and fewer complications following gynecological cancer staging procedures, such as hysterectomy, myomectomy, sacrocolpopexy, and other surgeries and following surgery, as well as a higher standard of living than with open incision procedures.8 Gynecological robotic-assisted laparoscopic procedures include lymph node dissection, benign hysterectomy, myomectomy, radical hysterectomy, and saccolpopexies. While robot-assisted gynecologic surgery usually results in equivalent clinical outcomes, less blood loss, and a shorter hospital stay than open or laparoscopic surgery, it can occasionally take longer in the operating room.9
After careful analysis, we found that robotic surgery was consistently connected to shorter post-surgical hospitalization when compared to open surgery, a difference less significant when compared to laparoscopic surgery. Also, it seems that robotic surgery is highly feasible in gynecology. There are quite a few inconsistencies regarding operative times and estimated blood loss between the different approaches, though in the majority of studies estimated blood loss was lower in the robotic surgery group. The high variance in operative times resulted from the difference in surgeon’s experience. The decision whether robotic surgery should become mainstream in gynecological surgery or remain another surgical technique in the gynecological surgeon’s toolbox requires quite a few more randomized controlled clinical trials.
Robotic surgery in Benign gynaecological diseases
Hysterectomy
One of the most common gynecological procedures performed worldwide is the hysterectomy, and over time, efforts have been made to simplify and ease its execution through the development of minimally invasive techniques. However, both in India and the United States, the prevalence of open hysterectomy has increased. The emphasis ought to be to do as many laparoscopic or vaginal hysterectomies as possible that are only somewhat disruptive. Better functional results are obtained in terms of a reduction in postoperative sickness and a faster rate of healing. The American Association of Gynecologic Laparoscopy promoted the use of laparoscopy or extra vaginal access for many hysterectomies performed for benign diseases.10
Although hysterectomy involves slightly more involved techniques, RAS is not frequently performed or accepted in gynecological surgery. This is most likely due to its technological complexity and the necessary steep learning curve. When a robotic platform is presented, there are high rates of robotic hysterectomy and low rates of abdominal Hysterectomy.It is not unexpected that the adoption of mechanical techniques for gynecological surgery, particularly uterine excision, has progressed more quickly in recent years than laparoscopic procedures. However, RAS for benign gynecological sickness demonstrated that it increased the procedure's cost rather than its performance.11
Initial studies where surgeons were early in their learning curve reported longer operative time for Robot assisted hysterectomy , but later with increased training there is no difference in operative time .
Most clinical results such as loss of blood, difficulties, and clinical rest, were comparable to the robot-assisted and laparoscopic hysterectomy. Vaginal hysterectomy (VH) appears to be preferable to laparoscopic hysterectomy (LH) and abdominal hysterectomy (AH) among women having a hysterectomy for benign illness because it is linked to a quicker return to regular activities. Vaginal hysterectomy should be used instead of AH if it is technically possible due to more rapid postoperative healing and fewer febrile event. Laparoscopic hysterectomy provides several benefits over AH in situations when VH is not feasible (including more fast recovery and more occasional hot events and injury and abdominal wall infections). Still, these are offset by a longer operating time. The most popular forms of therapy for endometrial and cervical malignancies in their early stages are total and radical hysterectomies. Open surgery, laparoscopy, and, nowadays, marginally interfering robot-assisted surgery are examples of surgical methods.12
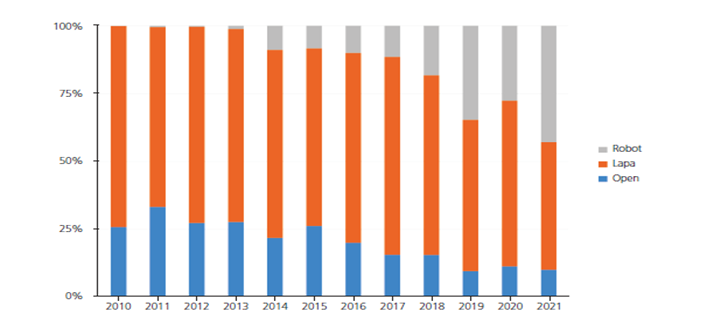
According to a multicenter study in Korea in 2021, robotic assisted hysterectomy accounted for 43% of all hysterectomies, showing a significant increase from 11% reported 5 years ago with a 4.6-fold increase in the total number of surgeries.13
Swenson et al.14 found that the rate of post-surgical complications was lower in the robotic surgery group (3.5% versus 5.6%, P=0.01), including lower rates of surgical site infection (0.07% versus 0.7%, P=0.01) and need for blood transfusion (0.8% versus 1.9%, P=0.02). Major post-surgical complications such as intraoperative bowel and bladder injury, readmissions, and the need for reoperations were similar between groups. Thus, robotic hysterectomy did not decrease major morbidity following hysterectomy for benign indications when compared to laparoscopic hysterectomy. Though total complications were lower, in the absence of substantial reductions in clinically and financially burdensome complications, it seems that hysterectomy for benign indications via robotic technique is not clinically superior or cost-effective.
Estimated blood loss and length of post-surgical hospitalization were reduced with robotic hysterectomy in three out of four studies (P<0>
Deimling et al.16 carried out the lone RCT to date comparing robotic versus laparoscopic hysterectomy for benign reasons. A total of 72 patients were assigned at random to each surgery arm. For the robotic hysterectomy group, the mean operation time was 73.9 min (median 67.0 min; interquartile range 59.0–83.0 min), while for the laparoscopic hysterectomy group, it was 74.9 min (median 65.5 min; interquartile range 57.0–90.5 min). The study found that robotic hysterectomy was not more time-consuming than laparoscopic hysterectomy when carried out by a surgeon skilled in the selected procedure.
Myomectomy
Currently Myomectomy is mostly performed via laparotomy , but several systematic reviews comparing robotic and open myomectomy also report lower blood loss , short hospital stay , less pain and complications.lavazzo and colleagues reported no difference in complications , operative time , blood loss and post operative fertility between RAS and laparoscopic myomectomy. Wang and colleagues found fewer conversion to open surgeries which was 4 times high in laparoscopic myomectomies and lower complication rates. A 2021 systematic review reports no difference in fertility , pregnancy outcome in robot assisted myomectomy as compared to open surgery. Although further data is needed but Robotic myomectomy can be considered in future as an equal or improved option.
Endometriosis-
Laparoscopy surgery for endometriosis is challenging. The surgeon is under increased pressure to perform an exacting and comprehensive procedure due to adhesions, disturbed anatomy of adnexal tissues, and low reproductive outcomes. Female endometriosis patients typically experience severe cramps with heavy bleeding, prolonged pelvic pain, subfertility, heavy menstrual bleeding, and abdominal bloating. These symptoms are usually incapacitating and require special care during surgery to replace anatomy and function while all endometriotic implants are removed. However, following endometriosis laparoscopic surgery, space is typically regarded as a surgical accomplishment.,with Robotic platform, it is possible to overcome the space and provide the surgeon with an expanded and comprehensive operative view.17
With the exception of a longer operating duration, there was no discernible difference between RAS and standard surgery for endometriosis in terms of blood loss, clinical rest, or challenges. There was not a laparoscopy transformation observed. Notably, no adjustments are needed, and the robotic viewpoint might be more effective in intricate procedures involving particular organ compromises. Segmental bowel operations, nodule extraction from the recovaginal septum with or without rectal shave, and partial bladder procedures are among the documented roles of RAS in deeply infiltrated endometriosis. Anastomotic discharge was observed, but no specific perioperative complications have been reported. One of the longest robotic procedure series available for deep infiltrating endometriosis (DIE) is
The RCT (LAROSE trial) compares Robotic assisted surgery with traditional laparoscopy for resection of endometriosis in 73 patients found no difference in operative time, blood loss, intraoperative or postoperative complications or rate of conversion to laparotomy, with improved Quality of life.
A combination of laparoscopic surgery and the da Vinci system has been used to treat colorectal endometriosis in some infertile female patients with severe small intestine disorders. Every patient has demonstrated operating margins free of disease. Ureteroneocystostomy and automated laparoscopic restricted ureterectomy were used to treat endometriosis-related ureter obstruction. There have also been reports of a few patients receiving successful treatment for endometriosis of the bladder, ureter, and small intestine by robotic laparoscopic surgery.
Robotic-assisted surgery for endometriosis is demonstrated to be possible; however, it hasn't been established that it is any better than traditional laparoscopy. Fluorescence and narrow band imaging are two other advanced imaging methods that have been researched. However, long-term clinical advantages have yet to be demonstrated.19 Robotic technologies may be used in endometriosis surgery in particular circumstances. These circumstances include heterogeneity of lesions, which makes it difficult to identify them, difficulties in precisely forecasting surgical complexity, and extended OT times for severe patients.
Robot-assisted laparoscopy (RAL) is a significant advancement that has created new avenues for the treatment of endometriosis, especially Deeply infiltrating lesions . It provides a number of technological benefits in the techniques for managing this difficult condition, like tremor filtering, 3D vision, and improved surgical ergonomics, all improve surgical outcomes without increasing operating times, causing blood loss, increasing intra- or postoperative problems, or increasing the likelihood of laparotomy conversion. More prospective studies are required to further evaluate outcome and better define the role in endometriosis.9
In order to compare the safety and effectiveness of robotic surgery to laparoscopic surgery for the treatment of advanced-stage endometriosis, Chen et al.20 carried out a meta-analysis. Only two studies could be included because there were no appropriate clinical trials. In terms of post-surgical hospitalization, complication rate, and estimated blood loss, no discernible variations were seen between the two groups. The robotic surgery group's mean operation time was longer (73.85 min, P<0>
Sacrocolpopexy
Pelvic organ prolapse is the leading source of morbidity in women, and an increasing number of them are opting for surgical therapy rather than living with pain and humiliation. Between 0.2% and 45% of cases of vaginal vault prolapse have been reported. The experience of the surgeon plays a big role in figuring out what to do. The patient's expectations for the procedure, age at presentation, prolapse grade, and surgical fitness all affect which procedure is made available to them. Abdominal sacrocolpopexy with mesh has the highest long-term success percentage of any operation. Patients with pelvic organ prolapse who are generally in good health can recuperate rapidly with robotic-assisted laparoscopy.21
However, the benefits of robotic assistance include reduced blood loss and shorter clinical rest periods. The main advantages of the mechanical approach are improved eyesight and talent, particularly once the pre-sacral area is divided and the mesh is the intracorporeal sutures are put. The employment of a robot during laparoscopic surgery facilitates the successful completion of difficult tasks and yields favorable outcomes. One advantage of robotic sacrocolpopexy is that it simplifies intracorporeal suturing. Either the suturing or the entire procedure may be mechanically assisted. In this process variation, they were contrasting with the operative time.21
The benefits of these expensive procedures are still unclear, despite a rise in the use of robotic technology for minimally invasive hysterectomies with sacrocolpopexy. A comparison of robotic and traditional surgery revealed differences in costs, 30-day readmission rates, and perioperative problems utilizing a global database to facilitate laparoscopic hysterectomy and concomitant sacrocolpopexy. Pelvic floor disorders are a major risk to public health. Sacrocolpopexy is the most effective treatment for female vaginal prolapses. The relatively new and efficient laparoscopic ventral mesh rectopexy treatment can be used to treat rectal prolapse. The two robotically assisted procedures have not been combined in any literature.22
Laparoscopic and robot-assisted sacrocolpopexies appear to be just as successful as abdominal sacrocolpopexies; nevertheless, future prospective studies contrasting the long-term effects of abdominal sacrocolpopexy (ASC), laparoscopic sacrocolpopexy (LSC), and robotic sacrocolpopexy (RSC) with medical expenses are urgently needed. Selection of the right surgical approach is a complex decision process involving many factors.23 Pelvic organ prolapse (POP) is a common condition that drastically reduces women's quality of life. Practical support for the vaginal apex is a vital component of an efficient surgical repair for women with severe prolapse, including anterior and posterior wall prolapse. There are two surgical options: abdominal and vaginal. The former can be performed openly, laparoscopically, or robotically.
A Chochrane review of RCT,s comparing Robot assisted sacrocolpopexy with conventional laparoscopy showed no difference in complications, blood transfusion or conversion, there was a longer operative time , but of low quality evidence.
Robotic Single-port SCX
A study reviewed a state-of-the-art robotic surgical technique, single-port SCX, during which the surgeon operated almost exclusively through a single entry point, leaving only a single small scar. The investigators’ aims were to evaluate the new technique’s learning curve and, in addition, to share tips for improved single-port robotic SCX based on the first 25 patients to have undergone single-port robotic SCX. Median age was 59 years (range 35–74). Median “pelvic organ prolapse quantification” stage was 3 (range 2–4). Median total operative time was 190 min (range 114–308). Median console time was 130 min (range 85–261). A comparison between the first 15 cases and the next 10 cases demonstrated significant reductions in median operative times and console times: 226 min (range 142–308) versus 156 min (range 114–180), and 170 min (range, 85–261) versus 115 min (range 90–270), respectively (P<0>
Robotic surgery in malignant gynaecological diseases
Robotic-assisted surgery has revolutionized the field of minimally invasive surgery, providing enhanced precision, dexterity, and visualization compared to traditional methods. The da Vinci Surgical System, introduced by Intuitive Surgical in 2000, has been at the forefront of this transformation, offering a robotic platform that allows surgeons to perform complex procedures with greater control and accuracy.
Importance in Malignant Gynaecological Diseases
Robotic surgery has become increasingly important in the treatment of malignant gynaecological diseases, including endometrial, cervical, ovarian, and vulvar cancers. These malignancies often require complex surgical interventions that can benefit from the precision and minimally invasive nature of robotic systems. The use of robotics in oncology aims to improve surgical outcomes, reduce morbidity, and enhance patient recovery.
Early Use in Gynaecology- The application of robotic surgery in gynaecology began in the early 2000s, initially focusing on benign conditions such as hysterectomy and myomectomy. The success of these early applications paved the way for the use of robotics in more complex oncological procedures.
Adoption in Oncology- The adoption of robotic surgery in gynaecologic oncology followed the initial successes in benign gynaecological surgeries. By the mid-2000s, robotic-assisted procedures began to be used for the treatment of gynaecologic cancers, offering benefits such as improved lymph node dissection, reduced blood loss, and shorter hospital stays compared to traditional open surgery.
Imaging and Instrumentation- Advancements in imaging technology, such as fluorescence imaging, have further enhanced the capabilities of robotic surgery. Fluorescence imaging can highlight blood vessels and lymph nodes, aiding in the accurate identification and dissection of cancerous tissues. Additionally, the development of more flexible and versatile instruments has expanded the range of procedures that can be performed robotically.
Applications in Malignant Gynaecological Diseases
Endometrial Cancer
Robotic-assisted surgery is commonly used in the treatment of endometrial cancer, particularly for performing hysterectomy with bilateral salpingo-oophorectomy and lymphadenectomy. Studies have shown that robotic surgery for endometrial cancer offers reduced blood loss, shorter hospital stays, and lower complication rates compared to traditional open surgery.
For treating endometrial cancer, MIS is considered the first choice. Two large prospective randomized controlled trials, “laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology group LAP2”, based on gynecologic oncologists in the United States, and “laparoscopic approach to cancer of the endometrium”, based in Australia, New Zealand, Hong Kong, and Scotland, reported that compared to open surgery, laparoscopic surgery reduced the length of stay in the hospital, blood loss, and the number of antiemetics
Cervical Cancer
For early-stage cervical cancer, robotic-assisted radical hysterectomy and lymph node dissection are becoming standard practices. The precision of robotic surgery allows for meticulous dissection of the parametrial tissues and lymph nodes, which is crucial for achieving clear surgical margins and reducing the risk of recurrence.
Studies have shown that robotic surgery outcomes are better than open surgery outcomes, making it an option for patients. However, when choosing a surgical approach for cervical cancer surgery, the LACC trial results can make clinicians rethink the decision to select robotic surgery24. Many clinicians choose radical hysterectomy via laparotomy in light of the results of the LACC trial. As with other diseases, robots have become more common, and robot-assisted approach to cervical cancer trials are being conducted to create results that can compete with this trial. Research is also being conducted in China25.
Ovarian Cancer
Ovarian cancer necessitates staging and typically involves a substantial portion of the abdominal cavity, thus the debulking procedure is time-consuming. However, the prognosis is typically poor, and the majority of patients require adjuvant chemotherapy following surgery. Based on the findings of the INTERNATIONAL MISSION trial26 cytoreductive interval surgery has replaced neoadjuvant chemotherapy in recent years. Depending on the cell type, MIS is also carried out following neoadjuvant chemotherapy if the response is outstanding.
Although less common than for endometrial and cervical cancers, robotic surgery is also used in selected cases of ovarian cancer, particularly for early-stage disease and staging procedures. The ability to perform precise dissections and thorough lymph node assessments makes robotic surgery a valuable tool in the management of ovarian cancer.
Vulvar and Vaginal Cancers
Robotic-assisted surgery for vulvar and vaginal cancers is less common but has been utilized for radical resections and lymphadenectomy. The enhanced visualization and precision of robotic systems can be particularly beneficial in these anatomically complex regions, improving surgical outcomes and reducing morbidity.
Comparative Studies with Traditional Methods
Numerous studies have compared the outcomes of robotic-assisted surgery with traditional open and laparoscopic methods for gynaecologic cancers. These studies generally show that robotic surgery offers comparable, if not superior, outcomes in terms of surgical margins, lymph node yield, and survival rates. Additionally, robotic surgery is associated with lower complication rates and faster recovery times.
Survival and Recurrence Rates
Survival and recurrence rates for patients undergoing robotic-assisted surgery for gynaecologic cancers are generally comparable to those for traditional surgical methods. The precision of robotic surgery contributes to thorough cancer resection, which is critical for long-term outcomes.
Complication Rates and Patient Recovery
Robotic surgery is associated with lower intraoperative and postoperative complication rates compared to open surgery. The minimally invasive nature of robotic procedures leads to reduced blood loss, lower infection rates, and shorter hospital stays. Patients also experience less postoperative pain and quicker return to normal activities.
Benefits of Robotic Surgery
Precision and Minimally Invasive Techniques- The precision of robotic surgery allows for meticulous dissection and suturing, which is especially important in oncological procedures. The minimally invasive nature of robotic surgery results in smaller incisions, reduced trauma to surrounding tissues, and faster recovery times.
Reduced Blood Loss and Recovery Time- Robotic-assisted surgery typically results in less intraoperative blood loss compared to open surgery. This is due to the enhanced visualization and precision of robotic instruments. Additionally, the shorter recovery times associated with minimally invasive surgery lead to improved patient satisfaction and reduced healthcare costs.
Enhanced Surgeon Ergonomics- The ergonomic design of robotic systems reduces physical strain on surgeons, allowing them to perform complex procedures with greater comfort and less fatigue. This is particularly beneficial during lengthy oncological surgeries, where precision and endurance are crucial.
Challenges and Limitations
Cost and Accessibility- One of the major challenges of robotic surgery is the high cost associated with the acquisition, maintenance, and operation of robotic systems. These costs can be prohibitive for smaller healthcare facilities and can limit the accessibility of robotic surgery to patients.
Learning Curve and Training Requirements- Surgeons require extensive training to become proficient in robotic-assisted surgery. The learning curve can be steep, necessitating dedicated training programs and simulation models. This can be resource-intensive and time-consuming.
Technical and Procedural Limitations- Despite the advancements in robotic technology, there are still technical limitations, such as the lack of haptic feedback and the rigidity of instruments. These limitations can pose challenges in certain surgical scenarios and may impact the surgeon's ability to perform delicate tasks.
Future Directions
Technological Innovations- Ongoing technological innovations aim to address the current limitations of robotic surgery. Developments such as improved haptic feedback, smaller and more flexible instruments, and enhanced imaging technologies are expected to further improve the precision and capabilities of robotic systems.
Expanding Access and Affordability- Efforts to make robotic surgery more accessible and affordable include the development of cost-effective robotic platforms and initiatives to integrate robotic systems into more healthcare facilities. Expanding access to training programs and reducing the financial barriers to acquiring robotic systems are also important steps.
Integration of Artificial Intelligence and Machine Learning- The integration of artificial intelligence (AI) and machine learning (ML) into robotic systems holds great potential for the future. AI and ML can provide real-time data analysis, predictive analytics, and decision support, enhancing the precision and outcomes of robotic-assisted surgeries.
Informed Consent and Patient Autonomy- Ethical considerations regarding informed consent and patient autonomy are critical in the context of robotic surgery. Patients must be fully informed about the benefits, risks, and alternatives to robotic surgery to make informed decisions about their care. Surgeons have an ethical obligation to provide transparent and comprehensive information.
Equity in Access to Robotic Surgery- Ensuring equity in access to robotic surgery is a significant societal issue. The high costs and limited availability of robotic systems can create disparities in access to advanced surgical care. Efforts to address these disparities include expanding training programs, developing affordable systems, and implementing policies to ensure equitable access.
Robotic-assisted surgery has significantly advanced the field of gynaecologic oncology, offering numerous benefits over traditional surgical methods. The precision, minimally invasive nature, and improved recovery outcomes associated with robotic surgery have made it an invaluable tool in the treatment of malignant gynaecological diseases. Despite challenges such as high costs and technical limitations, ongoing innovations and efforts to expand access are likely to further enhance the role of robotic surgery in gynaecologic oncology.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
