AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Ankita Pandey, Department of radiotherapy and oncology, PGIMER, Chandigarh, India.
Citation: Ankita Pandey (2024), Radiotherapy in Hepatocellular Carcinoma – A Review of Literature, J. Cancer Research and Cellular Therapeutics, 8(3); DOI:10.31579/2640-1053/193
Copyright: © 2024, Ankita Pandey. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 April 2024 | Accepted: 22 April 2024 | Published: 29 April 2024
Keywords: hepatocellular carcinoma; radiotherapyo utcome
Our knowledge of how radiation affects primary and secondary liver tumours is still developing. Decades ago, radiation delivery methods that treated large numbers of patients also cautioned against using radiation for definitive and palliative care. Over time, the function of radiation therapy in the treatment of hepatocellular carcinoma has changed. New information regarding HCC therapy choices has been made possible by the capacity to administer a tumoradical dose to liver lesions while protecting the normal parenchyma surrounding them. The purpose of the review article is to cone down various treatment approaches that were traditionally used to treat hepatocellular carcinoma and the gradual adaptation of the radiation therapy to treat lesions that failed to respond to other therapies.
Cancer incidence rises dramatically with age, most likely due to an accumulation of risks for specific cancers that rise with age. The accumulation of overall risk is combined with the tendency for cellular repair mechanisms to become less effective as a person ages[1, 2]. The risk factors of cancer include tobacco use, alcohol consumption, poor diet, inactivity and air pollution are all risk factors for cancer and other non communicable diseases. Some chronic infections are cancer risk factors; this is especially prevalent in low- and middle-income countries. Carcinogenic infections such as Helicobacter pylori, human papillomavirus (HPV), hepatitis B virus, hepatitis C virus, and Epstein-Barr virus were responsible for approximately 13% of cancers diagnosed globally in 2018[3]. Between 30 and 50% of cancers can currently be prevented by avoiding risk factors and implementing existing evidence-based prevention strategies. The cancer burden can also be reduced through early detection of cancer and appropriate treatment and care of patients who develop cancer. Many cancers have a high chance of cure if diagnosed early and treated appropriately[4, 5] .
Liver cancer remains a global health challenge and its incidence is growing worldwide. It is estimated that by 2025 more than one million individuals will be affected by liver cancer annually. HCC is the sixth most common cancer and the fourth leading cause of death. One reason for the high mortality rate is the disease unknown pathogenesis as well as the lack of early diagnostic and prognostic biomarkers[6]. Hepatocellular carcinoma is one of the most common cancers in the world and it poses a significant global health-care challenge. Although viral hepatitis and alcohol continue to be risk factors for hepatocellular carcinoma, non-alcoholic fatty liver disease is quickly becoming the leading cause. The risk attributed to hepatitis C virus (HCV) infection has substantially decreased owing to patients achieving sustained virological response (SVR) with antiviral drugs. Nonetheless, patients with cirrhosis are still considered to be at high risk for HCC even after HCV clearance. Non-alcoholic steatohepatitis (NASH) is associated with metabolic syndrome or diabetes mellitus and is becoming the fastest growing aetiology of HCC, particularly in the West. Additionally, reports on mutational signatures have established aristolochic acid and tobacco as potential pathogenetic cofactors in HCC[7].
Hepatocellular carcinoma is one area of oncology warranting further investigation into its epidemiology. Although, HCC is one of the first cancers to be linked epidemiologically to a definite risk factor (hepatitis B virus in Taiwan); the explanation for what accounts for the incidence of this disease is less clear. Although liver cancer is the sixth most common neoplasm worldwide, it carries poor prognosis which makes it the third leading cause of cancer-related mortality and is responsible for nearly 600,000 deaths annually. In most countries, HCC accounts for 70%–85% of primary liver cancer cases, with the burden of disease expected to increase in coming years[8].
The molecular pathogenesis of HCC differs depending on the genotoxic insults and aetiologies. Despite advances in our understanding of disease pathophysiology and drivers, this knowledge has yet to be translated into clinical practise. Approximately 25% of HCC tumours have actionable mutations; however, the prevalence of most mutations is 10%, making proof-of-concept studies difficult. Indeed, TERT, TP53, and CTNNB1 remain unsolvable mutational drivers in HCC[9].
HCC is typically diagnosed using non-invasive criteria, though there is a growing need in clinical practise for molecular characterization of the tumour using tissue biopsies. In terms of prevention, in addition to HBV vaccines and anti-viral therapies for HBV and HCV infection, cumulative data support the preventive role of coffee and aspirin. HCC management has significantly improved since the early 2010. Curative treatments for HCC have traditionally included hepatic resection and liver transplantation. Patients with hepatocellular carcinoma have a variety of treatment options, including liver transplantation, surgical resection, percutaneous ablation, and radiation, as well as trans arterial and systemic therapies. Refinements in patient selection have resulted in enhanced surgical resection outcomes and remarkable 10-year post-liver transplantation survival rates for tumours down-staged beyond Milan criteria[10].
Local ablation with radiofrequency remains the backbone of image-guided ablation for non-surgical early-stage HCC, despite progress in other techniques. Adjuvant therapies to preclude relapse, following these potentially curative approaches, are an unmet medical need, as randomized controlled trials (RCTs) have so far yielded negative results. For intermediate-stage HCC, transarterial chemoembolization (TACE) has been the most widely used treatment and the standard of care over the past two decades. As a result, clinical decision making necessitates a multidisciplinary team that adapts the individual treatment strategy over time based on the patient's tumor stage, liver function, and performance status. The treatment landscape for advanced hepatocellular carcinoma is more diverse than ever, thanks to the approval of new first- and second-line agents, as well as the acceptance of immune checkpoint inhibitor-based therapies as standard of care[11].
A systematic literature search was undertaken using the PubMed data base and secondary references to identify peer-reviewed articles that reported clinical outcomes in HCC after external beam RT alone or in combination with other treatments. More than 70 articles were identified and collected for the review article to identify the probable outcome of unresectable HCC patients after RT.
Local liver RT in unresectable HCC
The role of RT in HCC has not been defined in curative setting due to low tolerance of liver in a range of 30-35Gy, which is much less than the therapeutic dose. This much dose can lead to hepatomegaly, ascites, elevated liver enzymes and is due to veno-occlusive disease secondary to the fibrosis[12]. Because of this reason, unresectable HCC are mainly treated with more efficacious treatment modality that includes TACE. However, single setting of TACE may be not sufficient to completely eradicate the tumor. Due to dual blood supply, these tumors may grow in between the TACE sessions that may lead to reduced efficacy of this most commonly used method for unresectable HCC. To address this issue Seong J et al in 1999, combined TACE with RT in these patients. They reported that this method is well tolerated and leads to substantial decrease in size of the tumor [13]. To further expand the role of RT, in 2000 the authors published their experience on Local radiotherapy for unresectable hepatocellular carcinoma[14]. The purpose of their study was to investigate the efficacy of local radiotherapy (RT) as a salvage treatment for unresectable hepatocellular carcinoma (HCC) patients who failed with transcatheter arterial chemoembolization (TACE). TACE failure was determined based on incomplete lipiodol-Adriamycin mixture tumour filling either on angiography or computed tomography (CT) scan. From January 1993 to December 1997, 27 patients who had UICC Stage III (17) or IVA (10) disease entered into this study. Local RT was delivered with a mean tumour dose of 51.8 ± 7.9 Gy, in daily 1.8-Gy fractions using a 6 - 10MV linear accelerator. 66.7% patients had objective response including one with complete response. Intrahepatic and extrahepatic metastasis was seen in 10 and 4 patients, respectively. Survival rates at 1, 2, and 3 years were 85.2%, 58.1%, and 33.2%, respectively, from the diagnosis and 55.9%, 35.7%, and 21.4%, respectively, from the start of RT. The median survivals were 26 months from the diagnosis and 14 months from the start of RT. Acute toxicity included changes in liver function tests in 13 patients and thrombocytopenia in 2 patients. Subacute and chronic toxicity involved gastroduodenal ulcer (3 patients) and duodenitis (2 patients). No treatment-related deaths were seen. Authors concluded that in local RT caused a significant tumour response of 66.7% in unresectable HCC patients who failed TACE, with a 3-year survival rate of 21.4% and a median survival period of 14 months.
As the median dose of 51.8Gy was reported to be well tolerated in a mean tumor volume of 7.2±2.9cm, Laura A Dawson et al (2000) conducted research on Escalated Focal Liver Radiation and Concurrent Hepatic Artery Fluorodeoxyuridine for Unresectable Intrahepatic Malignancies[15]. In this phase I trial, the objective was to evaluate the response, time to progression, survival, and impact of radiation (RT) dose on survival in patients with intrahepatic malignancies. A total of 43 patients with either unresectable intrahepatic hepatobiliary cancer (HB; 27 patients) or colorectal liver metastases (LM; 16 patients) were treated with high-dose conformal RT with a median dose of 58.5 Gy (range, 28.5 to 90 Gy), 1.5 Gy twice daily, with concurrent continuous-infusion hepatic arterial fluorodeoxyuridine (0.2 mg/kg/d) during the first 4 weeks of RT. The median tumour size was 10 × 10 × 8 cm. Authors reported the response rate in 25 assessable patients to be 68% (16 partial and one complete response) and the median times to progression for all tumours, LM, and HB as 6, 8, and 3 months, respectively. The median survival times of all patients, patients with LM, and patients with HB were 16, 18, and 11 months, respectively. On multivariate analyses, improved progression-free and overall survival was associated with escalated RT dose. The median survival of patients treated with 70Gy or more was not reached (16.4+ months), while median survival in patients with lower dose RT was 11.6 months (p = .0003). Authors concluded that the excellent response rate, prolonged intrahepatic control, and improved survival in patients treated with RT doses of 70Gy or more motivate continuation of dose-escalation studies for patients with intrahepatic malignancies.
Cheng et al (2001) evaluated outcome, failure pattern and toxicity in patients with unresectable HCC treated with radiotherapy(n=9), TACE +RT (n=17) or TACE (n= 16) alone [16]. Mean RT dose was 46.9±5.8Gy in 1.8 to 2Gy daily fraction. TACE was performed using combination of lipiodal, doxorubicin, mitomycin C and cisplatin followed by Gelfoam or Ivalon embolisation. Worst survival was seen in RT alone group while TACE +RT and TACE treated patients had comparable 2 year survival rate of 58% and 56% respectively. Although intrahepatic recurrences outside the treated tumor were common and similar in these two groups, the extrahepatic progression free survival was significantly shorter in TACE+RT patients (2year rates: 36% in TACE+RT and 100% in TACE). One of the reason behind inferior outcome in RT alone patients were due to selection bias wherein advanced disease and compromised patients were included in this group. Authors concluded that local RT may be added to unresectable HCC that may result in control of progression of treated tumor even of larger size. Compared to previous two studies, the mean RT dose in this study was much lower.
Laura A Dawson and Chandan Guha (2004) in their review Hepatocellular carcinoma: radiation therapy[17] stated thatalthough whole liver tolerance to radiation therapy (RT) is low, hepatocellular carcinoma (HCC) can be treated with focal high-dose RT, using a variety of advanced and specialized treatment strategies like conformal RT planning, breathing motion management, and image-guided RT. Apart from this, use of charged particles that have a property of desirable dose distributions allowing tumoricidal doses to be delivered with sustained tumour control and little toxicity, even in the presence of Child-Pugh class B or C cirrhosis can also be used. Another strategy is hepatic arterial delivery of radioisotopes, such as microspheres tagged with yttrium-90. Hence, a more advanced form of RT techniques can help to deliver high dose to tumor with reduced and manageable radiation induced liver injury.
Similar study evaluating role of RT in HCC with portal vein or inferior vena cava tumor thrombi was conducted by Zhao Chong Zeng et al in 2005[18]. Forty-four patients received local limited EBRT (in addition to other treatment modalities) to a total radiation dose of 36-60 Gy (median, 50 Gy) and was focused on the tumour thrombi. One hundred fourteen patients with HCC who did not receive EBRT were classified as the non-EBRT group, and were treated with transarterial chemoembolization or resection, based on the patients' status. Of the 44 patients who received EBRT, 15 (34.1%) showed complete disappearance of tumour thrombi, 5 (11.4%) were in partial remission, 23 (52.3%) were stable in their tumour thrombi, and 1 (2.3%) showed disease progression at the end of the study period. The median survival was 8 months and 1 year in EBRT and non- EBRT group, respectively. In the EBRT group, poorer prognosis was significantly related to intrahepatic multifocal or diffusion lesions, and the most common reason for death was liver failure caused by uncontrolled intrahepatic disease. They concluded that although EBRT is palliative in intent, it is preferred for prolonging survival in the treatment of tumour thrombi.
Hani Soliman (2013) in Toronto evaluated the feasibility and response of liver radiotherapy (RT) in improving symptoms and quality of life in patients with hepatocellular carcinoma (HCC). Forty-one patients (30 men and 11 women) with HCC (n = 21) or liver metastasis (n = 20) with an index symptom of pain, abdominal discomfort, nausea, or fatigue were included in the trial. The Brief Pain Inventory (BPI), Functional Assessment of Cancer Therapy–Hepatobiliary (FACT-Hep), and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire C30 (EORTC QLQ-C30) were completed by patients at baseline and each follow-up. The primary outcome was the percentage of patients with a clinically significant change at 1 month in the BPI subscale of symptom on average in the past 24 hours. Secondary outcomes were improvement in other BPI subscales and at other time points, FACT-Hep and EORTC QLQ-C30 at each follow-up, and toxicity at 1 week. At 1 month, 48% had an improvement in symptom. Improvements in the FACT-G and hepatobiliary subscale were seen in 23% and 29% of patients, respectively, at 1 month. There were also improvements in EORTC QLQ-C30 functional (range, 11% to 21%) and symptom (range, 11% to 50%) domains. Authors concluded that improvements in symptoms were observed at 1 month in a substantial proportion of patients[19].
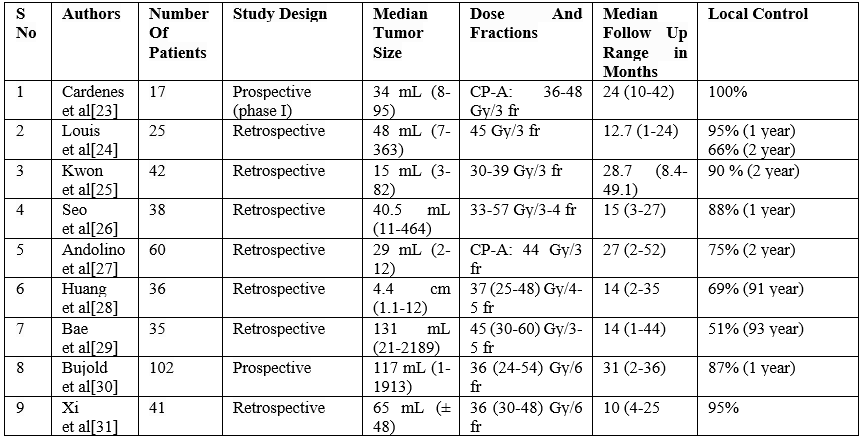
Table 1: Other Similar Studies In role of Stereotactic Body Radiotherapyin Hepatocellular cancer
Palliative Radiotherapy in Hepatocellular Carcinoma
External beam radiation therapy (EBRT) has historically only been used to treat HCC metastases that cause bothersome symptoms. External beam radiation therapy has been reported to be successful in treating metastases to the bone, lymph nodes, and soft tissues. For a very long time, HCC has been regarded as a radioresistant cancer[20]. Given that radiation-induced liver damage begins at a dose of 30 Gy, the whole liver could not receive more than this from traditional external beam radiation therapy. This dose level, however, is significantly lower than the typical doses of tumour radicals for the majority of solid cancers. Dose escalation is now possible thanks to technological advancements in radiotherapy precision delivery and normal tissue sparing. Regardless of the location of the tumour, radiation therapy is becoming more and more popular in the treatment of patients with advanced-stage HCC, and the outcomes are encouraging. Stereotactic body radiation or conformal high dose radiation therapy, has become a viable local treatment option for unresectable hepatocellular carcinoma. Numerous studies showed that the majority of patients had tumour control at one and two years. However, many patients are not appropriate candidates for high dose radiation due to the severe liver involvement associated with malignancy, borderline liver function, and/or the existence of extra-hepatic metastases. Radiotherapy has long been utilised to treat painful symptoms resulting from HCC metastases in a palliative situation. The most typical locations of extrahepatic metastatic
HCC include the lung, the abdominal lymph nodes, and the bones. There have also been reports in the literature of unusual metastatic locations, like the central nervous system[21]. HCC lymph node metastases are sensitive to EBRT within a dose range of 8-60 Gy. A dose of 50 Gy in 25 fraction was shown to be an effective palliative treatment for lymph node metastases in the Zeng et al series; nevertheless, survival declines with increasing lymph involvement distance from the liver due to the normal flow of lymph. The incidence of death resulting from lymph node-related complications was lower in the EBRT group in comparison to patients not receiving RT[22].
The use of radiation therapy to treat hepatocellular carcinoma has changed over time. The capacity to administer a tumoradical dosage to liver lesions while preserving the normal parenchyma around them has opened up new avenues for HCC treatment. Despite the long-held belief that HCC is a radioresistant cancer, the evidence supports the effectiveness and safety of radiation therapy for this condition. In terms of local control and survival, radiation treatments—either used alone or in conjunction with other local therapies like radiochemoembolization—show encouraging results. After a successful shift from radiotherapy's palliative role in HCC, we are now in a new era when patients who are not candidates for other therapeutic techniques can benefit from radiotherapy as an effective treatment.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
