AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Lurildo R. Saraiva, Titular Professor University Federal of Pernambuco Hospital das Clínicas UFPE Cidade Universitária, Brasil.
Citation: Lurildo R. Saraiva, (2023), Rheumatic Fever in Pernambuco, Brasil. Biomedical Research and Clinical Reviews. 8(1); DOI:10.31579/2692-9406/148
Copyright: © 2023, Lurildo R. Saraiva. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 February 2023 | Accepted: 17 February 2023 | Published: 24 February 2023
Keywords: salivary gland neoplasm; pleomorphic adenoma; submandibular gland; benign
The State of Pernambuco, located in the Northeast of Brazil, is a region with a high level of pauperism in the working class, especially for those who live in slums, and for the peasants, who live in the hinterland (“SERTÃO”) Rheumatic Fever in this population tends to present in its severe form. The present review shows peculiar clinical aspects of this disease, which is still very present in our country.
Rheumatic Fever (RF), better known amongst us with the term Rheumatic Disease (RD), due to the influence of the great master of Brazilian Cardiology, Luiz V. Décourt, who published a classic book on the subject in 1969 [1] - for him, the word “disease” says more about a illness, which can appear even without fever, especially in its typical recurrences – since its appearance amongst us, in the 1940s, it persists as the major cause of cardiac surgeries in Brazil, reaching the percentage of 40% of all of them. As our country has a profoundly unfair and very unequal distribution of income, in the big cities it is seen, above all, in slums and popular neighborhoods, with an accentuated degree of pauperism, and in very poor, isolated communities in rural areas.
The disease is distributed in our patients from five to fifteen years of life in the acute form, silences in youth and again has an important presentation in the third and fourth decades of life, now, in its chronic form, characterized by the presence of mitral or mitral-aortic valve disease symptomatic, in patients seeking valve correction in Cardiac Surgery Services, found throughout the country. There is no exact number of the incidence of RD in the country, but it is assumed that the prevalence is around 5% [2].
The preponderant symptoms, in the different stages of life, are dyspnea, palpitations, wet cough and edema of the lower limbs. Fever that is not very high may appear in younger children, but it does not have the character of a prominent symptom [3]. Abdominal pain is not uncommon, often suggesting acute appendicitis.
Etiopathogenesis
Since the classic description of RD in France, in the 19th century, by Jean Baptiste BOUILLAUD [4] - the author showed that there was more agreement between arthritis of large joints and valve lesions than disagreement, - joining the descriptions of other researchers over the centuries In the 19th and 20th centuries, it is accepted that the disease results from an autoimmune reaction due to infection of the pharynx by group A beta-hemolytic Streptococcus by Rebecca LANCEFIELD, beyond nine days, in a genetically predisposed individual.
Thus, not every patient who has strep throat has RD: only 3% of patients with streptococcal pharyngotonsillitis develop RD, in the presence of epidemic outbreaks, and only 0.3%, in an endemic situation. Amongst us streptococcal skin infection does not seem to be relevant.
What would lead a patient to develop RD? What characteristics would he have? A curious note was made by the London clinician Walter CHEADLE [5] at the end of the 19th century, when he found that his only son had mitral stenosis and his wife had RD – for him, then, there would be a “family predisposition” to the onset of RD. As at that time the so-called “connective tissue diseases” were unknown, most likely, cases of RD would result from these diseases.
The work of great importance on this fact was that of Manoel PATARROYO et al [6], carried out in the city of Bogotá, Colombia, in 1979. The contact of the blood of 41 rheumatic patients with the blood of a multiparous woman allowed the group to identify rheumatic patients “883 +” and others “883-”. As the patient's blood ran out, in New York, ZABRISKIE et al [7], injecting blood samples from Colombian rheumatic patients studied in monkeys, obtained two monoclonal antibodies, 883S19.23 and 256S.10, which, when used with precision, recognized the candidates to have DR in 92% of the time. Later, the same authors identified the D8/17 monoclonal antibody capable of identifying in almost 100% of choreic patients.
As a disease resulting from altered immunity, its symptoms and signs were grouped by Duchet JONES, in 1944, in what the medical literature has always called “Jones' Criteria”, which are periodically changeable, with the last change taking place recently, in 2015 [8]
How is the disease produced? In rheumatic patients, an initial phase is described by alteration in humoral immunity, with the production of autoantibodies by B lymphocytes, which are directed against aggressor antigens, resulting in tissue necrosis in the skin, subcutaneous tissue, joint synovium, in the nuclei of the cerebral base in Sydenham's chorea [9] and in the heart tissue, especially in the valve endocardium of the mitral and aortic valves.
The action of B lymphocytes is carried out through glycoproteins found on the surface of macrophages or antigen-presenting cells, which, like “cups”, having two layers α and β, allow the insertion of an antigenic fragment (epitope ) [10].
It is current knowledge that the amino acids that make up the M protein, - which, crossing the entire cytoplasm and cell wall of bacteria, hatch in the external environment as "fimbriae", - and the fibrillar proteins of the human heart are similar in 45% of the times. On the other hand, the M protein, myosin, actin and tropomyosin of the human heart are shaped like an alpha-helix, thus, whether due to structural homology or the shape of the protein, the possibility of a similar cross-reaction produced against them is evident.
The participation of altered cellular immunity also takes place simultaneously, or at a later stage, by the HLA-DR system, through activated DR4 T helper lymphocytes, in the intimacy of the valve tissue, with a marked inflammatory alteration and production of lymphokines and other inflammatory factors. , which tends to perpetuity, explaining what McCARTY [11] said back in the 1940s: “in some way, the streptococcus inserts itself into the human heart and remains there for a lifetime”, thus, theoretically, RD is incurable.
The participation of the HLA-DR system allowed the authors to identify rheumatic patients by typing activated DR4 T lymphocytes. Luisa GUILHERME et al [12] recognized in Brazil the predominant loci DR7 and DR53 in individuals with rheumatic valvular heart disease, and thus, in the same way, loci DR3 were recognized in India [13], DR2 and DR4 in the United States – DR2 in blacks and DR4 in whites [14] -, DR4 in Saudi Arabia [15], although in Turkey, even in the same city and in the same racial group, disparate results have emerged, as in Ankara, with DR4 [16] and DR11 [17] being identified. Faced with this multiplicity of loci, CARLQUIST and ANDERSON [18] raised doubts about this argument
The most curious aspect of the disease - something that fascinates us - is that there is production of cross-reactive antibodies against bacterial proteins, which have structural homology with the contractile proteins of the human heart, such as myosin, actin, tropomyosin and vimentin, located on the edge of the valves, and of course, against the human heart.
In 1962, and in subsequent years, KAPLAN et al [19], by injecting bacterial macerates into guinea pigs, found antibodies in their blood that were directed against the bacterial M protein and, at the same time, against structures of the human heart and the ocular cornea. of the human being. In 1967, GOLDSTEIN et al [20] working with the carbohydrate layer of the streptococcus, containing N-acetyl-glucosamine, verified an antigen-antibody cross-reaction against the mitral and aortic valves, which structurally contain the same N-acetyl-glucosamine – such antibodies, which turn against cardiac valve proteins, disappear with the debatable “cure” of the disease, but remain perennial, in case it is a real rheumatic heart disease, or, on the other hand, there is permanent production of antibodies against the valve system of the heart of the man with rheumatic stigmata, a fact consistent with McCARTY's statement in 1946. which is to say, again, RD is incurable [1], [11]
Jones Criteria, 2015
Proposed by the author in 1944, it received successive modifications with the evolution of knowledge, and in 2015, after a suggestion by RD researchers in Australia, Latin America and Asia, regions with a high incidence of RD, a new update of these criteria was carried out, with emphasis on Doppler echocardiography, which had already recognized long before, the existence of subclinical carditis [21], revealing valve lesions not perceived with the stethoscope and which tend to reproduce the real valve lesion.
In this context [22], “major signs or manifestations” are considered – arthritis, carditis, chorea, erythema marginatum and subcutaneous nodules – and “minor signs or manifestations” – fever, increased erythrocyte sedimentation, elevated C-reactive protein and first-degree AV block in the ECG. Classically, two major signs or one major and two minor signs allow the diagnosis of initial acute RD and, at recurrences, two major signs or one major and two minor signs or three minor signs make the diagnosis of disease recurrence: they all require that there be at least one patient evidence or history of pharyngeal streptococcus.
In the changes just made, the authors started to consider “low risk populations” in developing RD compared to others of “moderate and high risk”.
Low-risk populations are those with an incidence of acute RD ≤ 2 per 100,000 school-aged children and, for any age, with a prevalence of rheumatic heart disease ≤ 1 per 1000 per year.
Major criteria:

Minor criteria:

ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; Pernambuco, Brazil: there is a population at high risk for the development of RD.
Arthritis – It is the most frequent clinical manifestation of RD, reaching the percentage of 80 to 90%, affecting even small children, as we have shown in a two-year-old girl, decades ago, today a working lady and without complaints linked to the joint system or the heart [23]
Classically, it affects large joints, especially in the lower limbs (knees and ankles), but also in the upper limbs (wrists and elbows), which, in a peculiar way, migrates from joint to joint, without leaving sequelae.
A particularity of rheumatic arthritis is that it responds promptly to the use of acetylsalicylic acid, within 48 hours at most. If this response does not occur, the diagnosis of RD is called into question.
In recent years, we have observed participation in the inflammatory process of the small joints of the hands, above all, also, the complaint of pain involving lower joints of the lumbar spine is not uncommon.
Carditis – found in 65 to 70% of the cases, it is the most worrisome sign of JONES CRITERIA, as it can result in perennial involvement of the heart, characterizing chronic rheumatic heart disease. In RD, there is a predilection for mitral valves producing, in the acute phase, mitral insufficiency (MI) and, later, double mitral lesion or isolated mitral stenosis (MS), including the malignant type, described by ROY et al [24], in India, in 1963, which It mainly affects adolescents under 20 years of age.
Probably, the richness of N-acetyl-glucosamine in the mitral valve or the pressure factor in the left ventricle, justify this tropism for the mitral valve.
In our midst, a child hospitalized with fever, arthralgia and the presence of a gallop rhythm by B3, with a holosystolic murmur detected in the mitral area, will have active rheumatic carditis, until further notice.
Thus, we can even see older children with acute pulmonary edema, a very rare phenomenon in rich countries.
In clinical practice, MI is mild, moderate or severe, but regardless of this classification, choreic movements may be associated with it in the victimized child, i.e., by the presence in brain neurons of the same N-acetyl-glucosamine, with antibody genesis directed against it
In a serious situation, on the ECG we can detect signs of left ventricular overload, with an inverted U wave, an aspect seen only in chronic oro-valvar lesions, noting significant cardiomegaly in the chest radiological study.
Sydenham Chorea – named after the English physician who recognized it as part of acute RD. It is found in Pernambuco about 12% of the time, a much lower percentage than that found in rich countries such as the USA, where it is described in up to 30% of the cases. appear late, weeks after the pharyngeal infection.
Currently, it is accepted that Chorea is the extreme of a syndrome, which ranges from anxious behavior, or even slightly obsessive-compulsive behavior, or restlessness of the lower limbs, going to TOURETTE's disease and, finally, to Chorea [25]. Famous characters like the American painter Andy Warhol had DR, who presented himself in this way.
Historically, it was called “Saint Vitus Dance” because it was confused with a manic attitude of dancing, present in communities in Central Europe, the Czech Republic and Italy, in the Middle Ages, where bystanders danced nonstop, even with lethal success. Authorities of these small communities thought that the dancers were “possessed by the devil”, and the only way to curb this mania was to have them exorcized by the Italian priest Vito, considered a saint and active in northern Italy.
Despite these historical data, we know that in the serious capitalist economic crisis of the 1930s, there were similar dance contests, also endless, as seen in New York and Boston, also with records of deaths in couples, who lived in a situation of deprivation.
Chorea sufferers are hypersensitive, and any physical or psychic damage produced against them, in a tumultuous environment, there is a clear accentuation of uncoordinated and aimless muscular movements. On the contrary, in a calm, soberly lit environment, in psychic stillness, these movements disappear.
Choreic syndrome predominates in females, but regardless of gender, patients easily fall to the ground, breaking plates, cutlery and glasses during meals. Individuals with Chorea have a characteristic handwriting and sometimes suffer from a change in the timbre of the voice. Physical signs of Chorea are restlessness, inability to stick out the tongue, and the so-called “milkmaid's grip”.
Considered as benign, this impression goes against what DÉCOURT [1] has always warned about, as the choreic syndrome can recur, take months, and be accompanied by mitral valve insufficiency. In our midst, despite being accepted as a late sign of RD, it is by no means unusual for us to come across in our wards with girls admitted with the “arthritis, carditis and chorea conjunction”.
Subcutaneous Nodules and Erithema Marginatum – are the least expressive manifestations of RD, being found around 8% - nodules – and 4% - erythema. Similar to the other manifestations, they result from antibodies that act against the carbohydrate layer of the streptococcus, cross-reacting against the keratin of the skin - erythema marginatum - and the subcutaneous nodules result from granulomatous lesions, which develop in the cutaneous dermis, as a result of the same delayed hypersensitivity against streptococcal antigens - Meynert's nodules. A similar mechanism produces the so-called “Aschoff bodies'' in the heart valves and in the intimacy of the myocardium.
With regard to nodules, it has long been accepted that their presence indicates the occurrence of severe valve damage, however, in the LAPA`s Master thesis [26], who studied subclinical rheumatic carditis, the occurrence of these nodules was verified in two cases. From this assumption, we began to admit subclinical carditis as a “micro-expression” of RD, occurring in the same way as RD itself, which would be the “macro-expression”

Figure 1: A poor peasant 12-year-old boy, in the first rheumatic attack, he reveals signs of protein-calorie malnutrition, with the presence of subcutaneous nodules over the thoracic spine. On the echoDopplercardiogram, the presence of moderate rheumatic mitral-aortic insufficiency.
Laboratory Findings 1 -
1. Complete blood count – in acute RD, there is mild hypochromic anemia, and, in the leukocyte formula, the alteration is consistent with a mild bacterial infection, with mild leukocytosis with a shift to the left, drop in eosinophils and monocytosis. In rare serious situations, leukocytosis can reach values above 17,000 l/mm3, with a marked shift to the left.
2. The measurement of anti-streptolysin O levels remains very useful, being the most used anti-enzyme in the clinic. Titers increase at the end of the first seven days of illness, reaching above 250 units, this increase being seen more in adolescents than in children. In about 3% of patients, titers can remain high, without finding a cause for this: curiously, there is a “certain rigidity” of the measured value.
In case of normal antistreptolysin O values, the measurement of anti-deoxyribonuclease B levels is very useful in the diagnosis of active RD. On the other hand, in 40% of choreic individuals, we can find an increase in antideoxyribonuclease B.
3. Serum acute phase reactions – we are particularly interested in erythrocyte sedimentation (ESR), C-reactive protein (CRP) and mucoprotein dosage.
a) Amongst us, erythrocyte sedimentation (ESV) reaches values around 50 mm1h, which are contemporaneous with the onset of the disease, with higher values in more severe cases, however they may be less expressive in milder cases and be modified to very high levels to low due to complications of the disease, such as congestive heart failure (CHF)
b) C-reactive protein, an anomalous protein that does not exist in normal blood, which precipitates with carbohydrate C from pneumococcus, is found in almost all rheumatic patients before the end of the second week of evolution of the acute condition, so that two negative determinations speak for themselves absence of RD - however, may disappear from serum prematurely with RD still present.
c) The measurement of mucoproteins can reveal high values in 95% of rheumatic patients and is parallel to the evolution of the condition in a similar way to α2-globulins, not being modified by the influence of medication and disappearing with the presumed cure of the disease. Maximum normal values are 4 mg% (tyrosine content) and 14.5 mg% (polysaccharide content)
3. Alterations found in serum protein electrophoresis – a slight decrease in albumin, elevation of α1-globulins and α2-globulins, in the initial and intermediate phases of RD, and of Ƴ-globulins, in a later phase, when it occurs more intense tissue alteration. Among us, this aspect is often found in RD, which makes it characteristic of the disease (Figure 2)
The modification that best suits the follow-up of a rheumatic patient is that of α2-globulins, since it is constant, seen from the beginning of the disease, changes according to the treatment and normalizes with the cure of RD.
The elevation of α1-globulins is very inconstant and transient.
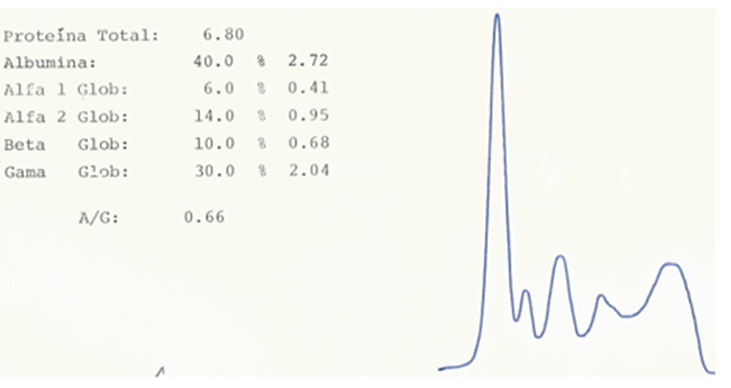
Figure 2´- Serum protein electrophoresis of a 12-year-old adolescent in the second rheumatic attack. Observe the increase in α2-globulins.
4. Electrocardiographic modifications –
Cardiac chamber overload are found, according to the severity and type of existing valve lesions. Regardless of the predominant type of injury, in acute RD we can register extrasystoles and, sometimes, decrease in QRS voltage in the frontal plane and its alternation exposing “pericardial effusion”, which is frequent in the disease.
Changes in the ST segment and T wave are not uncommon, as is also seen in other situations that produce peri-myocardial inflammation.
Indicators that have a certain specificity with rheumatic carditis are AV blocks, ranging from the first to the third degree, and QTc elongation.
First-degree AV block is found in 11% of patients, while QTc elongation is diagnosed in 28% of our acute rheumatic patients.
A relevant aspect amongst us is the “conjunction AV block and elongated QTc”, which is not rare (Figure 3)

Figure 3 - A 19-year-old male patient with his third rheumatic attack, the first having occurred at the age of 4-year-old. Note the prolonged PR interval (190 msec) and the also lengthened QTc (430) with the signs of overloading both atria.
The arrhythmias that are useful for diagnosing RD, especially in recurrences, are atrial fibrillation and isorhythmic AV dissociation (Figure 4)

Figure 4: Isorhythm AV dissociation in a 12-year-old boy in the first rheumatic attack, with mild damage to the mitral valve.
Treatment and prevention
treatment
1. Rest-it is essential, especially when severe carditis with CHF is present. Bed rest with an elevated headboard can, per se, reduce the intensity of the damage that the disease may produce in heart valves.
2. Extirpation of the streptococcus-assuming that the patient harbors bacterial cells in the pharynx, if the patient is hospitalized at an adult or weighing more than 20 kg, 1,200,000 IU of benzathine penicillin are applied intramuscularly, preferably on the buttocks, where the musculature is deeper; for patients weighing less than 20 kg, 600,000 units are used.
While the patient is hospitalized, the antibiotic will be given every 8 days, starting the prevention of the disease.
3. Arthritis - due to the excellent response of the joint inflammatory process, acetyl salicylic acid is used, at a dose of 80 to 100 mg per kg of weight, a maximum of 4 g per day, which is divided into four intakes. The attack lasts for about four or five days, when the drug is gradually reduced. Another very useful drug is ibuprofen.
4. Carditis - despite the controversies about the reduction or not of valve damage by hormonal anti-inflammatory drugs, for a long time, we use prednisone, for all forms of carditis, with an attack of 1 to 2 mg/kg, with a maximum dose of 80 mg, maintained for ten days, when the drug is gradually reduced by around 10 to 20% per week - in this way, there is coverage of the entire “rheumatic cycle”, which can reach 90 to 120 days.
It is not uncommon for the patient to develop a “Cushingoid aspect”, however, usually, this is a transitory finding, which gradually disappears, with real benefit from its use. The observation accepted by GHATI et al [27] in India, that the steroid reduces inflammation, resolves the toxic state, prevents the appearance of new murmurs and acts in the resolution of pericardial effusion, justifies its use.
By the way, the picture of a six-year-old patient, hospitalized with a great variety of symptoms and signs of severe RD, illustrates this fact. With complaints of uncoordinated movements in the left hemibody, arthritis of the right knee and exertional dyspnea, EAF she was admitted to the Pediatrics Unit of the Barão de Lucena hospital, with edema in the lower limbs, hepatomegaly with pain, jugular stasis at 45o and uncoordinated and aimless movements, making “grimaces”, with the mother fearful that the girl “would fall apart”.
On cardiac auscultation, with a heart rate of 130 beats/min, a protodiastolic gallop rhythm was perceptible, with a very intense holosystolic murmur in the mitral area, radiating to the back, indicating severe IM. She was medicated with prednisone (60 mg/day), diuretics (furosemide, 2md/day), oral digoxin, and haloperidol (0,5 mg/day, in increasing dose)), in addition to weekly injectable penicillin.
The attached Doppler echocardiogram was recorded during admission:

Figure 5: EchoDopplercardiogram of EAF, a 6 -years- old female Severe mitral regurgitation in an acute rheumatic condition, rich in symptoms and signs.
During follow-up, the mother religiously obeyed our instructions, including making the patient sleep in an isolated room, using benzathine penicillin every 15 days. After a long period of seven years, the mitral systolic murmur practically disappeared, being replaced by a clear mid-systolic click (Figure 6)

Figure 6: EAF, echoDopplercardiogram at age 13 - years-old. Note the marked reduction in mitral regurgitation, now considered mild, in the presence of thickened anterior leaflet prolapse.
Altogether, this case of EAF was the most beautiful we have seen, with almost complete resolution of the valve damage, which was so severe at the beginning.
Currently, the patient is a married woman and mother of two children!
a) Cardiac arrhythmias are not life threatening. Even the infrequent third-degree AV block tends to disappear with the use of anti-inflammatory drugs.
b) The rare "rheumatic pneumonia" [1], [23] , controversial but accepted by the Décourt`s School , is closely related to severe carditis. It usually appears in the lower third of the right lung and is revealed clinically by coughing with hemoptoics, tachypnea and drowsiness, concomitantly with severe congestive conditions, hence being confused with mere pulmonary congestion. It has a poor prognosis and is treated with corticosteroids.
c) The surgical treatment of the valve disease is based on the initial observations [28], showing an excellent response in cases of severe carditis, unresponsive to conventional therapy, to surgical treatment of mitral regurgitation, this technique started to be used in the presence of refractory CHF.
Prevention -
In the triad that produces acute RD – the host, the bacteria and the environment – it is clear that the only way to curb the disease is to change the environment in which the patients live. Caravetis et al [2] recently instituted what they call "primordial prevention", which fundamentally concerns changing homes that are incompatible with life, with the patient always having to sleep alone in a single bedroom.
In the absence of a vaccine to prevent new streptococcal pharyngeal infections, the only way to curb these infections is through "secondary prevention", which begins with the patient still hospitalized, as we have seen. The antibiotic of choice is benzathine penicillin, since after its discovery 70 years ago, until today, there is no streptococcal strain resistant to it; only in the presence of allergy to penicillin, we use other antibiotics or sulpha drugs, thus, oral penicillin itself – penicillin V 250 mg every 12 hours – or sulfadiazine, at a dose of 1 g/day orally for adults and 0.5 g/ PO day in children weighing less than 20 kg.
The ideal is the use of benzathine penicillin, thus, in patients weighing less than 20 kg, 600,000 IU are given every 15 days in the first two years, then, every 21 days; in patients weighing more than 20 kg, 1,200,000 IU of depot penicillin is used every 15 days in the first two years, then every 21 days.
Surgical correction of rheumatic valve disease constitutes the tertiary prevention [2] of the disease, maintaining the use of injectable benzathine penicillin throughout life.
How long is secondary prevention maintained?
- in the operated valve disease patient, for life;
- in patients with residual valve damage, up to the age of 40, or for life;
- RD with previous carditis, residual IM or resolution of the valve disease, up to 25 years or 10 years after the last attack, whichever covers the longer period;
- RD without previous carditis, up to 21 years or 5 years after the last outbreak, whichever covers the longer period.
The Current Scenario In The Poorest Countries
In the mid-twentieth century, with countries with greater economic support drastically reducing the incidence of RD and obtaining effective control of the disease, with great scientific data on the causative bacteria, better understanding of how the disease occurs and better living conditions and housing for victims of RD. At the same time, publications on RD have faded, especially in the United States.
Several years later, the discovery of subclinical carditis through Doppler echocardiography and the finding of a latent form of rheumatic heart disease, as well as the perennial search for an effective vaccine against the disease, which was so limiting, led once again to the production of excellent clinical research, coming mainly from Asia and Africa.
Subclinical valvitis was discovered by echoDoppercardiography. surprisingly, since it was recorded in children with normal cardiac auscultation. As we saw in LAPA's work, subclinical valvitis appears in silent subclinical cases as if it were a “micro-expression” of rheumatic fever, which is the most discreet and least aggressive form of rheumatic heart disease. We must keep in mind, however, that this form also results from the same immune reaction already discussed, therefore, the same assumptions accepted for the usual form, of “'macro-expression'”, should guide the clinician's conduct.
So, faced with a form that is also cardiologically silent, which is the latent form of rheumatic heart disease, what should we do? What is our conduct?
In 2014, the cohort study by BEATON et al [29], using Doppler echocardiography, initially showed the occurrence of rheumatic heart disease in asymptomatic patients, which they called latent, corresponding to children of school age, with no previous history of rheumatic outbreak and without symptoms, but with Doppler ultrasound revealing clear signs of rheumatic heart disease.
The follow-up of the 63 patients studied for two years revealed clinical stability in 91% of the cases, but in 10% there was a morphological alteration of the mitral valve with present MI, progressing to definitive rheumatic heart disease. In established rheumatic heart disease, improvement is difficult. According to BEATON et al [29], younger children, those with multiple abnormalities in the mitral valve apparatus and those who show higher titers of antistreptolysin O are the least likely to obtain improvement, even in the face of well-conducted secondary prophylaxis
On other hand, in populations at high risk for rheumatic heart disease, these subclinical changes are reasonably interpreted as signs of latent RHD.
The observations made by three great researchers of this serious disease - YUSUF, NARULA and GAMRA [30] - recognize that, in compliance with WHO recommendations implemented in poor countries, such as Cuba, Tunisia and Costa Rica, there was a significant drop in acute DR and rheumatic heart disease. In Tunisia, for example, which even doubled its population in a period of ten years, saw the reduction in the incidence of RD fall from 900 cases per year to nine cases per year.
The measures taken by the Central Government were:
1. Compulsory notification to the Ministry of Health;
2. Preferential use of benzathine penicillin to prevent disease recurrences;
3. Forwarding of surgical cases to centers specialized in cardiac surgery;
4. Nursing participation;
5. Promotion of decent housing of habitation with rheumatic patients sleeping in an isolated room.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
